
Abstract
Abstract
Background:
Retroperitoneal infection can be lethal. Optimal management is still elusive to describe because of the small number of case reports. We presented here a case of retroperitoneal abscess caused by Clostridium difficile arising in the puerperal period.
Methods:
Case report and review of recent English-language literature.
Results:
The patient presented with surgical incision dehiscence. A gas-forming fluid collection was discovered in the pelvic retroperitoneal fascia by computed tomography, but the patient did not show marked symptoms of sepsis. Emergency laparotomy drainage and debridement were performed. Clostridium difficile was isolated, and she was treated with a three-week course of vancomycin. The patient recovered without major morbidity. Recent case reports describe variation in the course of the disease and management options for puerperal retroperitoneal infection.
Conclusion:
Puerperal retroperitoneal abscess caused by C. difficile can present with minimal symptoms. Prompt recognition, early surgical intervention, and optimal use of antibiotics can reduce morbidity and prevent death.
I
Case Report
A 25-year old nulliparous Thai woman presented with unexplained fetal demise at 22 wk gestation. Medical termination was performed using vaginal misoprostol and intravenous oxytocin. There was spontaneous rupture of the membranes two days later, and she soon developed chorioamnionitis. Her cervix was unfavorable; therefore, hysterotomy was performed to evacuate the infected conceptus. No intra-operative complication was reported during the surgery. However, total wound dehiscence occurred on the fifth day postoperatively. Gram staining of wound discharge showed mixed bacteria, including oval, sub-terminal spore-bearing Gram-positive bacilli, which was suggestive of a non-perfringens Clostridium (Fig. 1). Rectovaginal examination found a pelvic collection with crepitus. Emergency computed tomography (CT) showed large pockets of gas-containing fluid in the retroperitoneal space. Other, smaller fluid collections were present between bowel loops (Fig. 2). Her vital signs remained stable, except for a low-grade fever.
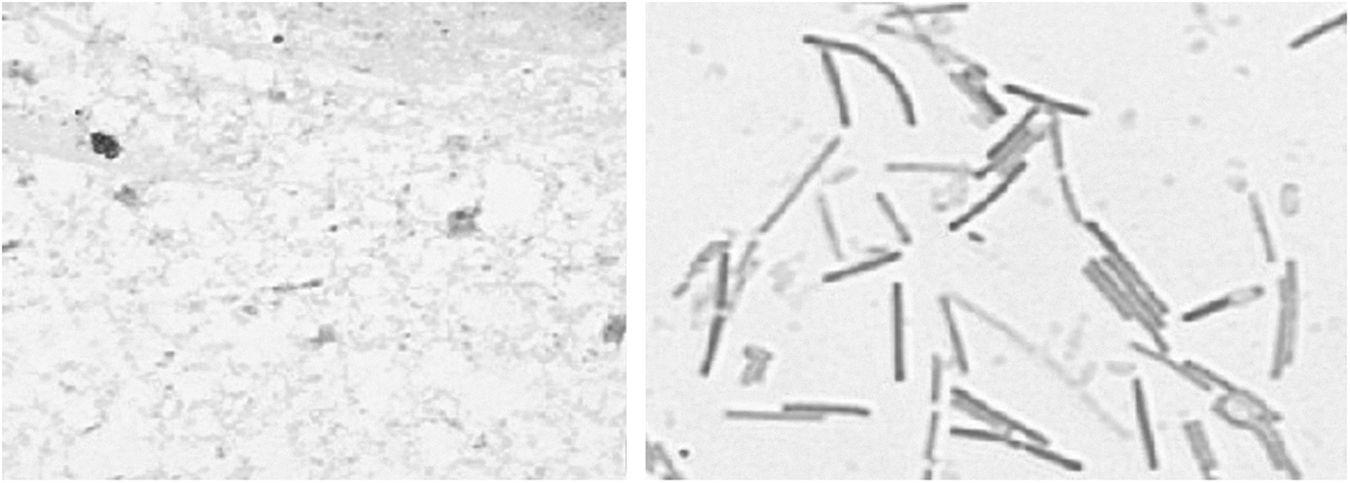
Gram stain of material from surgical site shows large gram-positive bacilli with oval sub-terminal spores. Spore formation was more prominent after culture.
