
Abstract
Abstract
Background:
Multi-drug-resistant organisms (MDRO) complicate care increasingly on the general ward and in the emergency department, operating room, and intensive care unit (ICU). Whereas barrier precautions are important in limiting transmission of MDRO between patients, few tactics have been defined that reduce the genesis of MDRO.
Method:
Review of pertinent English-language literature.
Results:
Antibiotic heterogeneity practices, as part of an overall antimicrobial drug stewardship program, offer one readily deployable means to reduce selection pressure for MDRO development in the ICU. The data underpinning this approach and data derived from its use indicate that, especially in surgical ICUs, heterogeneity of antibiotic prescribing can preserve or restore microbial ecology, reduce the prevalence of MDRO and the incidence of infections caused thereby, and facilitate the implementation and effectiveness of other antibiotic-sparing tactics, such as de-escalation.
Conclusion:
Heterogeneity of antibiotic prescribing is effective in preventing the dissemination of MDRO pathogens.
Most currently articulated tactics to minimize and militate against resistance rely on newly implemented or enhanced infection control practices, including universal barrier precautions, cohorting, or isolation [7] until patients are proved culture-negative for an MDRO of interest and minimization, and avoidance of high-risk invasive procedures (e.g., percutaneous central venous catheterization [8–11]). Less frequently, modifications of equipment are offered as mechanisms enhancing local control. Such interventions include silver coating on a variety of catheters, as well as antibiotic coating of multi-lumen central venous catheters [12]. New antimicrobial agents are being identified less frequently as salvage options because of the small number of new agents in the pipeline for clinical deployment—tigecycline, telavancin, and ceftaroline are notable recent exceptions [12,13]. Because the rate of development of new antimicrobial agents that may target MDRO is low, the clinician is left with little hope for rescue on that front. Instead, an examination of novel methods of guiding antimicrobial prescription may offer a foundationally sound method to manage extant and emerging MDRO. This review summarizes the evidence underpinning the need for novel antimicrobial prescription practices, the practices that have been identified as potentially useful, and the clinical data derived from deploying those tactics in the critical care unit. The seemingly ubiquitous nature of MDRO in the healthcare environment, the gastrointestinal (GI) tract as a reservoir of MDRO, and the end result of a variety of antimicrobial prescription tactics, specific pathogens, and potentially useful new methods targeting MDRO control in the ICU are discussed.
Emergence of Multi-Drug-Resistant Organisms
Although many microbial isolates in hospitalized patients demonstrate susceptibility profiles amenable to readily available antimicrobial agents, a well-defined group has emerged that demonstrates multi-drug, multi-class, and multi-mechanism resistance [2]. These pathogens may be grouped conveniently under the acronym “ESCAPE.” Initially termed the ESKAPE pathogens [14] (Table 1), the resistance profiles of Escherichia coli and Proteus spp. (as well as other fermentative gram-negative bacilli) have driven the change in terminology from Enterobacter spp. to the more inclusive Enterobacteriaceae family. Similarly, Clostridium difficile, which emerged as a major pathogen after 2001 [15–18], warrants a separate designation. Thus, ESKAPE has appropriately been renamed ESCAPE [19]. This group represents collectively the majority of MDRO infections in hospitalized patients, and their study has articulated paradigms of pathogenesis, transmission, and resistance.
Gastrointestinal Tract as a Reservoir
The density of microorganisms in the normal human GI tract increases progressively as one samples more aborally. Ultimately, the density in the colon averages 1011 to 1012 bacteria/g stool, representing an estimated 15,000–36,000 unique species. Amazingly, this complex ecosystem works in concert with a “community structure” that aids in the processing of nutrients in the luminal contents [5,20,21]. Unsurprisingly, shock and reperfusion, which disrupt normal mucosal barrier integrity, promote translocation and allow lymphatic and hematogenous embolization of bacteria and their products, which may lead to systemic inflammation and, ultimately, organ dysfunction [3,22].
Combination Therapy
Often touted as a means of enhancing antibiotic regimen efficacy and reducing resistance pressure by increasing pathogen eradication, combination therapy (most commonly a beta-lactam-based agent plus an aminoglycoside) has been scrutinized recently in light of antibiotic stewardship program development and deployment. Justification for combination therapy stems from the belief that the extended spectrum of coverage is essential to bridge gaps in empiric monotherapy.
