
Abstract
Abstract
Background:
Chemotherapy remains a mainstay of treatment for cancer patients. However, anti-cancer drugs frequently cause a wide range of side effects, including leukopenia and gastrointestinal toxicity. These adverse effects can lead to treatment delays or necessitate temporary dose reductions. Although chemotherapy-related changes in gut morphology have been demonstrated, the influences of chemotherapeutic regimens on gut immunity are understood poorly. This study aimed to examine whether the anti-cancer drug paclitaxel (PTX) impairs gut immunity in mice.
Methods:
Male ICR mice were randomized into three groups: Control, low-dose PTX (low PTX; 2 mg/kg), or high-dose PTX (high PTX; 4 mg/kg). A single intravenous dose was given. On day seven after the injection, lymphocytes from Peyer patches (PP), intraepithelial (IE) spaces, and the lamina propria (LP) were counted and analyzed by flow cytometry (CD4+, CD8+, αβTCR+, γδTCR+, B220+). Immunoglobulin A (IgA) concentrations were measured in small intestinal and respiratory tract washings.
Results
: Total, CD4+ and γδTCR+ lymphocyte numbers in PPs were significantly lower in the high PTX than in the control group. The CD4+ lymphocyte numbers in the IE spaces were significantly lower in both PTX groups than in the control group. Respiratory tract IgA concentrations were lower in the high PTX than in the control group.
Conclusion:
The present data suggest high-dose PTX impairs mucosal immunity, possibly rendering patients more vulnerable to infection. Careful dose selection and new therapies may be important for maintaining mucosal immunity during PTX chemotherapy.
P
However, PTX frequently causes severe side effects, which may include a low white blood cell count, weakness, infections, and muscle pain, as well as numbness, tingling, and burning sensations of the extremities; i.e., neuropathy. Gastrointestinal toxicities reported in patients treated with PTX include neutropenic enterocolitis, bowel obstructions/perforations, pseudomembranous colitis, mucositis, and ischemic colitis [5–8]. These side effects limit the dose of PTX that can be given safely. Although changes in gut morphology induced by PTX-based chemotherapy have been demonstrated [9–11], the influences of chemotherapeutic regimens on gut immunity are poorly understood. If GI injury induced by PTX impairs gut immunity, PTX may allow bacterial infection and thereby predispose patients to serious infection. Elucidation of the adverse effects of PTX on gut immunity is thus an important research goal.
Gut-associated lymphoid tissue (GALT) has been considered a center of mucosal immunity because of its mass and function [12]. Anatomically, GALT is composed of organized lymphoid structures and diffusely distributed cell populations, such as intraepithelial (IE) and lamina propria (LP) lymphocytes. Organized GALT consists of Peyer patches (PP), which are regarded as the primary mucosal immune-inductive sites and sources of immunoglobulin (Ig) A-secreting cells. Once naïve lymphocytes have migrated into PP, they are sensitized and stimulated through interaction with dendritic cells and migrate to mesenteric lymph nodes, where they mature, proliferate, or both. After release into the thoracic duct, these lymphocytes are distributed by the vascular system to GALT effector (the LP and IE space) and extraintestinal sites.
This study examined whether PTX impairs gut immunity in mice. We examined the effects of a single intravenous dose of PTX on GALT (PP, LP, and IE) lymphocyte numbers, GALT cell phenotypes, and the secretory IgA concentration. Pathologic examination of the intestine also was performed.
Materials and Methods
Animals
The studies described herein conformed to the Guidelines for the Care and Use of Laboratory Animals established by the Animal Use and Care Committee of the National Defense Medical College. Male Institute of Cancer Research (ICR) mice, five weeks of age, were purchased from Japan SLC Inc (Hamamatsu, Japan). The ICR mouse is a standard strain for testing the toxicity, pharmacokinetics, and influences of drugs. In addition, many experimental studies focusing on the influences of nutrition on gut immunity in these animals have obtained results compatible with human clinical data. This strain has been used widely for evaluating gut immunity [13–15].
The mice were housed under controlled temperature and humidity conditions with a 12-h:12-h light:dark cycle. For acclimation, mice were fed commercial mouse chow (CE7, Clea, Japan) with water ad libitum for one week before protocol entry.