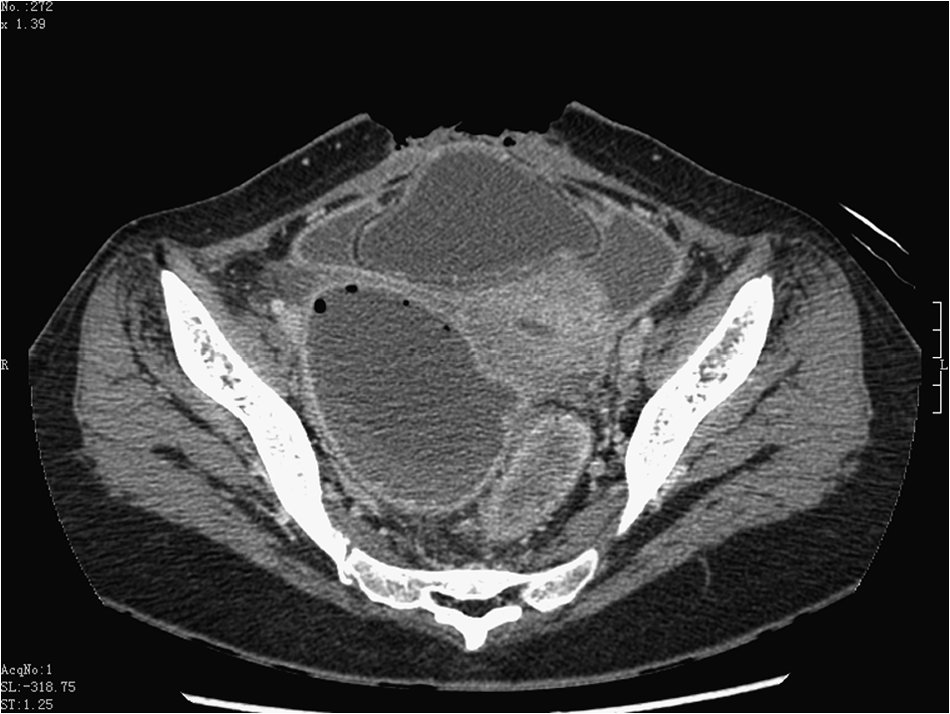
Computed tomography reveals gas-containing collection in endopelvic fascia. Disruption of abdominal incision is noted.
The patient agreed to a prompt re-exploratory laparotomy including the possibility of hysterectomy. Prior to the surgery, both ureters were catheterized cystoscopically. A large amount of pus was drained from the retroperitoneal pelvic collections by blunt and sharp dissections of the necrotic endopelvic fascia until a bleeding tissue plane was reached (Fig. 3). Collections between the bowel loops also were evacuated. Systematic examination of the small and large bowel excluded injury from the previous operation. The decision was made to preserve the uterus because her uterus appeared to be free from infection, and the Gram stain suggested a non-virulent strain of Clostridium spp. Operating time was 3 h, with an estimated blood loss of 500 mL. Percutaneous drains were placed. The skin and subcutaneous tissue were left open for delayed primary closure five days later.