Recent meta-analyses have challenged the veracity of these assumptions. In patients with sepsis, the presumed ideal target patient population for whom benefit might accrue, the addition of an aminoglycoside to a beta-lactam-based regimen fails to improve clinical efficacy and in some circumstances has led to adverse outcomes. More specifically, utilizing a narrow-spectrum beta-lactam agent plus an aminoglycoside, instead of a single broad-spectrum β-lactam agent, is associated with more treatment failures and may have a deleterious effect on the mortality rate. Combination therapy also has produced more frequent adverse events, especially nephrotoxicity. Moreover, short-term combination therapy is ineffective in preventing the development of resistance, as reflected in superinfection or colonization rates after completion of a therapeutic antibiotic course. Analyzing the data specifically to address the question of combination therapy for gram-negative infections yields similarly disappointing but illuminating results. Mortality assessments for patients with gram-negative sepsis identify no outcome advantage for beta-lactam-plus-aminoglycoside regimens compared with beta-lactam monotherapy. In fact, when the beta-lactam antibiotics evidenced similar spectra of activity, the addition of an aminoglycoside was associated with poorer outcomes. Connecting these observations, combination therapy should be chosen on a case-by-case basis, integrating the patient's clinical status with local antibiogram data [23–27].
In sum, there is no evidence that combination therapy of surgical infections provides results superior to those of broad-spectrum monotherapy, even for Pseudomonas aeruginosa infections, the target pathogen for combination therapy. Importantly, combination therapy also fails to prevent the emergence of resistance in gram-negative pathogens. Although in patients with cystic fibrosis, some data support a microbiologic benefit for combination therapy, there is no correlation with better patient outcomes [28].
Collateral Damage by Gram-Negative Pathogens
Combination therapy is not the sole example of an unintended consequence of therapy. Growth of an MDRO organism driven selectively by therapy targeting a different pathogen is termed “collateral damage.”
Antibiotic use has exerted collateral damage on gram-negative pathogens. For example, use of third-generation cephalosporins (GC-3) is linked to the appearance of MDR Klebsiella, MDR Enterobacter, cefotaximase (CTX-M)- and Klebsiella pneumoniae carbapenemase (KPC)-producing beta-lactamase-positive organisms, as well as the development of MDR Acinetobacter. Fluoroquinolones, prescribed with increasingly frequency together with an anti-pseudomonal beta-lactamase inhibitor combination agent as a non-aminoglycoside-based combination regimen, are linked to the genesis of MDR Klebsiella, CTX-M beta-lactamase-producing bacteria, MDR Pseudomonas, and MDR Acinetobacter Finally, carbapenem use is related to the development of KPC beta-lactamases, New Delhi metallo-beta-lactamase 1 (NDM-1), other metallo-beta-lactamases, MDR Pseudomonas, and MDR Acinetobacter. Clearly, antibiotic stewardship programs have multiple opportunities to reduce resistance selection pressure and improve global hospital microbial ecology [29–46].
The strength of such associations is highlighted by evaluating the risk of extended-spectrum beta-lactamase (ESBL)-producing and carbapenem-resistant Klebsiella pneumoniae (CRKP). With increasing duration of exposure to both fluoroquinolones and carbapenems, an adverse interaction of these two agents on the risk of ESBL CRKP development has been identified. Such organisms have followed even 1–4 days of fluoroquinolone administration, with progressively greater risk at 5–10 days and a yet-greater risk at >10 days of exposure [47]. Some of these isolates are pan-resistant and require novel antibiotic administration tactics for their eradication [48].
Antibiotic Resistance Is a Universal Healthcare Problem
Despite the well-characterized prevalence of community-acquired MRSA (c-MRSA), hospital-onset (HO), healthcare-associated community-onset, and c-MRSA have decreased steadily in frequency according to the Active Bacterial Core surveillance reports spanning 2005–2008 [49–52]. In tandem, the rate and number of VRE infections doubled from 2000 to 2006 according to data derived from the National Inpatient Sample (assuming that relatively few vancomycin-resistant infections actually were vancomycin-intermediate or -resistant S. aureus infections) [53]. As vancomycin-resistant pathogens were increasing, epidemic C. difficile was noted in 2000 in association with fluoroquinolone use. Concomitantly, in 1996–2003, there was a significant increase in hospital discharges in which C. difficile infection was the primary diagnosis [54,55].