Surgical procedure
After the mice had been fasted overnight, they were given general anesthesia (ketamine 100 mg/kg and xylazine 10 mg/kg) and randomized into three groups: Control (n=18), low-dose PTX (low PTX; n=22), or high-dose PTX (high PTX; n=24). All mice underwent implantation of silicon rubber catheters (0.3 mm inner and 0.5 mm outer diameter; Imamura Co., Tokyo, Japan) into the right jugular vein to assure intravenous (IV) administration of PTX. The proximal end of the catheter was tunneled subcutaneously over the spine and exited the tail at its midpoint. After these procedures, the mice were placed in individual metal metabolism cages and partially immobilized by tail restraint to protect the catheter during infusion. This technique is a well-established method that induces neither physical nor biochemical stress [16]. All procedures were performed aseptically. Catheterized mice were connected immediately to infusion pumps (TE331; Terumo, Tokyo, Japan) and received physiologic saline at 0.2 mL/h for 48 h with ad libitum access to chow and water.
Infusion protocol
The control group received a continuous IV infusion of physiologic saline at 0.2 mL/h throughout the study period with free access to chow and water (Fig. 1). On postoperative day 2, a single IV dose of PTX (Bristol Myers Squibb, Tokyo, Japan) was given to the low- (2 mg/kg) and high-dose (4 mg/kg) PTX groups. After the injection, the mice continued to receive saline at 0.2 mL/h throughout the study period with free access to chow and water.

Experimental protocol. All mice received a saline infusion with free access to chow and water. Mice were given low or high paclitaxel (PTX) doses intravenously at 2 mg/kg or 4 mg/kg, respectively. GALT=gut-associated lymphoid tissue.
At seven days after the injection, all mice were anesthetized (ketamine 100 mg/kg and xylazine 10 mg/kg) and exsanguinated by cardiac puncture. Complete blood cell counts were performed. Nasal and bronchoalveolar washings were obtained by lavage with 1 mL of phosphate-buffered saline. The entire small intestine was harvested and flushed with 20 mL of chilled Hank balanced salt solution (HBSS). The washings were stored in a −80°C freezer for later IgA analysis.
Peripheral blood-cell counts
Total numbers of leukocytes and the hemoglobin concentrations in the peripheral blood were measured with a hemocytometer (PCE-210; Erma Inc, Tokyo, Japan).
Cell isolation
Lymphocytes were isolated from the GALT using a modification of the method described by Li et al. [13]. The PP were examined as an inductive tissue for mucosal immunity. Lymphocytes of the IE space and LP were chosen as gut mucosal immunity effector sites.
Peyer's Patches
The PP were excised from the serosal side of the intestine and teased apart. The fragments were treated with collagenase (40 U/mL; Sigma, St. Louis, MO) in Roswell Park Memorial Institute (RPMI) 1640 medium for 60 min at 37°C, with constant shaking. After collagenase digestion, the cell suspensions were passed through nylon filters.
Intraepithelial space and lamina propria
After PP excision, the intestine was turned inside out and cut into four segments. The segments were incubated with RPMI 1640 containing 5% fetal bovine serum (FBS), 1% glutamine, and a 1% antibiotic mixture (penicillin and streptomycin; GIBCO, Auckland, New Zealand), for 45 min at 37°C in a water shaker (150 rpm). Supernatant liquids containing released sloughed epithelial cells and IE lymphocytes were stored on ice. The remaining tissue pieces were incubated three times, 45 min each time, with RPMI 1640 containing collagenase (40 U/mL; Sigma), 5% FBS, glutamine, and the antibiotic mixture at 37°C at 150 rpm in a water shaker. Supernatant liquids containing LP cells from each of the incubations were pooled on ice. Supernatant liquids were filtered through a glass wool column. Suspensions were centrifuged, the pellets were resuspended in 40% Percoll (Pharmacia, Piscataway, NJ), and the cell suspensions were overlaid on 75% Percoll. After centrifugation for 20 min at 600×g at 25°C, viable lymphocytes were recovered and washed in RPMI 1640. The lymphocytes were resuspended in RPMI 1640 with 5% FBS, 1% glutamine, and the 1% antibiotic mixture and then counted. This procedure yields a cell population that is 95%–100% viable by trypan blue exclusion.
Flow cytometry
Lymphocytes (1×105) isolated from PP, the IE space, and the LP were suspended in 50 mcL of HBSS containing fluorescein isothiocyanate (FITC) anti-mouse γδ T-cell receptor (TCR) (clone GL3; Caltag, Burlingame, CA) and phycoerythrin (PE)-conjugated antimouse βTCR (clone H57–597; Pharmingen, San Diego, CA) to identify γδTCR+ T and αβTCR+ T cells, respectively, or PE-anti-CD4 (clone CT-CD4; Caltag) and either FITC-anti-CD8α (clone CT-CD8a; Caltag) to identify the two T-cell subsets or FITC-anti-CD45R (B220; clone RA3–6B2; Caltag) to identify B cells. All antibodies were diluted to 1 mcg/mL in HBSS containing 1% FBS. Incubations were carried out for 30 min on ice. After staining, the cells were washed twice in HBSS/1% FBS and fixed in 1% paraformaldehyde. Flow cytometric analyses were performed on an Epics XL (Coulter, Inc., Hialeah, IL).
