
Abstract
Abstract
Background and Purpose:
Whereas the negative impact of infectious complications (IC) during the index hospitalization after elective surgery is well established, the long-term ramifications of hospital-acquired post-operative infections are not well studied. This analysis evaluated the impact of a hospital-acquired IC after open abdominal vascular surgery on the readmission rate and the mortality rates 30 and 90 days after initial discharge.
Methods:
Data from all hospitals in the United States that performed elective open abdominal vascular operations in the Medicare population from 2005 to 2007 were extracted from the national Medicare Provider Analysis and Review database. The cohort consisted of all patients undergoing open abdominal vascular operations, including aortic, iliac, and visceral procedures. The ICs evaluated were pneumonia, urinary tract infection (UTI), postoperative sepsis (sepsis), surgical site infection (SSI), and Clostridium difficile infection (CDI). Patients were categorized as either developing an IC during their initial hospitalization (Index+INF) or not developing an IC (No INF). The rates of 30-day readmission, 30-day IC, and 30- and 90-day mortality after the initial discharge were evaluated longitudinally and compared in patients with and without an IC.
Results:
A total of 29,549 open abdominal vascular procedures were identified, and 4,016 patients (13.6%) developed an IC during their index hospitalization: Pneumonia (5.1% of the total), UTI (2.7%), sepsis (1.6%), SSI (1.4%), and CDI (0.6%). Additionally, 1.13% of patients developed pneumonia, UTI, SSI, or CDI complicated by sepsis. The hospital mortality rate during the initial hospitalization was 13.7% (Index+INF) versus 4.0% (No INF) (p<0.0002). Infectious processes (pneumonia, UTI, SSI, and CDI) complicated by sepsis had an in-hospital mortality rate significantly higher than patients having an IC alone (50.9% vs. 13.7%; p<0.002). The mortality rate 30 and 90 days after the initial discharge was significantly higher for Index+INF than for No INF (4.4% vs. 1.2% and 8.6% vs. 2.6%, respectively; p<0.0002). The highest 30-day mortality rates after discharge were found after CDI+sepsis (30%), pneumonia+sepsis (12.6%), and postoperative sepsis alone (8.6%). The same rank was found for the 90-day mortality rate: 30%, 22.5%, and 13.8%. Overall, readmission was more likely for Index+INF than for No INF (33.7% vs. 21.5%; p<0.0002). Rates of 30-day readmission after an index IC ranged from 32% to 50%.
Conclusion:
For Medicare beneficiaries undergoing elective open abdominal vascular procedures, the development of any IC significantly increased not only the in-hospital mortality rate but also the mortality rates 30 and 90 days after discharge from the hospital. Index ICs also were associated with a higher 30-day readmission rate. Hospital-acquired infections have a profound late effect on outcomes after discharge. Future programs targeting high-risk patients may improve long-term survival and minimize readmissions.
This study was designed to identify the occurrence of ICs after open abdominal vascular procedures [6], and to assess the impact of these complications on the readmission and long-term mortality rates. This analysis evaluated the initial and secondary ICs and their impact on longitudinal rates of 30-day re-admission, 30-day IC, and 30- and 90-day mortality after initial discharge. As well, secondary infections that developed after initial discharge and were associated with readmission were evaluated.
Patients and Methods
This study was approved by the Institutional Review Board of the University of Medicine and Dentistry of New Jersey–Robert Wood Johnson Medical School.
Data source
The data were derived from the Medicare Provider Analysis and Review (MedPAR) database from 2005 to 2007, which contains information regarding hospitalizations of Medicare beneficiaries. This database, with its personal identifiers, allows the tracking of hospitalizations and provides dates of death as late as three years after the dates of discharge. From among the numerous available variables, we selected demographic characteristics (age, gender, and race), type of admission, dates of admission and discharge, principal and secondary diagnoses and procedures, and date of death when appropriate. To recognize comorbid diseases, we used the Agency for Healthcare Research and Quality (AHRQ) Healthcare Cost and Utilization Project (HCUP) Comorbidity Software, version 3.5 (AHRQ, Rockville, MD) [7]. This software creates 29 co-morbidity measures, of which we used the following: Hypertension, congestive heart failure (CHF), valvular heart disease, chronic pulmonary disease, diabetes mellitus with and without chronic complications, renal failure, and obesity.
