
Abstract
Abstract
Background:
Biliary ascariasis is a common problem in Third World countries and other underdeveloped areas of the world. Ascaris lumbricoides migrates into the biliary tree, where it is apparent commonly on diagnostic imaging. We present a unique case of a patient with chronic right upper quadrant abdominal pain, massive hepatolithiasis, and stricture of a previous hepaticojejunostomy in whom ascariasis was found.
Methods:
A 28-year-old female presented to the emergency department with right upper quadrant abdominal pain, syncope, and seizure-like activity. She was found by magnetic resonance cholangiopancreatography to have cholangitis, choledocholithiasis, and bile duct stricture. After multiple radiographic studies, she was taken to the operating room for revision of a hepaticojejunostomy performed 10 years previously.
Results:
Ascaris lumbricoides was found in the right intrahepatic bile duct, that had not been identified by multiple radiologic modalities. The worm was sent to the pathology department for identification. A Fogarty catheter was passed into the hepatic ducts for successful stone extraction. The hepaticojejunostomy was revised, with catheter placement in the Roux limb to accommodate radiologic stone extraction as necessary. Post-operatively, she was given a single dose of albendazole and discharged on hospital day 19.
Conclusion:
The worm was likely the nidus for the stricture and stone formation. Surgical exploration of the biliary tree was required to diagnose and treat her condition accurately. This case is unique in that typical means of diagnosis failed to identify the causative agent of hepatolithiasis because of the prior Roux-en-Y hepaticojejunostomy.
Case Report
A 28-year-old female was transferred to this facility from an outside hospital with right upper quadrant abdominal pain, syncope, and seizure-like activity. She was found to have cholangitis, choledocholithiasis, and a bile duct stricture on magnetic resonance cholangiopancreatography (MRCP). Workup of her syncope revealed a normal ejection fraction, no regional wall motion abnormalities, and a bicuspid aortic valve. She was transferred to this facility for endoscopic retrograde cholangiopancreatography (ERCP).
