
Abstract
Abstract
Background:
Two percent chlorhexidine gluconate (CHG) is used in preparing the skin of surgical patients. In practice, it often is diluted with saline prior to use. Whether this affects efficacy is unknown, as the manufacturer does not address dilution but does recommend scrubbing twice. We attempted to determine whether diluting CHG affects its antiseptic potency and if one scrub is as effective as two.
Patients and Methods:
To test effects of CHG dilution, 60 healthy subjects were recruited and randomized into a dilution group (20%, 40%, 60%, 80%, or 100% CHG) or a control group (saline). One area of one foot of each subject was prepared, and colony-forming units (CFU) were counted at baseline and at 10 min after preparation. In a second study, 60 subjects were again recruited. Based on the previous study, a 50% dilution was applied as the scrub. Colony-forming units were calculated at baseline and after each CHG application.
Results:
Baseline CFU did not differ among the dilution groups (p=0.49). Subjects in all dilution groups exhibited nearly a 100% decrease in CFU, whereas the control group exhibited an 80% decrease. These results were statistically significant (p<0.01). In the second study, the CFU values after two scrubs (mean 0.1; range 0–3) were significantly lower than after one scrub (mean 3.6, range 0–100) (p=0.02).
Conclusions:
Diluting CHG to a concentration as low as 0.4% does not affect antiseptic efficacy. The manufacturer-recommended two scrubs is superior to one scrub at reducing skin bacterial colony counts.
S
Commonly used skin preparation agents are povidone–iodine (Betadine, Purdue Products, L.P., Stamford, CT.), chlorhexidine gluconate (CHG; Hibiclens (Molnlycke Health Care, Norcross, GA), BactoShield (STERIS Corp, Mentor, OH), iodophor/alcohol-based (Duraprep), and CHG/isopropyl alcohol (ChloraPrep, CareFusion Corp., San Diego, CA). Numerous studies delineate the variance in antiseptic qualities among these agents [3,4]. Although randomized controlled studies are lacking, it is accepted generally that CHG and the alcohol-based agents cover a broader antimicrobial spectrum than povidone–iodine and that CHG has the longest residual antiseptic activity. Most studies describe the anticipated effect of such agents on the hands of operating room staff using the glove juice method. Few studies have investigated how well these products eradicate skin bacteria at surgical sites, such as the abdomen and groin [5,6]. The manufacturer's instructions for the use of BactoShield (CHG 2% solution) do not recommend dilution, and according to their representatives, the company has not investigated the effect of dilution on the product's efficacy. Nonetheless, operating room personnel frequently dilute the product with ill-defined, non-standardized amounts of normal saline in order to make it easier to lather. There are no published studies that examine the implications of this practice. We determined if dilution of CHG increases skin bacterial colony-forming units (CFUs) (Study A) and whether application of two scrubs decreases bacterial CFUs compared with one scrub (Study B). We hypothesized that different concentrations of CHG would differ in bactericidal activity.
Patients and Methods
Patients
One hundred twenty patients were enrolled at one hospital (BMC). Sixty patients were enrolled from January to February 2008 for the dilution study (Study A), and the remaining 60 patients were enrolled from June to July 2008 for the number of scrubs study (Study B). Both studies were Institutional Review Board (IRB)-approved, and IRB standards for informed consent and data confidentiality were maintained. Subjects in both studies were healthy adult (>18 years old) volunteers recruited from the hospital via fliers and e-mail advertisements. Volunteers were compensated $15.00 for participation in the study. Participants were asked to refrain from using systemic/local antibiotics and antibacterial soaps on the area of interest for 1 wk prior to data collection. We recorded demographic data and documented the time since the subjects had last showered.
To standardize data collection techniques, one clinical research nurse performed all surgical preparation and swab collections. The nurse prepared subjects' skin while wearing sterile gloves and according to the BactoShield label instructions (scrub for 2 min, dry with a sterile towel, scrub another 2 min, and dry again) after hand-washing. Bacterial samples were obtained in the following manner. A 6×6-cm2 area was marked on the most level part of each foot sole. A culturette swab tip was placed in culture medium for 10 sec for moistening, after which the tip was wiped over the marked area in a standardized fashion. Samples were then transported to the microbiology laboratory, where laboratory personnel plated the samples and, after a period of growth, counted visually the bacterial colony-forming units (CFUs) on the plates. Samples were incubated in a controlled, New York State Department of Health-approved hospital-based microbiology laboratory, and CFUs were obtained 48 h after sample collection.
