
Abstract
Abstract
Background:
Mycobacterium tuberculosis infection rarely penetrates both skull and dura with temporalis muscle abscess formation.
Methods:
Case report and review of the literature.
Results:
A non-immunocompromised female patient with a right temporal mass underwent surgical resection. The tubercular abscess extended from the temporalis muscle to the skull and through the dura and subdural space with dissemination of the granuloma over the arachnoid membrane.
Conclusion:
Adequate debridement with a full course of antituberculous medication is necessary for complete treatment of these lesions.
Case Report
A 73-year-old female from a persistent right temporal headache for two months. Initially, she did not seek medical treatment. However, there was a tender, progressively growing mass over the area of the headache beginning about one month before admission, and she eventually came to our hospital for help. She had had diabetes mellitus for years with regular insulin use and fair blood sugar control. No other major systemic disease or intravenous drug addiction was noted.
On physical examination, there was an extremely tender soft mass measuring 3×3 cm over the right temporalis muscle. The skin was intact, and no palpable lymphadenopathy was noted. Other physical findings were unremarkable. Laboratory tests showed a white blood cell count of 4,500/mcL without abnormal differential counts. The human immunodeficiency virus test was negative. Preoperative magnetic resonance imaging (MRI) revealed a 4-cm abscess over the right temporalis with skull penetration and signs of leptomeningitis (Fig. 1A). Focal brain edema was apparent on the T2-weighted fluid attenuation inversion recovery sequence (Fig. 1B).
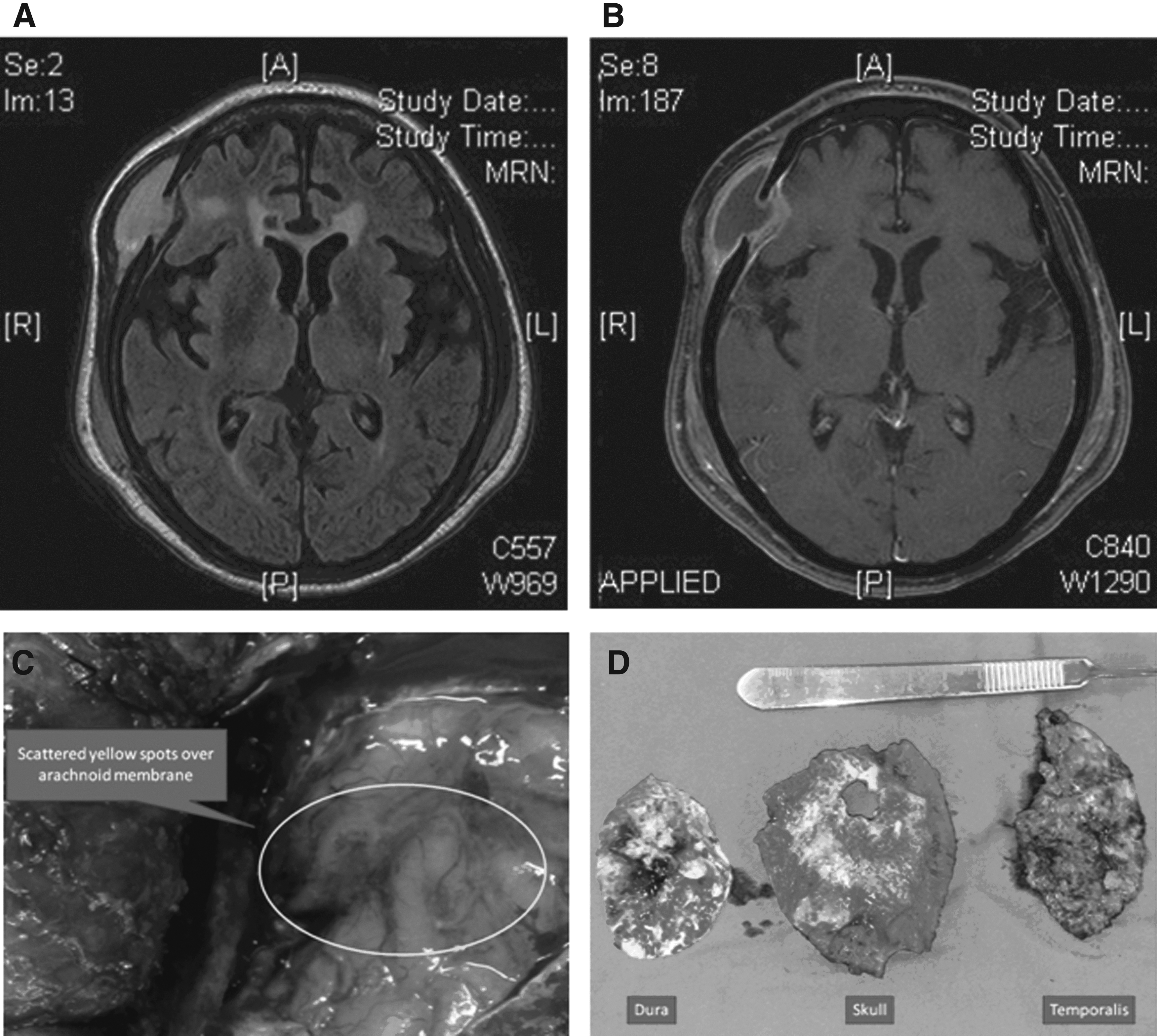
Views of tubercular temporalis abscess. (
The patient complained of intractable pain, and surgical intervention for resection and biopsy therefore was arranged. We resected a cystic lesion measuring 4×5 cm inside the right temporalis muscle with yellowish purulent material within; further, a penetration defect measuring 1×1 cm was noted in the underlying skull. The dura was exposed via craniotomy, and granulomatous changes were seen with a dural defect measuring 1×1 cm that was continuous with the skull defect. After removal of the abnormal dura, multiple white points were visible scattered over the arachnoid membrane (Fig. 1C).
The resected specimen is shown in Figure 1D. Histopathologic examination of the intraoperative frozen section showed chronic inflammation with granulomatous changes, whereas the final pathology report described necrotizing granulomatous inflammation with positive M. tuberculosis culture.
The patient's headache was relieved soon after the operation. No neurologic deficit or seizures were apparent. The patient recovered smoothly and was discharged on post-operative day 7. A course of antituberculous medication was completed through the outpatient department.
Discussion
Temporalis abscess is a rare presentation of M. tuberculosis infection [3]. Concomitant osteomyelitis of the skull and subsequent tuberculous meningitis is even rarer. Most cases of tuberculous infection of the skull or the central nervous system are confined epidurally [2,4] or subdurally because of the strong dural barrier composed of tenacious connective tissues. In our case, the tuberculous abscess extended from the temporalis muscle to the subarachnoid space; this may indicate the destructive ability of necrotizing granulomatous inflammation. Rich and McCordock showed that the meninges could not be infected directly by hematogenous spread [5] and indicated various possible routes of the spread of infection by M. tuberculosis. The route of the infection may be direct contact with a strong local inflammatory process that can cause dural invasion, which is observed most often in malignant rather than infectious disease.
Although rare, extradural and intradural M. tuberculosis infection can occur; the possibility of dural destruction by the infectious processes should be considered during surgical planning. Adequate debridement with a full course of antituberculous medication is necessary for complete treatment.
Author Disclosure Statement
No competing financial interests exist.