IgA quantification
Immunoglobulin A was measured in intestinal, nasal, and bronchoalveolar washings in a sandwich enzyme-linked immunosorbent assay using a polyclonal goat anti-mouse IgA (Sigma) to coat the plate, a purified mouse IgA (Zymed Laboratories, San Francisco, CA) as the standard, and a horseradish peroxidase–conjugated goat anti-mouse IgA (Sigma).
Histologic examination
To assess the influences of PTX on gut morphology, tissue sections of intestines collected from another set of mice (control: n=2, low PTX: n=3, high PTX: n=3) were examined. The harvested intestine was cut into three sections, and each piece was fixed by immersion in 10% buffered formalin. For light microscopy, tissue samples were embedded in paraffin, sectioned, and stained with hematoxylin and eosin (H&E).
Statistical analysis
All data are expressed as the mean±standard error of the mean for each group. Statistical significance was determined using analysis of variance (ANOVA) followed by the Fisher protected least-significant difference post-hoc test. Differences were considered significant at p<0.05. All statistical calculations were performed with SPSS Software for Windows (SPSS, Inc., Chicago, IL).
Results
Body weight
There were no significant differences in body weight in the three groups at the beginning of the experiment (mean 32.1±1.3 g [standard error] control; 31.5±1.5 g low-PTX; 31.6±1.4 g high-PTX).
Blood cell count
There were no significant differences in complete blood cell counts, including white blood cell counts and hemoglobin concentrations, among the three groups (Table 1).
Body weight change and food intake
We found no significant difference in body weight change or daily food intake among the three groups during the seven days after PTX injection (Fig. 2).
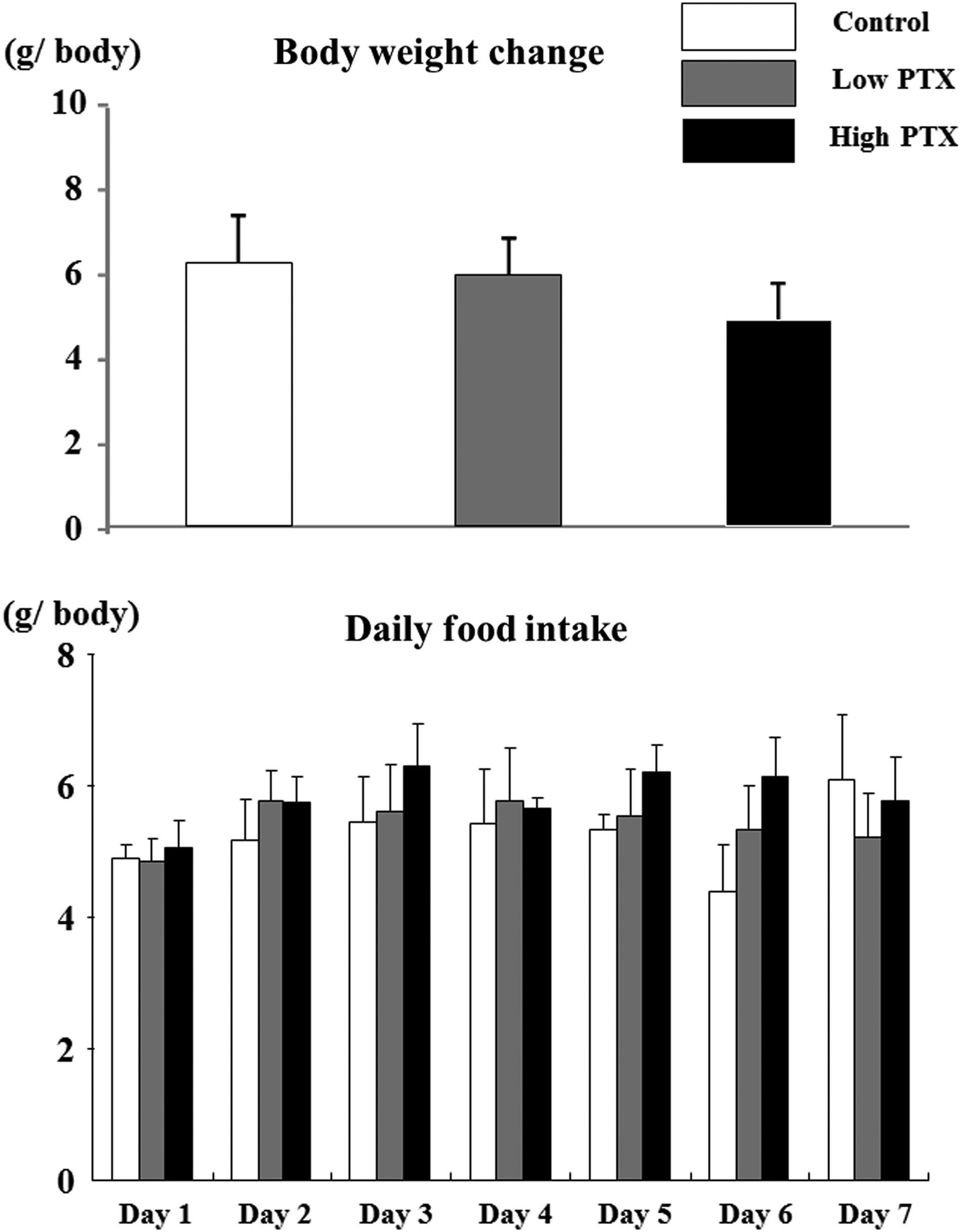
Body weight changes and daily food intake. Values are means±standard error. PTX=paclitaxel.
Total cell yields from GALT
The PP lymphocyte numbers were significantly lower in the high-PTX than in the control group (Fig. 3). The low-PTX group was midway between the control and high-PTX groups. The numbers of lymphocytes isolated from the IE and LP did not differ significantly among the three groups.
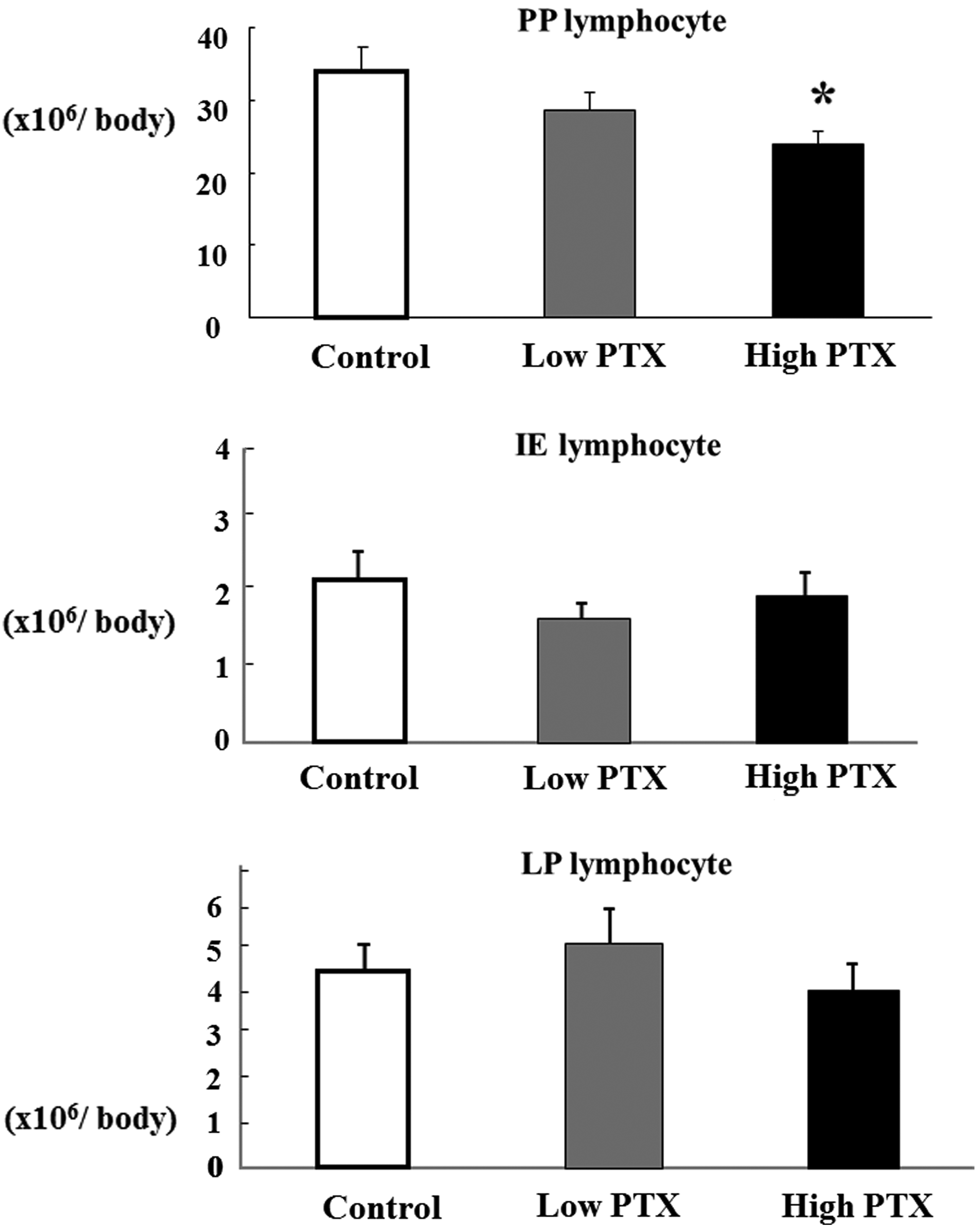
Total cell yields from gut-associated lymphoid tissue (GALT). Values are means±standard error. *p<0.05 vs. control (analysis of variance). PTX=paclitaxel; PP=Peyer patches; IE=intraepithelial; LP=lamina propria.