In 2005, the U.S. Centers for Disease Control and Prevention (CDC) merged three infection-reporting networks into a single entity, the National Healthcare Surveillance Network (NHSN). The NHSN incorporates the National Nosocomial Infections Surveillance program, the Dialysis Surveillance Network, and the National Surveillance System for Healthcare Workers, and allows analysis of infections outside the ICU. Not surprisingly, in light of the changes in the epidemiology of HO and gram-positive pathogens, in surgical site infection (SSI) surveillance of ESKAPE pathogens exclusive of Enterobacter spp., VRE and MRSA predominated from January 2006 through October 2007 [56]. Similar changes were noted in the prevalence of resistant gram-negative pathogens. Drawing again from the NHSN database, three (not four)-class antibiotic-resistant isolates predominated among resistant A. baumannii, P. aeruginosa, and K. pneumoniae [57]. However, four-class resistant isolates were noted in 52% of states for Pseudomonas, 68% of states for Acinetobacter, and 31% of states for Klebsiella, documenting that multi-drug-class resistance is a widespread phenomenon in the United States, as has been noted worldwide [58,59]. It therefore is appropriate to engage in a focused examination of specific pathogens.
Gram-positive pathogens
Emergence, growth, and maintenance of resistant pathogens, including MRSA, VRE, and C. difficile, have been associated with antibiotic prescription practices addressing infections with other organisms, as well as peri-procedural prophylactic antibiotics [42–45,60–66]. The growth of such MDRO may be tracked using nasal swabs during the course of typical hospitalizations. Progression from a GC-1 through a GC-3 to a glycopeptide in response to an MRSA-positive nasal swab has been documented. Unfortunately, as MRSA is treated in patients with prolonged hospitalization, VRE and Candida emerge, another example of collateral damage during therapy [67].
Gram-negative pathogens
In a similar fashion, exposure to antibiotics can drive the evolution of resistance in gram-negative pathogens [68] by exposing them to increasingly powerful antimicrobial agents targeting the specific pathogen that survives the prior agent (Fig. 1). Such progression has been well-documented with the step-wise development of beta-lactamases (i.e., TEM from E. coli, SHV from Klebsiella spp.), ESBL, and, finally, the carbapenemases (KPC from K. pneumoniae) and metallo-beta-lactamases (MBL from Enterobacteriaceae; VIM-1/VIM-4 cluster) with which we struggle now [2,69,70]. Recently, as noted above, a new MBL, NDM-1, was identified in New Delhi, India, highlighting the global nature of the problem with antimicrobial agent resistance. To take another example, CTX-M beta-lactamases were reported initially in Japan in 1986. This family of resistance enzymes is now distributed globally and involved in urinary tract infections to such an extent that infection with such bacteria has been termed a pandemic [71].