Study population
We included all Medicare beneficiaries age 65 years or older who were hospitalized and underwent elective open aortic, iliac, or visceral vascular procedures during the first two days (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] procedure codes 38.34, 38.44, 38.64, 39.24, 39.25, and 39.26). To identify post-operative infections, we used the following ICD-9-CM codes for the secondary diagnoses: 480.x, 481, 482.0–482.2, 482.3x, 482.4x, 482.8x, 482.9, 483.x, 485, 486, 997.31, and 997.39 for pneumonia; 599.0 and 996.64 for UTI; 038.0, 038.1x, 038.2, 038.3, 038.4x, 038.8, 038.9, 785.52, 995.91, and 995.92 for sepsis; 998.5x. 998.31, 998.32, and 998.83 for SSI and nonhealing surgical incision; and 008.45 for CDI.
Statistical analysis
Data analysis and all statistical calculations were performed with SAS version 9.2 (SAS Institute, Cary, NC). Hospital mortality and IC rates were calculated as the numbers of patients who died or developed ICs during the hospitalization for the index procedure, respectively, divided by the number of hospitalized patients undergoing the index procedure, the result being expressed as a percentage. The 30- and 90-day mortality rates were computed as the number of persons who died during the first 30 or 90 days after discharge following the index procedure, divided by the number of persons discharged alive after the index procedure, also expressed as a percentage. Thirty-day readmission or IC rates were calculated by dividing the number of patients who were re-admitted to the hospital or who developed IC(s) during the 30 days after initial discharge by the number of patients who were discharged alive after the initial hospitalization; both of these rates were expressed as percentages. Differences in rates between the groups were determined by chi-square analysis and calculating the odds ratio (OR) with the 95% confidence interval (CI). To minimize confounders, multivariable logistic regression analysis with stepwise selection was used, and adjusted outcomes (IC, readmission, death) were calculated by the patient's demographic characteristics (age, gender, and race) and comorbidities. The Cochran-Armitage test was utilized for trend analysis. P<0.05 was considered statistically significant.
Results
We identified 29,549 Medicare beneficiaries ages 65 years and older who underwent open elective abdominal vascular surgical procedures in 2005–2007. The relevant characteristics of these patients are presented in Table 1.
Among these patients, 4,016 (13.6%) developed post-operative (initial) infection during the index hospitalization. As shown in Table 1, postoperative ICs increased significantly with age, from 12.2% in the youngest group to 16.0% in the oldest patients (p<0.0001 for trend). Women were more likely to develop infection than were men (OR=1.21; CI=1.13–1.30). We did not find significant racial differences in the rates of post-operative infection in this study cohort, although such differences have been found in other studies, as reviewed recently [8].
Figure 1 demonstrates the frequency distribution of various postoperative ICs during the index hospitalization. Among these infections, pneumonia was the leading diagnosis followed by UTI, sepsis, SSI, and CDI. In some cases, pneumonia, UTI, SSI, and CDI were complicated by sepsis. The highest proportion of sepsis was found in conjunction with SSI (18.0%), followed in decreasing order by pneumonia (11.2%; p<0.0002), CDI (7.0%), and UTI (4.5%).