GALT phenotype
The PP and LP lymphocytes showed no significant differences in the percentages of αβTCR+, γδTCR+, CD4+, CD8+, or B220+ cells among the three groups (Tables 2–4). However, in the IE spaces, the percentages of CD4+ cells were significantly higher in the control group than in either the low- or the high-PTX group (Table 3). Absolute numbers of γδTCR+ and CD4+ cells in PP were significantly lower in the high-PTX than in the control group. In addition, there were significantly more CD4+ cells in the IE spaces in the control group than in either of the PTX groups (Fig. 4).
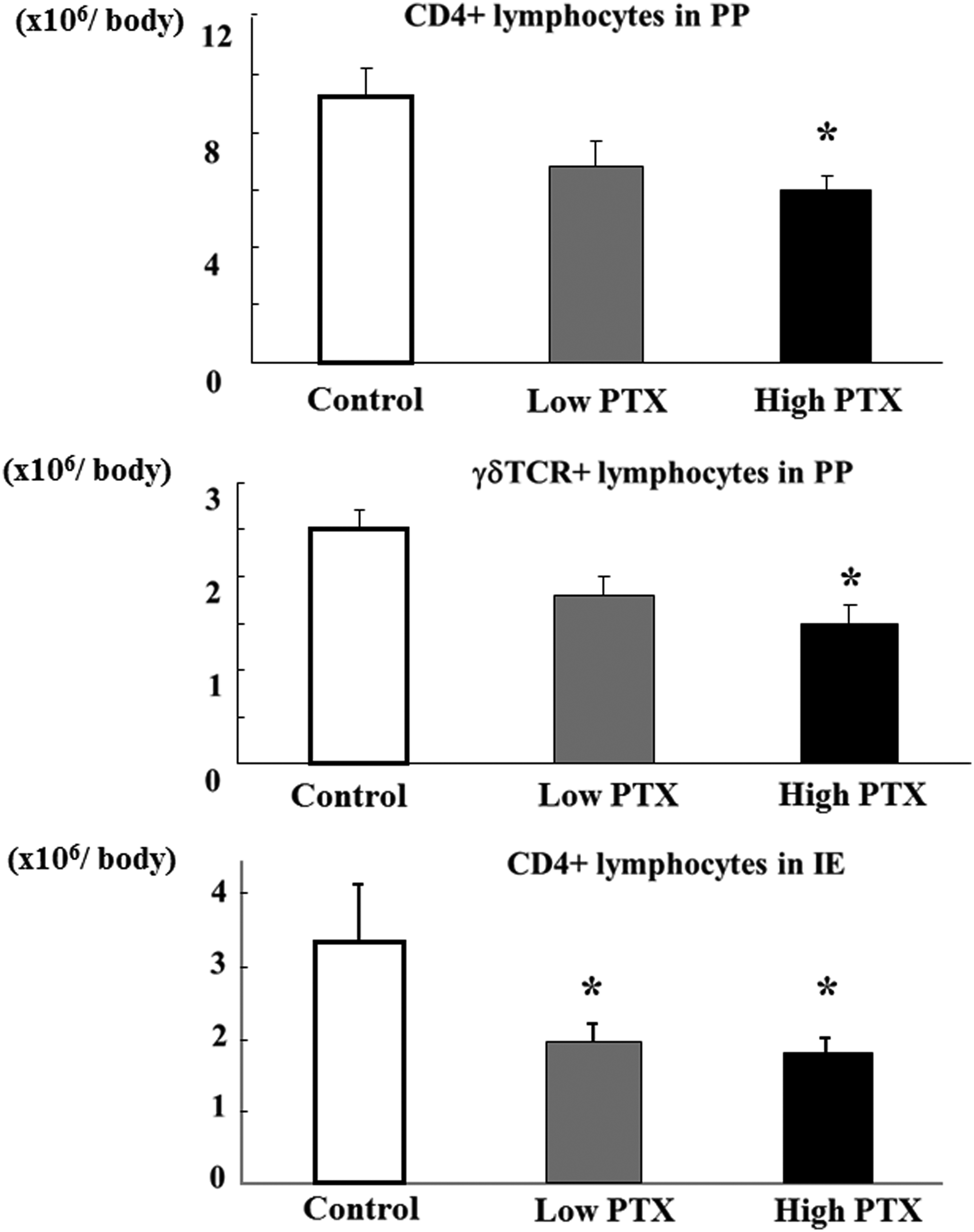
Absolute numbers of CD4+ lymphocytes in Peyer patches (PP) and intraepithelial (IE) spaces or γδ+ lymphocytes in PP. Values are means±standard error. *p<0.05 vs. control (analysis of variance) PTX=paclitaxel.