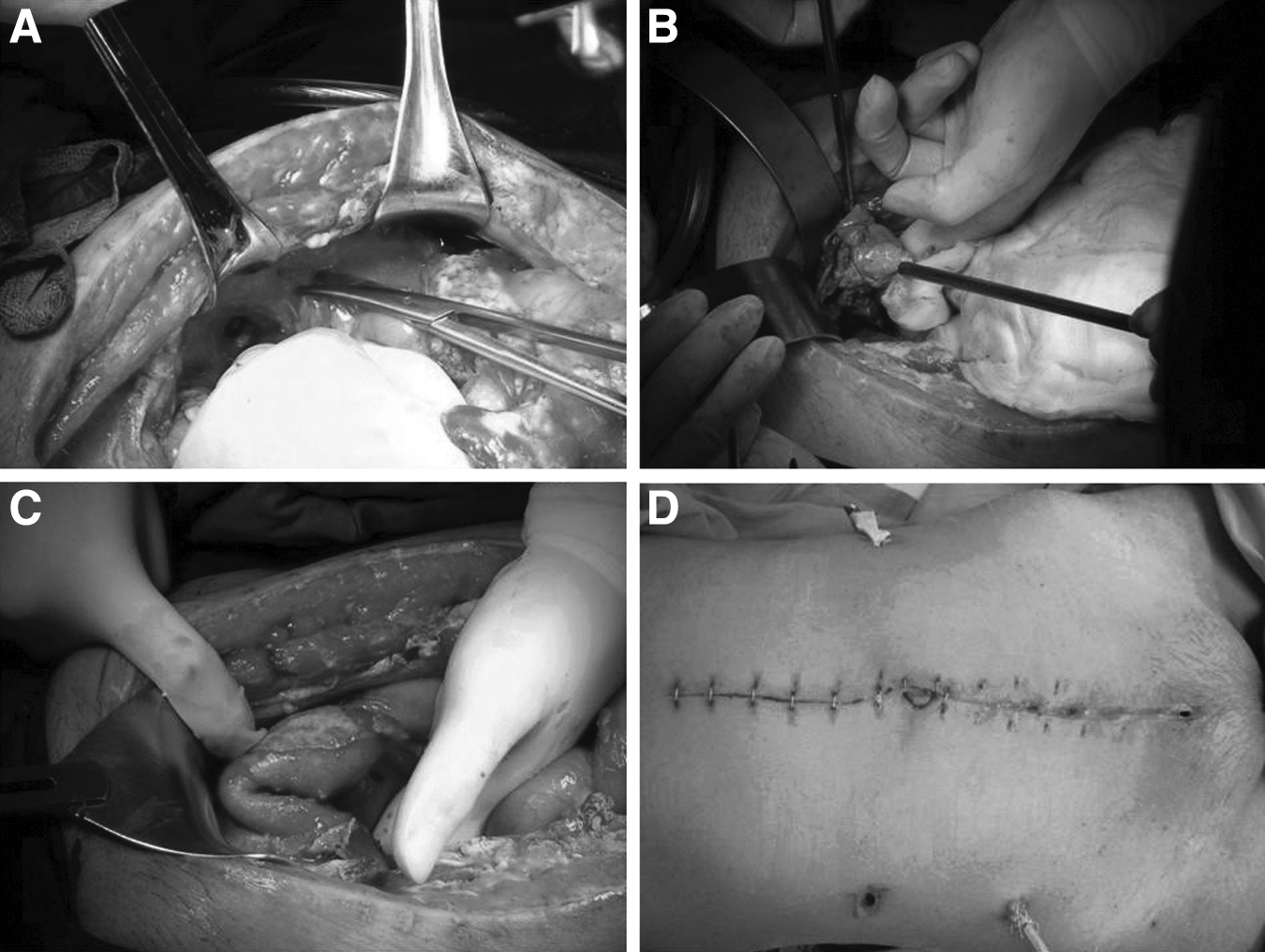
Intra-operative and post-operative findings. (
Vancomycin was given empirically at a dose of 1 g q 12 h IV for five days. Bacterial culture of the retroperitoneal collection revealed mixed aerobic and anaerobic bacteria, including Clostridium spp. The Clostridium was identified subsequently as C. difficile by its phenotype and 16S ribosomal DNA sequencing. Tests for toxin genes (A, B, and binary) were negative. After the patient became afebrile, she was switched to oral vancomycin 500 mg q 6 h for the next two weeks. No other antibiotics were used. The patient recovered without morbidity.
Discussion
Retroperitoneal infection is a serious obstetric complication. The mortality rate can be as high as 20%, especially if the infection is complicated by necrotizing fasciitis [2,3]. Symptoms of sepsis may not correlate with the size of the retroperitoneal collection. Aerobic bacteria are identified most frequently as the major cause [4,5]. However, co-infection with anaerobic bacteria may occur, although its real incidence may be underestimated. If Clostridium spp. is suspected from the Gram stain, identification to the species level essential to guide the treatment.
Definitive risk factors for puerperal retroperitoneal infection are still unclear. We were able to identify 12 recent reports of retroperitoneal infection associated with miscarriage or delivery (Table 1). An association between the route of delivery and retroperitoneal infection is still elusive. According to the data in Table 1, most retroperitoneal infections developed after vaginal delivery (nine of 12), followed by miscarriage (n=2), and cesarean delivery (n=1). The higher proportion of retroperitoneal infection after vaginal delivery may be either because of the higher number of such deliveries or the less aseptic nature of vaginal birth compared with cesarean section. Chorioamnionitis was diagnosed in two of nine patients with necrotizing fasciitis following cesarean delivery [3].