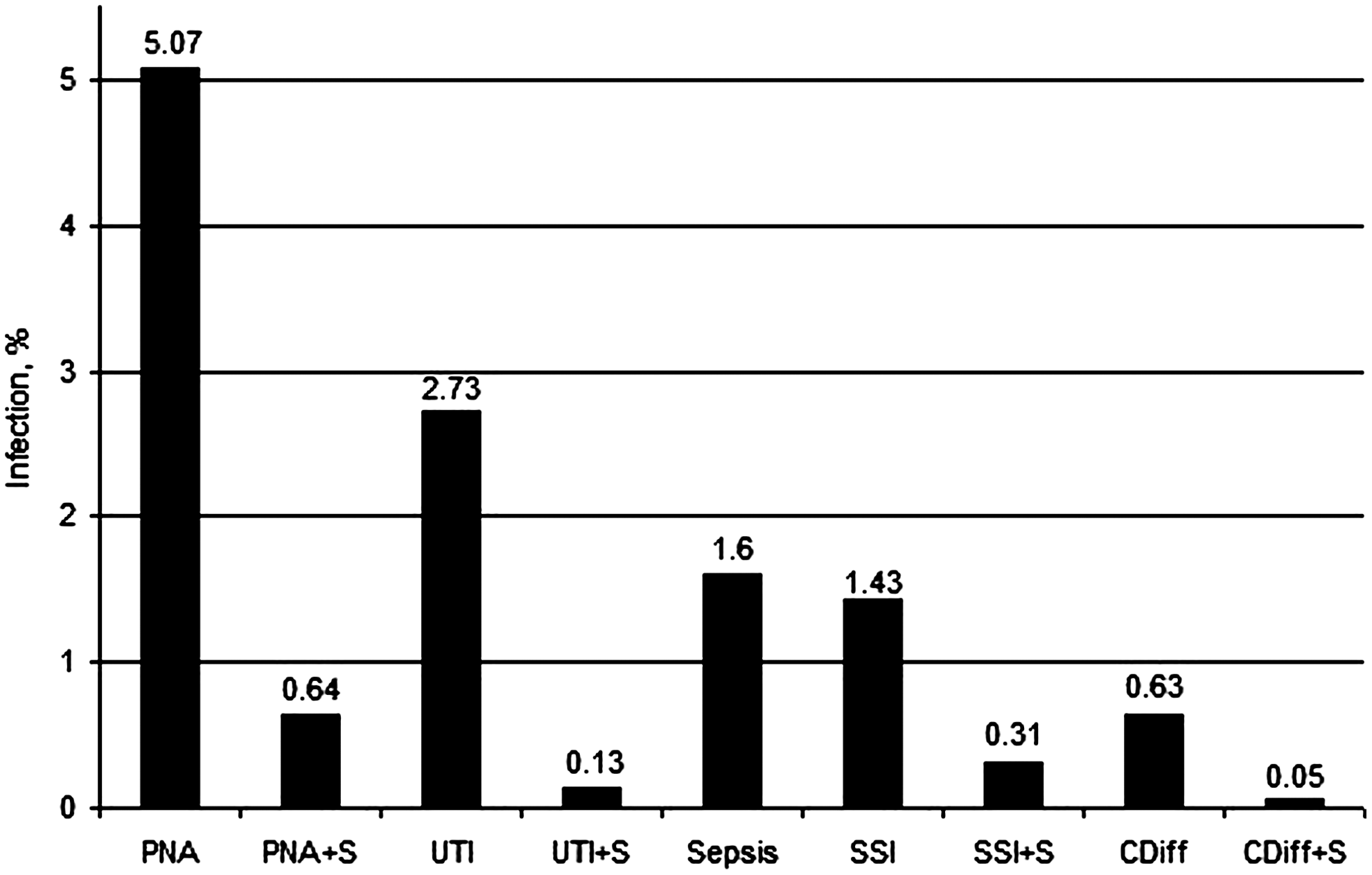
Rates of various postoperative infectious complications during index hospitalization. See text for definitions. +S=infection coexisted with sepsis.
The development of postoperative ICs worsened the outcome significantly. Overall, patients with infections were 3.8 times more likely to die during the index hospitalization than were those without infection (CI 3.39–4.22). Figure 2 displays the rates of in-hospital mortality after various ICs. Sepsis was the most often fatal IC, more than doubling the risk of death. Other infectious processes (pneumonia, UTI, SSA, and CDI) complicated by sepsis increased the mortality rate dramatically, from 5.5% to 39.1% overall (p<0.0001).