Using a random number generator for the dilution study (Study A), the initial 60 subjects were allocated to either the control group or one of the five dilution test groups. This method ensured that there were 10 subjects in each group. One foot was chosen randomly as the test foot. Prior to skin preparation, baseline bacterial counts were taken from all subjects using the aforementioned protocol. The control group was prepared with normal saline. The five test groups were prepared with the assigned percentage of CHG diluted with normal saline: 0, 20, 40, 60, or 80. In the test groups, the chosen foot was prepared as specified by the manufacturer's instructions using the assigned percentage dilution of CHG. Bacterial CFUs were measured 10 min after completion of the preparation. This lag time between skin preparation and measurement of bacterial CFU was chosen to simulate the amount of time from preparation to skin incision in a typical operating room environment.
For Study B, the final 60 subjects were allocated randomly to either a one-time scrub or two scrubs. The method for bacterial testing was identical to that in the first portion of the study save an additional bacterial swab was obtained between the first and second scrubs.
Analysis
In Study A, non-parametric testing was conducted to evaluate the difference in median values for baseline and post-preparation CFU, and p values were calculated using the Kruskal-Wallis test. Baseline CFUs for some subjects were too numerous to count and thus were reported by the laboratory as >500. All analysis was performed with SAS software, V. 9.1 (SAS Institute Inc., Cary, NC).
In Study B, we examined the percent difference in bacterial CFU based on one vs. two scrubs. The p values were calculated using the Wilcoxon signed rank test.
Results
Baseline demographics are displayed in Tables 1 and 2. One-quarter (22%) of the patients in Study A were men, and the majority were aged 41–60 years.
The median baseline bacterial CFU in the cohort of Study A ranged from 100 to 500 without a statistically significant difference among the groups (p=0.49 [Table 3]). The majority of patients had baseline CFUs of 500. The median post-preparation CFU was 0 for all test dilutions (range 0–1) except the control group, which had a median of 26 CFU (range 1–100)(p<0.01). Again, the majority of patients had post-preparation CFUs of 0. Median bacterial CFUs decreased by 100% from baseline to post-preparation for all groups (range 97%–100%) except the control group, which exhibited an 80% median reduction (range 0–100%)(p<0.01). Percent reduction was calculated by dividing the change by the original count.
In Study B, the majority of subjects (more than 50%) had greater than 100 CFUs of bacteria at baseline (Fig. 1). After one scrub, nine of 60 subjects had measurable CFUs (range 1–100). After two scrubs, five of 60 subjects had measurable bacterial CFUs (range 1–5)(p=0.0195). No subjects experienced an adverse reaction to the CHG preparation in either study.
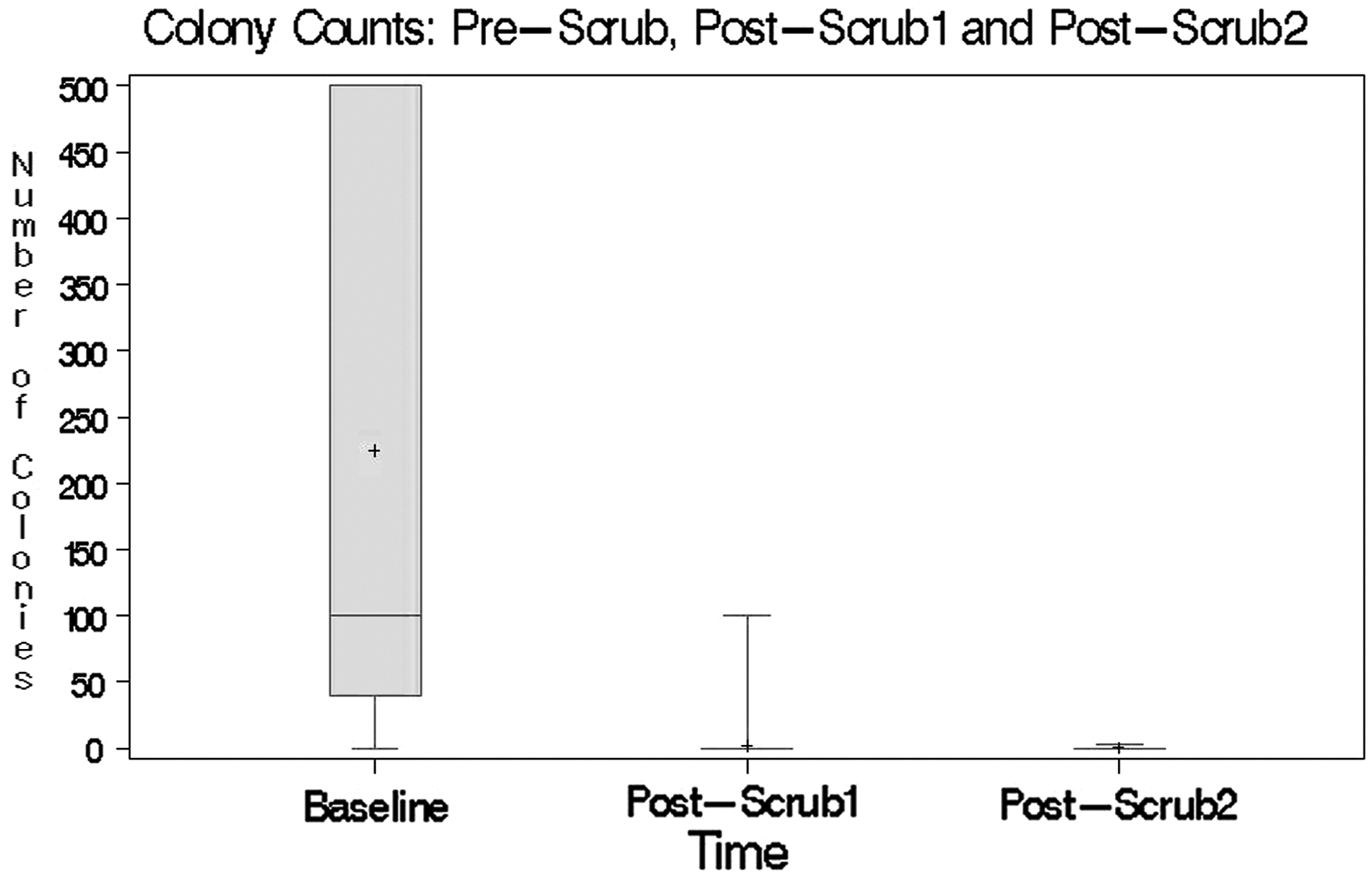
Colony-forming units before scrub and after one or two scrubs (Study B).
Discussion
In Study A, although the sample size was small, groups were similar in age, time since last shower, and baseline bacterial counts, so the results should be reliable. There was a difference in gender in Study A because of an imbalance in the number of volunteers, but the difference was not statistically significant. Thus, differences in CFU reductions should be attributable only to the variance in the CHG dilution. The majority of subjects had high initial counts (>500), but nearly all subjects prepared with any strength of CHG solution, ranging from 20%–100% (i.e., full-strength), had a 100% reduction in the number. This result provides convincing evidence that 2% CHG appears to be as effective in eradicating skin bacteria over a wide range of concentrations, to as low as 0.4% (i.e., 80% dilution with saline).