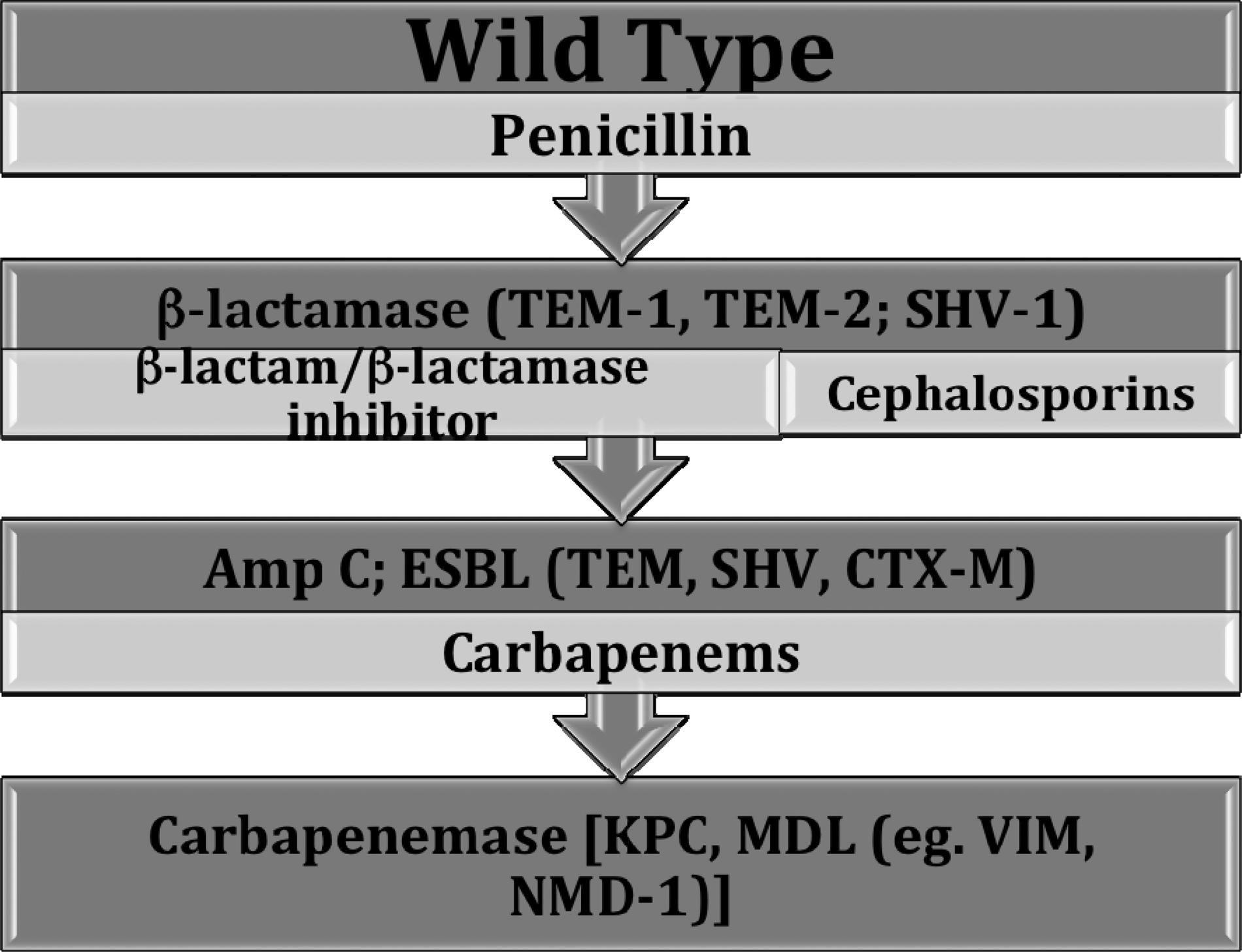
Schematic of evolution of resistance to beta-lactam agents. Adapted from Burgess DS, Rapp RP. Bugs versus drugs: Addressing the pharmacist's challenge. Am J Health-Syst Pharm 2008;65(Suppl 2):S4–S15.
However, β-lactamases are not the sole concern in gram-negative infections. Carbapenemases complicate hospital care increasingly, with outbreaks occurring in a clonal or polyclonal fashion. Carbapenemases are encoded by plasmids that are transmitted readily both within and between species [72–74]. Two significant issues complicate carbapenem resistance further [75,76]. First, because Enterobacteriaceae are normal commensal GI flora, patients with unrecognized CRKP may serve as reservoirs for transmission. Second, low-level resistance may be undetectable by routine laboratory screening techniques. Thus, healthcare providers may be hampered in identifying patients who truly require therapy. Patients with a GI reservoir of MDRO may be suitable for GI decontamination [77–79], but the precise benefit of that therapy for the non-critically ill patient remains unclear.
The KPC-producing Enterobacteriaceae have been identified in 33 U.S. states as well as several other countries, including Israel, Greece, Brazil, China, India, Norway, Scotland, Sweden, and Colombia. Pulsed-field gel electrophoresis (PFGE) and multi-locus sequence testing (MLST) of the blaKPC gene, coupled with polymerase chain reaction mapping of the TN4401 flanking regions and plasmid analysis, fingerprinted the loci responsible for KPC production and determined the clonality of the identified organisms. Sequence homology was noted by PFGE in 80% of isolates, and all had an identical MLST type. These techniques have demonstrated that the specific K. pneumoniae identified in the southwest United States is a single-locus variant of what has been documented in the remainder of the database. The importance of this finding lies in the potential for this specific clone to represent a new and sustainable resistance mechanism [80].