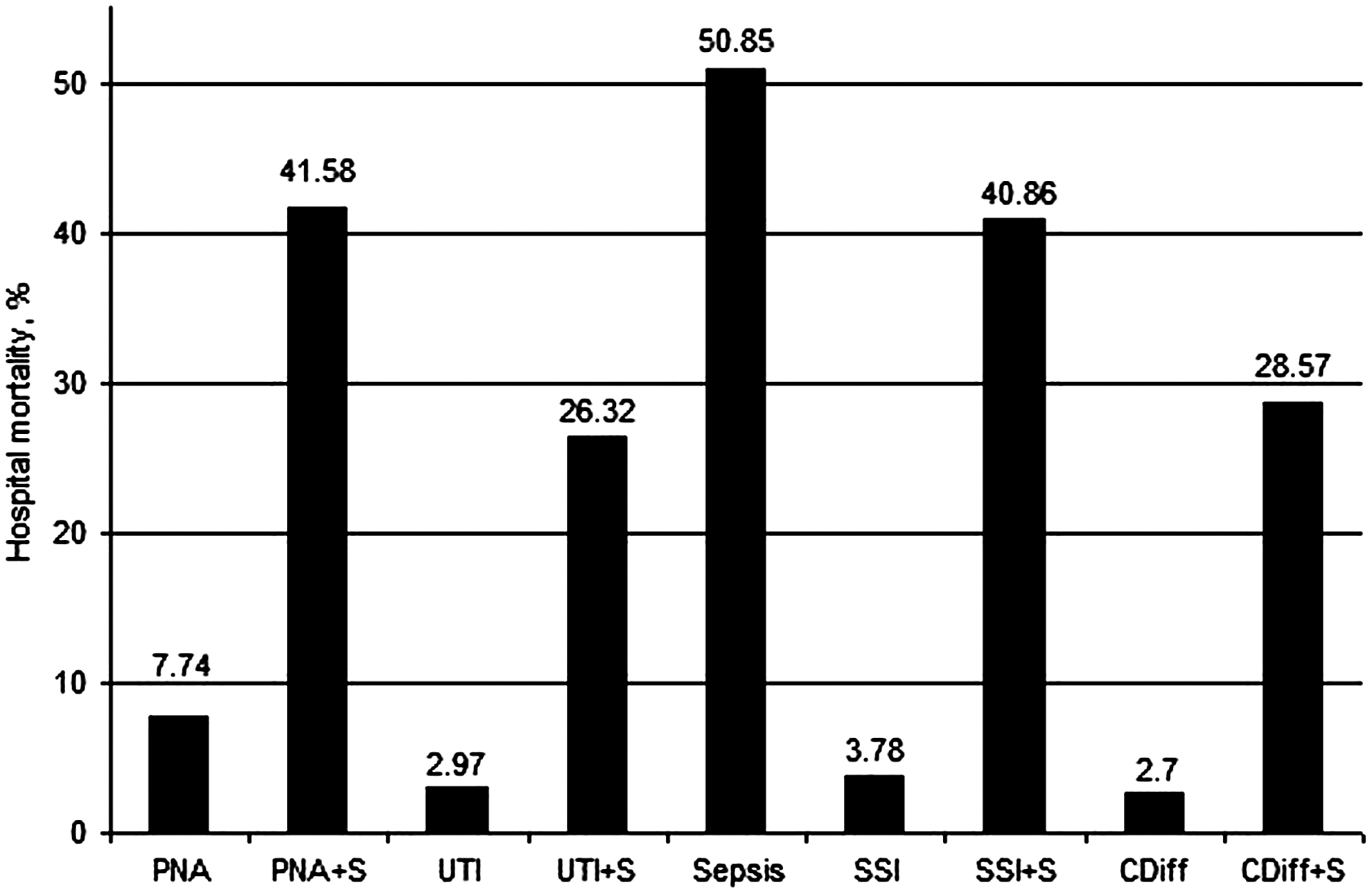
Hospital mortality rate after infectious complications during index hospitalization. See text for definitions. +S=infection coexisted with sepsis.