All subjects in Study A had a reduction in CFUs, including the control group, in which a normal saline preparation alone decreased the bacterial load considerably. This is noteworthy, as the mechanical action of scrubbing accounts for a substantial amount of bacterial removal during skin preparation, whereas CHG appears to enhance this effect.
In Study B, we used both the manufacturer's recommendations and the findings from Study A. We determined that a dilution of 50% would be the reproducible most easily in the operating room. The research nurse obtained samples at three time points to determine the reduction in bacterial counts. In a majority of the 60 subjects, there were no bacteria after one scrub; a second scrub would ensure that all bacteria had been eradicated.
Several limitations of these studies exist, including the small sample size, the somewhat arbitrary sample collection, and the inability to quantify high baseline counts precisely. However, these limitations do not undermine the strength of the results. More pertinent is the question of whether these results are applicable to a variety of clinical settings. Feet were chosen for this pilot study because they could be tested non-invasively and harbored ample bacteria for the anticipated treatment difference to be seen. The authors tested other more clinically relevant sites initially, such as the hand and forearm, but the baseline bacterial burden of these sites was negligible. This study measured treatment effects of CHG at 10 min after preparation to mimic a typical length of time from skin preparation to incision in the operating room. At longer intervals, post-incision and throughout procedures, it is unknown whether diluting CHG affects its touted ability to maintain antisepsis. Finally, subjects were prepared exactly according to the manufacturer's protocol using a two-scrub method. However, in clinical practice, patients often are scrubbed only once. On the basis of our results from Study B, manufacturer guidelines for two scrubs should be employed to ensure complete eradication of surface bacteria.
The practical result of this study addresses the utility of CHG as a preparation agent. Our study suggests controlled dilution of the surgical preparation material would allow a small amount of CHG to be used more efficiently. Dilution for surgical care in areas with limited access or funds may allow a vital resource (skin antisepsis) to achieve wider utilization.
Conclusion
When used as prescribed, 2% CHG appears to be a potent antiseptic agent even when it is diluted to 0.4% of its concentration as manufactured. Two surgical preparations (as recommended by the manufacturer) appear to be better than one. Directions for future research include studying various surgical sites and documenting bacterial CFUs at longer intervals after preparation.
Footnotes
Acknowledgments
We are grateful to Dr. David Borgstrom (research advisor), Ellen Dauchy, RN (clinical research nurse), Patrick Burdick/Melissa Scribani (statistical analysis), E. Donnall Thomas (committee funding), and Timothy Williammee (laboratory supervisor), and Dr. Nicholas Hellenthal (reviewer) for their assistance with these studies.
Author Disclosure Statement
No competing financial interests exist.