On admission, the patient reported sharp, chronic right upper quadrant pain with intermittent exacerbations over the last 11 years. Her medical history included a complicated cholecystectomy and pancreatic cyst removal in 2001. Laboratory investigation revealed elevation of liver enzyme concentrations, with aspartate transaminase (AST) 82 U/L, alanine aminotransferase (ALT) 129 U/L, alkaline phosphatase 1,224 U/L, and serum total bilirubin concentration 1.2 mg/dL. She was admitted and started on antibiotics. Attempted ERCP on hospital day (HD) two failed, as cannulation of the bile duct was unsuccessful. She underwent percutaneous transhepatic cholangiopancreatography (PTC) with drain placement on HD three, which depicted clearly a Roux-en-Y hepaticojejunostomy with ductal dilation and hepatolithiasis (Fig. 1A). She improved and was discharged on HD seven with the biliary drain intact and plans for repeat PTC in a few weeks.
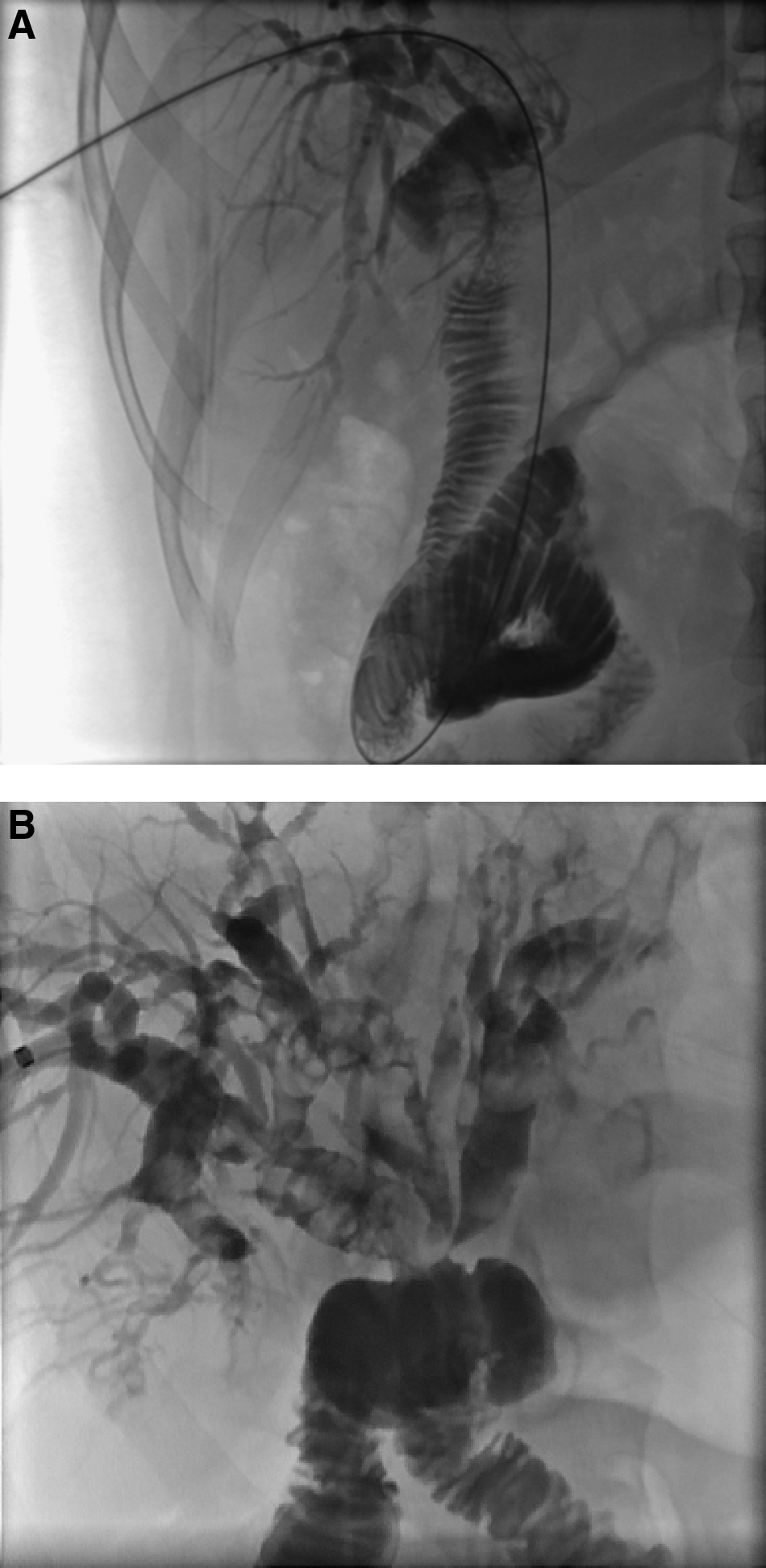
Percutaneous transhepatic cholangiograms in a 28-year-old female. (
The patient returned to the emergency department two weeks later with fever, chills, and right upper quadrant abdominal pain. The abdominal examination was a notable for tenderness in the right upper quadrant, no peritoneal signs and with bile fluid from the PTC drain. Admission laboratory study revealed a white blood cell count of 7.1×109/L; eosinophils at 10×109/L; and elevated liver enzymes lipase (72 U/L), and total bilirubin concentrations (2.1 mg/dL). She was admitted, the fluid was cultured, and she was started on antibiotics.
The interventional radiology department performed a repeat cholangiogram with stent exchange on HD seven, revealing continued dilation of the biliary system and severe stenosis of the hepaticojejunostomy (Fig. 1B). On HD 11, she underwent revision of the hepaticojejunostomy with stone extraction. Intraoperatively, a stricture was found at the hepaticojejunostomy. The PTC catheter was flushed vigorously, producing a large number of stones and an 8-inch worm (Fig. 2). The worm appeared parasitic and was identified later as Ascaris lumbricoides. A No. 4 Fogarty catheter was passed into the left and right posterior hepatic and right anterior hepatic ducts with removal of all accessible stones, which were small, black, and friable. An 8.5F pigtail catheter was placed through the skin and advanced into the Roux limb and bile duct to facilitate future stone extraction by interventional radiology if needed. The Roux limb was reanastomosed to the hepatic duct in a Kasai-like fashion with 5-0 polydioxanone suture.

Hepatolithiasis and Ascaris lumbricoides found in right hepatic duct.
The patient did well postoperatively with no complications. The infectious diseases department was consulted about the parasitic infection, and stool cultures were ordered, yielding no evidence of ova or parasites. A single dose of oral albendazole was given prior to discharge on HD 19.