Infection after surgery affected both the short- and long-term mortality rate, and also increased hospital re-admissions. Patients who developed ICs during the index admission were 1.9 times (CI 1.72–2.01) more likely than patients without infection to be readmitted to the hospital within 30 days after the index discharge. The results were similar after adjustment by patient age, race, gender, and co-morbidities (OR 1.7; CI 1.55–1.82). This analysis also demonstrated that women were more likely than men to be re-admitted (OR 1.3; CI 1.25–1.41), and black patients were more likely to be re-admitted than were white patients (OR 1.3; 95% CI 1.16–1.51). No differences were identified in the 30-day readmission rate among patients with various types of post-operative infections.
Mortality rates in patients with and without initial IC were compared at 30 and 90 days after the index discharge. In the univariable analysis, patients with initial infection were more likely to die during either time interval than were non-infected patients (OR 3.8; 95% CI 3.15–4.69 and OR 3.6; CI 3.10–4.11, respectively). In the multivariable logistic regression analysis, the likelihood of dying after the index discharge was greater for patients with initial infection versus those without infection within both 30 (OR 2.9; CI 2.37–3.59) and 90 (OR 2.7; 95% CI 2.33–3.14) days.
Among the 24,503 patients who did not develop post-operative infection during their index hospitalization, were discharged alive without infection, and were evaluated 30 days after the index discharge, 1,503 (6.13%) developed secondary infection. As demonstrated in Figure 3, SSI was the predominant secondary infection, followed by UTI, pneumonia, sepsis, and CDI. After adjustment, women were more likely to develop secondary infection during the 30 days after discharge than were men (OR 1.5; CI 1.33–1.65). The same was true of black and Hispanic patients compared with white patients (OR 1.3; CI 1.03–1.67 and OR 2.0; CI 1.20–3.28, respectively). Other risk factors for secondary infection were advanced age, CHF (OR 1.6; CI 1.42–1.90), chronic pulmonary disease (OR 1.2; CI 1.08–1.34), diabetes mellitus (OR 1.2; CI 1.07–1.44), and renal failure (OR 1.9; CI 1.66–2.25).