P<0.05 vs. control (analysis of variance).
Secretory IgA concentration
There were no significant differences in intestinal IgA concentration among the three groups (Fig. 5). Nasal and respiratory tract IgA concentrations were significantly lower in the high-PTX than in the control group when we defined these concentrations as those of nasal plus bronchoalveolar washings. The low-PTX group was midway between the control and high-PTX groups in these measures, but the differences did not reach statistical significance.
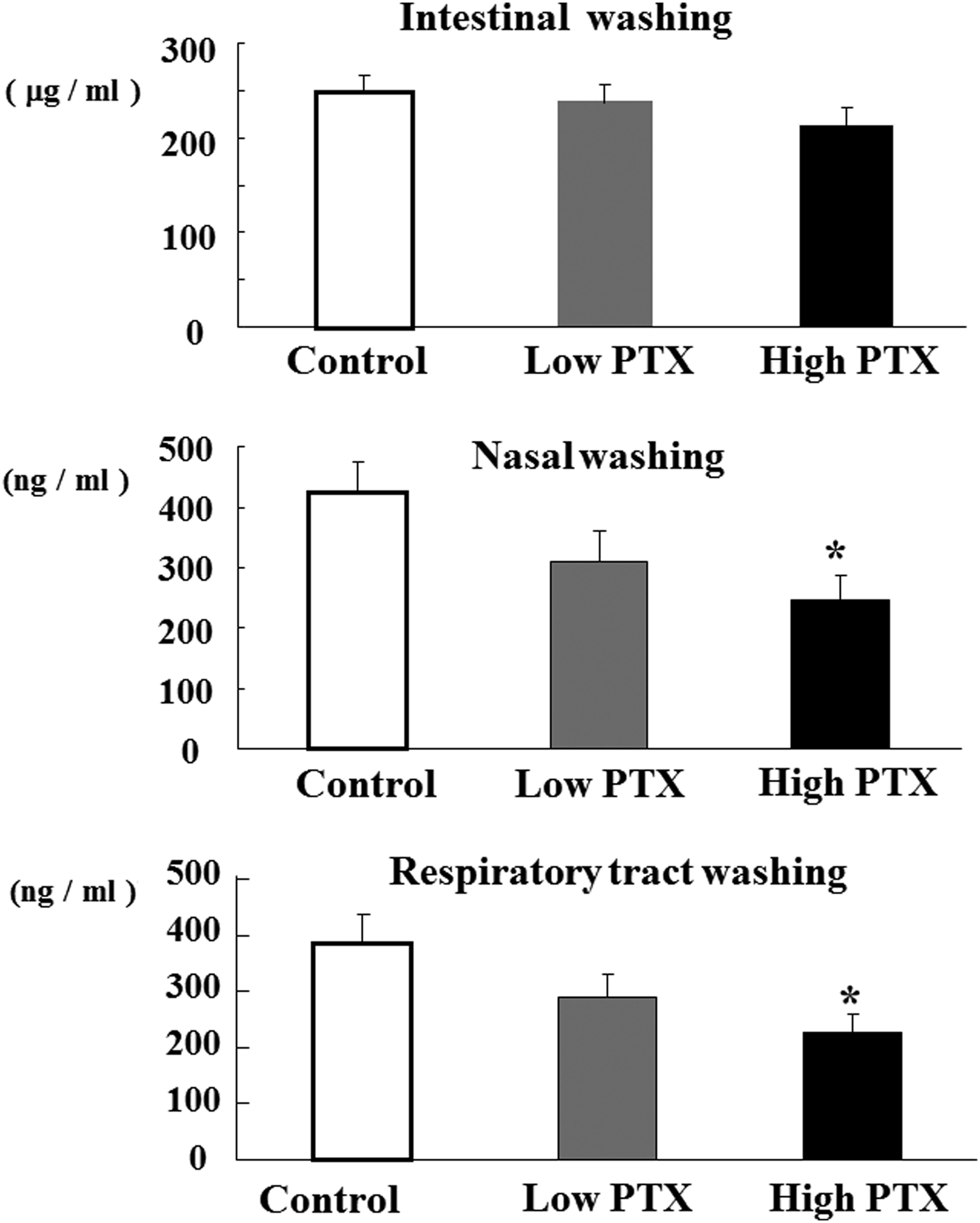
Mean secretory IgA concentration±standard error. Respiratory tract washings=(nasal+bronchoalveolar washings)/2. *P<0.05 vs. control (analysis of variance). PTX=paclitaxel.