Discussion
Ascaris lumbricoides is the largest nematode that infects the intestinal tract of human beings, infecting approximately 1.3 billion individuals—25% of the world's population [1,2]. It accounts for 20,000 deaths per year [2]. Adult worms live primarily in the duodenum and proximal jejunum, growing to 35 cm in length and 6 mm in width [3]. The presence of a few worms in the intestine is rarely noticed; however, large numbers of worms can cause abdominal pain and diarrhea [3]. Fever or drug therapy may stimulate migration of these worms to other locations, such as the bile ducts, appendix, or stomach [4,5].
Transmission of the parasite occurs by ingestion of fertilized eggs in contaminated food or by contact with contaminated hands [4]. Larvae hatch in the intestine and migrate through the liver or heart to the lungs, where they are coughed up and swallowed to re-enter the intestine [4]. Infection by A. lumbricoides is diagnosed often by the finding of eggs in feces or passage of an adult worm in feces or emesis [3]. Infections can cause nutritional deficiencies and growth retardation secondary to lactose intolerance and malabsorption of vitamin A [4]. Patients with biliary ascariasis present with recurrent bouts of pyogenic cholangitis, biliary colic, pancreatitis, multiple liver abscesses, biliary cirrhosis, or cholangiocarcinoma [2,6]. Dead worms are associated often with choledocholithiasis, hepatolithiasis, liver abscess, stricture, or cirrhosis, something that is not true of living worms [2]. Studies have demonstrated the possibility of immunodiagnosis of ascariasis in patients with hepatolithiasis [7]. Intrahepatic stones associated with parasites occur predominantly in the left lobe [7] but can affect the right side. In our case, hepatolithiasis was present diffusely (Fig. 1B).
The worms migrate up through the common bile duct (CBD) and excrete polypeptides, creating chemical reactions leading to allergic responses and spasm of the sphincter of Oddi [2]. As worms migrate through the CBD, they transmit fecal bacteria, causing biliary infections and stasis, leading to stone formation and cholangitis [2]. In addition, A. lumbricoides has high glucoronidase activity, deconjugating bilirubin and providing substrate for creation of pigment stones [2]. Females are five times more likely than males to suffer complications from Ascaris [2]. A suggested reason is relaxation of the sphincter of Oddi caused by progesterone, allowing easy access to the CBD and migration into the liver [2]. Although ascariasis is more common in females, it causes more severe symptoms in males [2].
The worm may be visible on ultrasound scans or cholangiography as a tube-like structure [8]. Endoscopic modalities have been used to treat hepatolithiasis and choledocholithiasis [6], but in our case, this was not possible because of the prior hepaticojejunostomy. Hepatobiliary ascariasis is difficult to detect with imaging or at surgery because most worms move out of the ducts within 24 h of entry [7]. If worms are trapped and die in the bile ducts, they can cause multiple problems, including hepatolithiasis [7].
Treatment of A. lumbricoides infection is primarily non-operative, including antihelminthic agents such as albendazole or mebendazole, analgesics, and antibiotics. However, worms in the biliary tree are not killed easily because the drugs are excreted poorly in bile [5]. In these cases, surgical management may be necessary for elimination of these parasites, specifically in patients with pyogenic cholangitis, worms retained for longer than four weeks, worms coexisting with stones, and associated liver abscess [2]. The creation of a hepaticocutaneous jejunostomy after surgery provides atraumatic access to the biliary tree for removal of recurrent stones [7]. In our case, a drain was placed in the Roux limb of the hepaticojejunostomy to facilitate subsequent stone extraction.
Reinfection with A. lumbricoides has been described in patients who have undergone endoscopic sphincterotomy. Some studies cite a prevalence of infection with A. lumbricoides of 47%–97.7% of the original prevalence [8,9].
Conclusion
Although A. lumbricoides can migrate into the biliary tree, where it commonly is found by diagnostic imaging, our case is unique in that the typical means of diagnosis failed to identify the cause of hepatolithiasis because of the prior Roux-en-Y hepaticojejunostomy. In this case, surgical exploration and irrigation of the biliary tree was required to diagnose and treat her condition accurately.
Footnotes
Author Disclosure Statement
No competing financial interests exist.