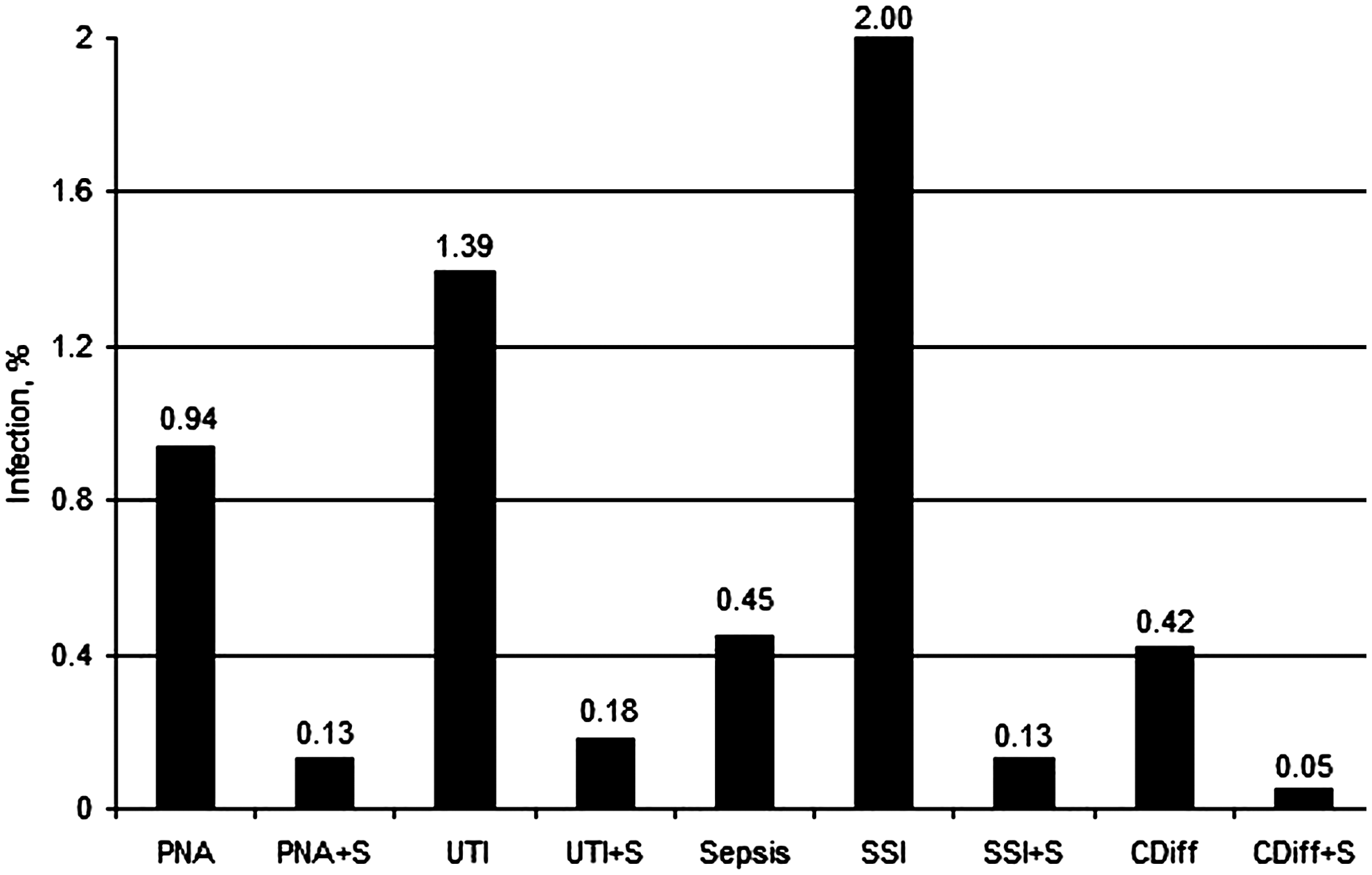
Rates of secondary infections during 30 days after index discharge in patients without initial infections. See text for definitions. +S=infection coexisted with sepsis.
Secondary infection that developed in patients without initial infection increased the mortality rate significantly during the 30 and 90 days after discharge (from 0.87% to 6.05%, p<0.0001; and from 1.90% to 12.01%, p<0.0001, respectively). This finding was confirmed by multivariable logistic regression analysis with adjustment for age, gender, race, and co-morbidities. Compared with patients without secondary infection, those who developed infection were more likely to die during the 30 (OR 6.1; CI 4.73–7.95) and 90 (OR 6.6; CI 5.46–7.87) days after the index discharge. Risk factors for death in both periods of time were advanced age, CHF, and renal failure, whereas chronic pulmonary disease was a risk factor for death within 90 days.
Discussion
This analysis utilized population-level Medicare data to evaluate not only the impact of ICs on the index admission but also the ramifications of an IC for long-term mortality and readmission rates.
The Medicare Payment Advisory Committee (MedPAC) identified pneumonia, heart failure, and acute myocardial infarction (AMI) as common, costly causes of hospitalization, with a high proportion of potentially preventable re-admissions. It has been recommended by MedPAC that Congress and the Centers for Medicare and Medicaid Services implement policies to address these high rates [9]. With the possibility of differential reimbursement for performance, there is pressure to identify risk factors to assist in minimizing these complications. Hospital readmission rates represent an important proxy measure for poor-quality inpatient and outpatient care and poor care transitions [10,11]. Linking hospital readmission rates to reimbursement is a complex issue that may have unintended negative consequences. Healthcare policy makers and the healthcare industry should give careful attention to developing innovative care transition measures and refining readmissions analyses for hospital reimbursement [9].
