
Abstract
Abstract
Background:
Procalcitonin (PCT) has been considered a more reliable marker than others because of its specificity for bacterial infection.
Methods:
Case report and review of the literature.
Results:
A 50-year-old male was diagnosed with subarachnoid hemorrhage, intraventricular hemorrhage, and intracerebral hemorrhage. We performed a ruptured aneurysm clipping and left unilateral external ventricular drainage. We also performed ventriculoperitoneal (VP) shunt placement in the course; however, VP shunt infection was indicated by fever, increased C-reactive protein concentration and leukocytosis. The cerebrospinal fluid culture showed methicillin-resistant Staphylococcus epidermidis but the serum PCT concentration was quite low.
Conclusions:
Although PCT is considered a more reliable serological marker of bacterial meningitis in several reports, the serum PCT concentration did not reflect the bacterial VP shunt infection that was present in our case.
Procalcitonin (PCT) is considered a more reliable serological marker of bacterial meningitis because of its specificity for bacterial infection [3–6]. Procalcitonin is a calcitonin propeptide and is believed to be synthesized in C cells of the thyroid gland and secreted from leukocytes. The secretion of PCT increases in response to endotoxins or mediators that are released following bacterial infections (interleukin [IL]-1β, tumor necrosis factor-α, and IL-6), and its concentration correlates strongly with the severity of bacterial infection [7]. It has been suggested that serum PCT concentrations increase during the course of bacterial, parasitic, or fungal infections but remain relatively normal in viral infections and inflammatory reactions without infection [7,8]. For this case, we measured PCT concentrations, in addition to CRP concentrations, WBC counts, and cerebrospinal fluid (CSF) cytochemical profiles, in order to detect a VP shunt infection.
Case Report
A 50-year-old comatose male was diagnosed with subarachnoid hemorrhage, intraventricular hemorrhage (IVH), and intracerebral hemorrhage (ICH). The rupture of an anterior communicating artery aneurysm was causative. We performed aneurysm clipping and external ventricular drainage on day 0. After the surgery, fever persisted. We started treatment with ceftriaxone (CTX; 2 g/d) for the prevention of infection. The drain was removed on day 25. CRP concentrations, WBC counts, CSF findings, and CSF cultures were all non-specific, and we stopped CTX. However, we had to restart CTX due to high fever on day 28. On day 33, the serum PCT concentration was 0.05 ng/mL.
The patient became stuporous with an expansion of the ventricle after the removal of the drain. We performed VP shunt placement on day 44 in confirmation of normal CRP, WBC, and CSF findings. On day 51, we found methicillin-resistant Staphylococcus epidermidis (MRSE) in the CSF culture that was submitted during the VP shunt operation and we started vancomycin (3 g/d). On day 53, the patient had septic shock and high fever. Both CRP and WBC concentrations were increased but the PCT concentration was 0.11 ng/mL (Fig. 1). We started biapenem (0.9 g/day) because VP shunt infection was suspected.