Histopathologic changes
Figure 6 shows representative H&E staining of the distal portion of small-intestinal sections from the control, low-PTX, and high-PTX groups. In the high-PTX group, PP size was decreased, whereas the low-PTX group showed only minor changes (Fig. 6A–C). However, the histologic appearances of luminal structures such as villous height or mucosal thickness were similar in the three groups. In the proximal and middle portion of the small intestine, a similar finding was observed (Fig. 6D–F).

Hematoxylin and eosin-stained sections of representative small intestinal tissues from control and low- and high-dose paclitaxel mice. Histopathologic changes are described in the text. Peyer patches from control (
Discussion
The present study demonstrated the influence of PTX on GALT cell mass and function. A high dose of PTX reduced lymphocyte numbers at PP GALT inductive sites, with decreased absolute numbers of γδTCR+ and CD4+ cells, but did not influence total lymphocyte numbers in GALT effector sites. In association with the GALT mass reduction, nasal and respiratory tract IgA concentrations were decreased in the high-PTX group, whereas the IgA concentration in the intestinal washings did not show significant differences among the three groups.
The absolute numbers of CD4+ cells in PP and IE spaces and of γδTCR+ cells in the PP were significantly higher in the control than in the high-PTX group. Reduction in absolute numbers of CD4+ and γδTCR+ cells in the PP as a result of PTX injection may impair systemic mucosal immunity. In fact, a reduction in CD4+ cells in GALT in the absence of enteral nutrition has been documented in association with impaired mucosal immunity [13,17]. In addition, intestinal γδ+ T lymphocytes are mainly involved in innate immunity and help to maintain mucosal homeostasis by participating in oral tolerance to food antigens and intestinal flora, in mucosal tissue repair, and in immunity to viral antigens and tumor cells [18–21]. Moreover, a recent study showed that activated human γδ T cells can serve as antigen-presenting cells and induce both Th- and Tc-cell-mediated responses [22]. New therapeutic methods to increase these lymphocytes during chemotherapy are needed.
Although our present results do not elucidate the mechanisms underlying the decreased PP cell number in the high-PTX group, we can speculate about some possible mechanisms. One possibility involves the effects of PTX on microtubules and cell proliferation. Because PTX inhibits cell proliferation by stabilizing microtubules [11] and PP lymphocytes proliferate more than IE and LP lymphocytes, the influence of PTX on PP may have been greater than that on IE spaces and LP. To the contrary, we previously reported administration of 5-fluorouracil (5-FU), an inhibitor of thymidylate synthese, to reduce lymphocyte numbers in IE spaces and LP without marked changes in PP lymphocyte number [23]. Second, PTX may have lowered adhesion-molecule expression on the high endothelial venules of PP, leading to reduction of PP cell number, because PTX reportedly exerts inhibitory effects on endothelial-cell adhesion and migration [24]. In therapy for coronary artery disease, PTX drug-eluting stents prevent in-stent re-stenosis by inhibiting endothelial-cell adhesion and migration [25]. A previous study indicated that exposure to PTX downregulates the expressions of lymphocyte function-associated antigen (LFA)-1 and intercellular adhesion molecule (ICAM)-1 in mastocytomas [26]. In addition, colchicine, a drug that inhibits cell microtubules, inhibits CD54 expression by human umbilical-vein endothelial cells as well as LFA-1 expression by human T lymphocytes [27]. Therefore, the interaction between naïve lymphocytes and endothelial cells may be altered in response to PTX.