This analysis has demonstrated the impact of ICs, not only on the initial hospital stay but also on readmission and late mortality rates. Infection after elective surgery affected not only the short-term but also the long-term mortality and hospital readmission rates overall. Patients with an index hospitalization infection were 1.9 times more likely to be re-admitted within 30 days after the index discharge. The hospital mortality rate at the index admission was highest for those patients suffering sepsis as a postoperative complication. The highest 30-day mortality risk after discharge was found with infections that manifested as sepsis. Clostridium difficile infection with sepsis had the highest mortality rate, followed by pneumonia complicated by sepsis; these finding were similar at the 90-day analysis. The overall 30-day mortality rate after discharge for patients without infection was 1.2%, which increased to 4.4% when an IC developed during the index admission. Furthermore, the 90-day mortality rate increased from 2.6% to 8.6%. Infection during the index hospitalization increased the 30-day readmission rate from 22% to 34%.
Many would argue that patients who develop ICs are more likely to need readmission on other grounds. Authors have suggested a risk-standardized measure of hospital re-admission rates to account for this bias; this has been found to be predictive of readmission [12]. Of note, the present cohort was risk adjusted by age, race, and gender, yet patients with ICs still were almost twice as likely to be readmitted. Further supporting this finding was that in the present cohort, black patients were more likely to be readmitted than white patients. Realizing that this is an epidemiologic study with a complete data set of the Medicare population undergoing open abdominal vascular procedures for the years evaluated, one may ask: Why?
Authors have attempted to address the question: Are ICs avoidable? This question was studied by van Walraven et al. in a meta-analysis that examined all readmissions deemed avoidable. The authors concluded that the median proportion of readmissions considered avoidable was 27.1%, but ranged from 5% to 79%. The investigators concluded that the true proportion of potentially avoidable hospital readmissions remains unclear [10].
Beyond the question of avoidable readmissions, examination of the groups with the highest rates of readmission may help to minimize readmissions and late deaths. This study has demonstrated that female and black patients were more likely to be readmitted. It has been suggested that economically disadvantaged patients have poorer overall health status, fewer community resources, and poorer access to primary care, all of which potentially confound assessment of the readmission risk [9]. Joynt et al. evaluated 30-day re-admission rates for Medicare beneficiaries by race and site of care. They utilized national Medicare data to examine 30-day readmissions after hospitalization for AMI, CHF, and pneumonia. They found that overall, black patients had higher re-admission rates than white patients and that patients from minority-serving hospitals had higher readmission rates than those from non-minority-serving hospitals. The authors concluded that black patients were more likely to be readmitted after hospitalization for the three common conditions, a gap that was related to both race and the site where care was received [13].
Theories to explain this epidemiologic finding regarding race are varied and include greater allostatic load [14–17], the stress of the complication, and perhaps increased inflammation or inflammatory mediators leading to greater susceptibility to infection [18]. Nonetheless, there is a distinct and significant association among the development of an IC, re-admission, and the subsequent outcomes of patients over time.
Another important finding from this analysis is the description of ICs that develop after discharge. SSIs were the most common IC after discharge in patients with no in-hospital infection. The association of SSI has been well established in the initial hospitalization [6,19,20], yet few have looked at the ICs responsible for readmission.
The limitations of this study include the potential selection bias derived from limited coding schemes, as well as confounding by indication for the procedures performed. The Medicare data represent administrative discharge data used for billing purposes, and clinical information is limited by the ICD-9 and CPT codes. It is possible that the definitions of indications and coding differ within the data set and among institutions and hospital coders. As well, certain complications may not be captured appropriately in administrative data. Although refined clinical data cannot be retrieved from administrative data, this study describes the rates of ICs after abdominal open vascular surgery, and assesses readmissions of many thousands of Medicare patients in the community at large.
In conclusion, this study has demonstrated that for Medicare beneficiaries undergoing elective open abdominal vascular procedures, the development of any IC significantly increases not only the in-hospital mortality rate but also the mortality rates 30 and 90 days after discharge from the hospital. Index admission ICs also were associated with more re-admissions within 30 days after discharge. Hospital-acquired infections have a profound late effect on outcomes after discharge. Future programs targeting high-risk patients may improve long-term survival and minimize readmissions.