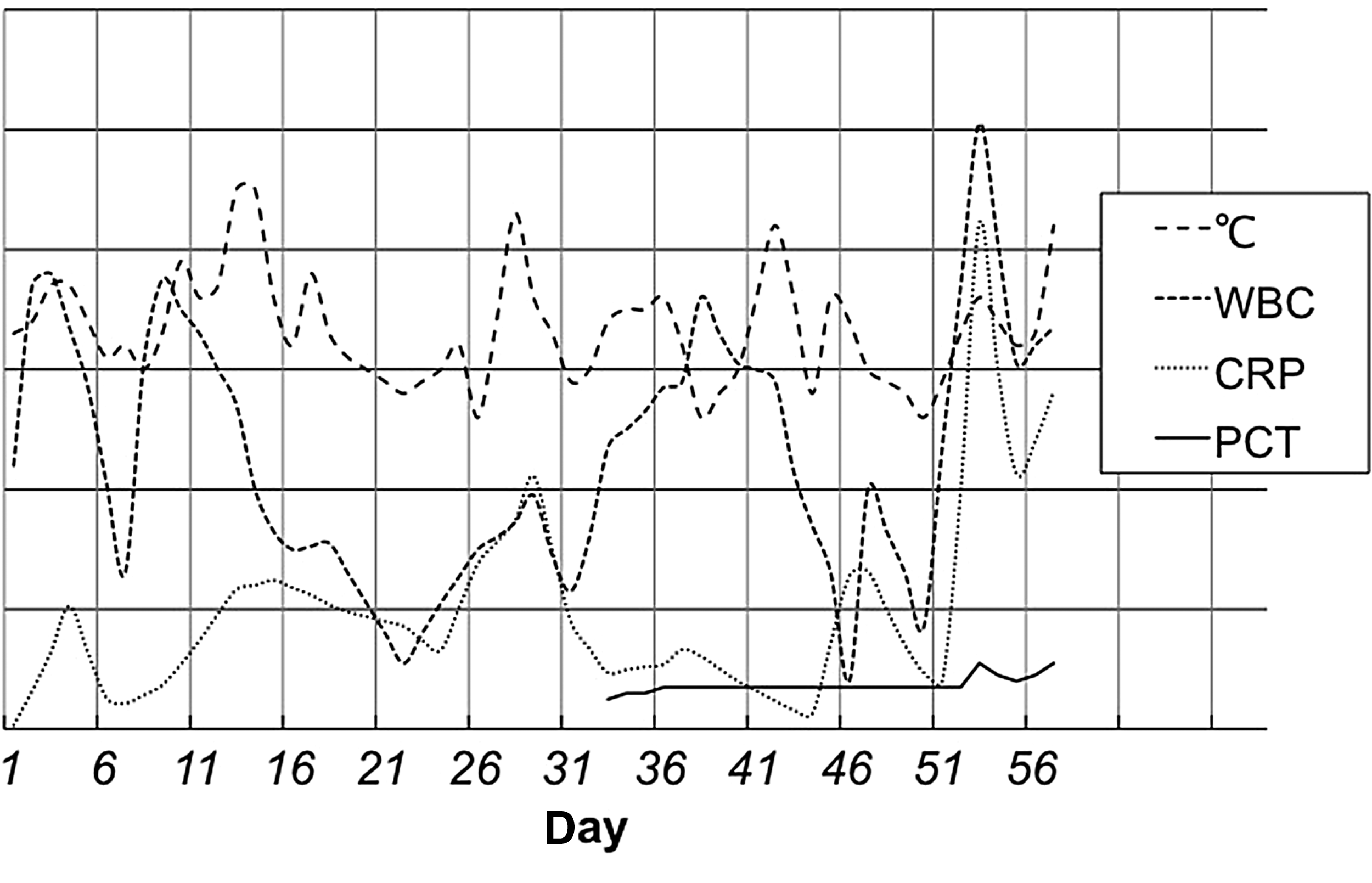
This line chart shows the trends of fever, white blood cell (WBC) counts, C-reactive protein (CRP) concentrations, and procalcitonin (PCT) concentrations. Both CRP concentrations and WBC counts were elevated at the time of the ventriculo-peritoneal shunt infection on days 53 to 57, but PCT concentrations changed only slightly and remained low.
On days 56 to 57, head computed tomography indicated shunt failure. The CSF findings showed a WBC count of 1,290/mcL (monocytes, 110; neutrophils, 1,180), a protein concentration of 180 mg/dL, and a glucose concentration of 7 mg/dL. The CRP concentration was 14.08 mg/dL, and the WBC count was 12,700 cells/mcL (Figs. 1 and 2). All of these findings indicated VP shunt infection. However, PCT remained low at 0.11 ng/mL.

This line chart shows the trends of fever, cerebrospinal fluid (CSF) cell counts, CSF protein concentrations, CSF glucose concentrations, and procalcitonin (PCT) concentrations. Both CSF cell counts and CSF protein concentrations were increased dramatically, and CSF glucose concentrations dropped at the time of the ventricular peritoneal shunt infection on days 53 to 57. However, PCT concentrations changed only slightly and remained low.