Unexpectedly, the IgA concentration in small intestinal washings did not differ significantly among the three groups regardless of whether or not PP cell numbers were reduced. One possible reason may be the maintenance of LP number despite PTX treatment. The LP is the major gut mucosal effector site enriched with IgA-producing cells. Otherwise, polymeric immunoglobulin receptor (pIGR), produced by epithelial cells, might be preserved in the PTX group, as PTX treatment did not affect the gut epithelial layer in a histologic study [28]. The pIgR is a specialized transport protein for IgA, which affects the luminal IgA concentration. Nevertheless, a decrease in respiratory tract IgA concentration as a result of high-dose PTX may have been associated with reduced PP cell number and suggests impaired extraintestinal mucosal immunity.
Generally, administration of anticancer drugs reduces villous height and mucosal thickness, as reflected by the GI side effects of these drugs [29,30]. Taxanes induce unique histologic changes in the epithelium of the GI tract associated with cell necrosis [11]. However, the dose in this study did not cause gut morphologic changes. Previously, Kadota et al. reported no abnormal histologic findings in the jejunum or the ileum after intravenous administration of PTX to rats [31]. The doses given by Kadota et al. were much higher than those administered in the current study. Mason et al. examined the effect of PTX on the GI mucosa in a murine model, with injections of single doses of 10 and 40 mg/kg of PTX [32]. They demonstrated the appearance of the jejunal mucosa to be nearly normal at 24 h after PTX administration, whereas mitotically arrested cells could be seen in the proliferative zone at 3–4 h. Therefore, our gut morphology data are broadly consistent with the results from these previous studies.
Because chemotherapy is often associated with a variety of disturbances that can affect nutritional status profoundly, chemotherapy-induced malnutrition may reduce the secretory IgA response and GALT lymphocyte number. However, low- and high-PTX mice ate almost the same amount of chow as the control group, and body weight changes did not differ significantly among the three groups in the present study. In addition, blood cell counts showed no significant differences. Thus, we do not consider the GALT alterations observed in this study to be attributable to nutritional factors.
The present data suggest that during chemotherapy with PTX, special tactics aimed at preserving mucosal immunity may be needed. We demonstrated previously that concomitant infusion of fish oil with 5-FU reverses 5-FU-induced GALT atrophy and normalize the respiratory tract IgA concentration [33]. Certain dietary compounds, especially probiotics and fiber, enhance intestinal secretory IgA production in healthy animals [34]. In addition, diets rich in flavonoids, such as cocoa and apple polyphenols, increase the γδ T cell population in GALT [35,36]. Supplements containing these immune-enhancing nutrients need to be tested as a possible strategy for avoiding PTX-induced impairment of mucosal immunity.
Based on pharmacologic information about PTX, the lethal dose (LD50) for mice given intravenous injections is approximately 12 mg/kg. In our preliminary study, we examined the effects of intravenously administering 6, 4, and 2 mg/kg of PTX to mice. The body weights of the animals treated with 6 mg/kg had decreased markedly after seven days, whereas the other two groups showed no weight loss. Thus, 4 mg/kg and 2 mg/kg do not appear to cause malnutrition and were chosen for this study. In addition, these doses are relevant to clinical use, although the difference between mg/m2 and mg/kg is a problem.
The current study has limitations. We performed a pilot study with a five-day time frame. However, neither the 2 mg/kg nor the 4 mg/kg dose of PTX produced deficits in gut immunity. Next, we extended the period to seven days and obtained the present data. We administered only a single dose of the drug, not repeated injection, as would be done in the clinical setting. Moreover, we observed GALT atrophy at only one time point; i.e., seven days after PTX injection. We recognize the importance of conducting a longitudinal study. Our future studies will focus on reducing the impacts of these limitations.
In conclusion, intravenous administration of high doses of PTX reduces PP lymphocyte numbers and the respiratory tract IgA concentration, whereas low-dose PTX has relatively minor effects. Because PTX has been considered to have relatively minor GI side effects, clinicians may not pay attention to gut function during chemotherapy with this drug. However, the present study raises the possibility of paclitaxel-related impairment of gut immunity, leading to a higher risk of respiratory tract infection. Careful dose selection and new therapies may be important for maintaining mucosal immunity during PTX chemotherapy.
Footnotes
Author Disclosure Statement
We received no financial or commercial sponsorship and no support from grants, organizations, or donations of equipment or drugs for this work.