Impaired immunity during pregnancy, concurrent use of non-steroidal anti-inflammatory drugs, diabetes mellitus, malnutrition, older age, and peripheral vascular diseases can contribute to post-partum infection [6]. The psoas muscle is the most common site of ascending infection because of its rich vascular supply and direct lymphatic drainage from the genital tract. Psoas abscess may present as pelvic pain, edema, and sepsis, as shown in seven of the case reports summarized in Table 1 [2]. Sonography is the main imaging modality to diagnose pelvic collections, but CT or magnetic resonance imaging may be helpful in equivocal cases because of their superior soft-tissue contrast and larger field of view [7,8]. In addition to ascending infection from the genital tract, surgical site infection, iatrogenic bowel injury, and hematogenous spread from an extra-abdominal site can lead to retroperitoneal abscess [9,10].
There is substantial diversity in the clinical manifestations of puerperal retroperitoneal infection that may not be associated with the route of infection. For example, an infection after a simple vacuum aspiration led to a serious case of psoas abscess, which required laparotomy for drainage [11], whereas another case of surgical site infection of cesarean section incision led to a minor psoas abscess that was treated successfully with aspiration and a short course of antibiotics [9]. Estimation of the true prevalence of puerperal retroperitoneal infection may be difficult because of under-reporting of cases with adverse outcomes.
Variation in management of puerperal retroperitoneal infection is notable. A long course of antibiotics alone may be adequate for an isolated, small psoas abscess [9, 12–14]. A combination of antibiotics and simple aspiration may be adequate for a collection of moderate size [7, 9]. If the collection is large but still contained in the retroperitoneal space, percutaneous drainage may be established with CT or ultrasound guidance to prevent recurrence [15–19]. Laparoscopy was used to guide the placement of continuous drainage in a pediatric case [20]. Exploratory laparotomy for drainage and extensive debridement can be lifesaving if the infection has spread beyond the retroperitoneal space [11]. Adequate drainage and extensive debridement should be accomplished in a single operation. Re-exploration is associated with increased morbidity [21]. Careful pre-operative preparation such as bilateral ureteral catheterization can facilitate adequate dissection of the pelvic fascia and prevent injury to the ureters. Prompt action is crucial, as delayed management can result in permanent disability such as hip joint damage [17].
It is important to exclude the more virulent species of Clostridium, especially C. perfringens, which causes gas gangrene, or C. sordellii, which causes toxic shock syndrome [22, 23]. Toxins produced by these Clostridium spp. are highly lethal. Because no antitoxins are available, prompt removal of the uterus is necessary. Clinically, profound septic shock is common in infection with virulent strains of Clostridium. Gram stain remains an excellent bedside test to identify the type of Clostridium by its morphology. Clostridium perfringens is a large gram-positive bacillus without spores. A large gram-positive bacillus with oval, sub-terminal spores, was present in our patient, could be either the virulent C. sordellii or the more benign C. difficile. The minor systemic symptoms in our patient were consistent C. difficile. This organism is a normal inhabitant of the genital tract in 18% of women [24]. Genetic typing assay can confirm the species and identify the primary source of infection for the purpose of tracing the origin of the infection [25].
In conclusion, our case illustrates a favorable outcome of puerperal retroperitoneal abscess treated with surgical intervention and antibiotics. This serious obstetric infection may not be preventable, but a timely, definitive approach can reduce the morbidity. Although our patient did not have obvious sepsis, her diagnosis could have been made earlier by checking for signs of infection of the incision in the first few days after her first operation. Individual risk factors, such as her chorioamnionitis, have to be recognized. The value of a strict aseptic protocol during surgery cannot be overemphasized. Prophylactic antibiotics have been proved to reduce serious infectious morbidity after abdominal delivery [26]. Alternative interventions may be available in the future with advancing knowledge of critical care, better antibiotics, or partially hyperbaric oxygen therapy [2, 27].
Footnotes
Acknowledgment
We thank the dedicating nursing staff at the Department of Obstetrics and Gynecology, Faculty of Medicine Siriraj Hospital. We thank the patient for her consent to this report.
Author Disclosure Statement
The authors have no conflicts of interest.