We removed the VP shunt. A CSF culture at that time was positive again for MRSE. The patient's fever, CSF findings, CRP concentration, and WBC count improved rapidly. The VP shunt was replaced after resolution of the infection, and the patient recovered, regaining full consciousness.
Discussion
Fever is a common response in intracranial hemorrhage; ICH and IVH often cause fever for long periods for reasons that do not involve infection (i.e., inflammatory reactions, brain injury, or thermoregulation deficits). The differentiation of VP shunt infection fever from other causes of inflammation after ICH and IVH is difficult. The most frequently used biomarkers for shunt infection are CRP, WBC, and CSF findings. However, CRP and WBC usually cannot discriminate between infections and inflammatory reactions [9]. Cultures of CSF and gram stains are the most reliable tests for diagnosing bacterial infection.
One of the serological indicators used most commonly is PCT, which has been shown in several reports to have sufficient specificity in the diagnosis of bacterial meningitis [3–6]. Nine articles were found that reported on PCT as an early diagnostic marker for bacterial meningitis, and Table 1 summarizes these publications. Viallon et al. demonstrated that one of the most discriminating parameters for the diagnosis of bacterial meningitis is PCT, which in a study of 254 patients, had a sensitivity of 95%, a specificity of 100%, a negative predictive value of 100%, and a positive predictive value of 97% at a diagnostic cutoff value of 0.28 ng/mL [6]. In another study of children of meningitis, Alkholi et al. reported that serum PCT with cutoff values higher than 2 ng/mL showed sensitivity, specificity, positive predictive value, and negative predictive value of 100%, 66%, 68%, and 100%, respectively, for the diagnosis of bacterial meningitis [3]. Laifer et al. reported the usefulness of serum PCT after major neurosurgery in the diagnosis of post-operative fever due to infection [10]. Berger et al. reported the role of PCT in patients with bacterial cerebral ventricular infections after the insertion of external ventricular drains. Concentrations of PCT higher than 1 ng/mL seem to be the best for indicating and predicting bacterial ventriculitis [9]. Although several reports have suggested the usefulness of PCT in the diagnosis of ventricular drainage infections, we were unable to find any previous reports about the usefulness of PCT for the diagnosis of VP shunt infections.
CDC=U.S. Centers for Disease Control and Prevention; CSF=cerebrospinal fluid; PCT=procalcitonin; BM=bacterial meningitis.
Most intracranial prosthetic device infections are caused by S epidermidis and other coagulase-negative staphylococci (CoNS), Staphylococcus aureus, and less commonly, nosocomial gram-negative bacilli and yeasts [10–14]. A small study showed a low sensitivity for PCT in the diagnosis of bacterial meningitis in adults, especially for nosocomial bacterial meningitis following neurosurgery [15]. The authors of that study suggested that PCT is of limited diagnostic value in adults with bacterial meningitis, especially in cases of nosocomial origin, but PCT was higher with typical meningitis agents (pneumococci and meningococci) in their report. Martinez et al. reported that PCT concentrations usually remain within the normal range even in the presence of a positive bacterial culture in patients with ventriculitis and ventricular catheters [16]. They suggested that ventricular catheter-related ventriculitis is a circumscribed infection without systemic involvement.
Although VP shunt infections seem to cause more expanding infections and higher PCT concentrations than ventricular drainage—including meningitis, peritonitis, and subcutaneous infections—PCT concentrations in our case were consistently far below the diagnostic cutoff values described in several reports.
We suggest two hypotheses for the low PCT concentrations in our VP shunt infection case. First, this VP shunt infection is a circumscribed infection without systemic involvement, but septic shock on day 53 in our case was considered compatible with systemic involvement. Second, S. epidermidis and other CoNS, which are the major cause of VP shunt infections, is not suitable for monitoring by PCT because of its attenuated systemic virulence.
It is difficult to estimate reliability of PCT in VP shunt infection by this single case. Our case report is unique in that PCT was totally impractical, although CRP, WBC, and CSF findings reflected the severity of the infection. More experiences may be needed to estimate usefulness of serum PCT in VP shunt infection.
Footnotes
Author Disclosure Statement
No competing financial interests exist.