New resistance profiles are disseminated readily across national and continental boundaries by patient or healthcare worker migration or travel. Such is the well-documented case for NDM-1 (discussed above). After the infection was identified in New Delhi, India, in K. pneumoniae from a pressure ulcer, the harboring individual returned to Sweden bearing the MDRO. Within a few months, the NDM-1 gene had been detected in several countries, including the United States [70,81]. Therefore, the healthcare worker's index of suspicion for MDRO must be high regardless of overall hospital epidemiology data. Gram-negative non-enteric bacilli are affected similarly by resistance selection pressures.
Gram-negative non-enteric bacilli
Perhaps the best known of the gram-negative non-enteric group is P. aeruginosa because of its prevalence in hospital-acquired pulmonary and urinary tract infections. Most strains are both invasive and toxigenic, but rarely infect the GI tract, bone, or skin [82,83]. In at least one study, major risk factors for MDR Pseudomonas infection included mechanical ventilation for >48 h and receipt of an anti-pseudomonal carbapenem (as much as 15 d prior to MDR infection onset); fluoroquinolone administration was not associated with such infections [38].
Increasingly identified in ICU MDRO outbreaks that are difficult to eradicate are Acinetobacter spp. These organisms are strictly aerobic gram-negative coccobacilli that are ubiquitous and deeply entrenched in the environment, making them difficult to eradicate because of their persistence in multiple locations. Air induction and delivery systems have been well characterized as reservoirs in the ICU, as have fans used for topical cooling and general air circulation and ventilator circuit tubing [84]. Unlike Pseudomonas, Acinetobacter is implicated equally often in hospital-acquired and community-acquired infections [85]. Risk factors for MDR A. baumannii infection in the surgical ICU include, but are not limited to, higher Acute Physiology and Chronic Health Evaluation II score (10% increase in incidence of infection per point), longer endotracheal intubation for ventilation (40% increase in infection risk per day), prolonged antibiotic prophylaxis [62], bronchoscopy, chronic obstructive pulmonary disease (COPD), fluoroquinolone (levofloxacin) exposure, and azole administration (fluconazole) [86]. Whereas one cannot control how sick the patient is on presentation or the presence of COPD as a co-morbidity, the clinician has some influence on the duration of mechanical ventilation, endotracheal intubation, and utilization of bronchoscopy and complete control over the use of specific antimicrobial agents. Accordingly, it is imperative to explore how one may optimize antibiotic prescription practices to maximize therapeutic efficacy while minimizing selection pressure for multi-drug resistance.
Antibiotic Optimization Strategies
Antimicrobial prescriptions for patients in the ICU generally begin as empiric therapy. Whereas the initial regimen of choice may be clearer for those with community-acquired infection, nosocomial infection may be more problematic because of the breadth of coverage likely to be required. To optimize that therapy, specific fundamental principles have been articulated for empiric therapy of serious nosocomial infections: Timeliness, appropriateness, pharmacokinetic and pharmacodynamic (pK/pD) dosing principles, and tailoring [87–89]. These principles are explored below.
Antimicrobial agents should be delivered in a timely fashion, as more rapid administration correlates with better outcomes. “Appropriateness” means that all pathogens are susceptible to at least one of the antimicrobial agents. Agent selection should flow from institution- and unit-based epidemiologic data (i.e., an antibiogram) utilizing known susceptibility profiles of pathogens commonly identified in that location (body site, geographic site within the facility). Dosing regimens should be in concert with pK/pD data and may be influenced by changes in the volume of distribution, total body mass [90], and concomitant therapies that alter drug clearance (e.g., renal replacement therapy). “Tailoring” refers to the planned de-escalation [91] or discontinuation of therapy in response to clinical effect and microbiologic data. Perhaps most important is the recognition of “no infection” and the timely discontinuation of a broad-based empiric regimen akin to the data and practices derived from the bronchoscopic diagnosis of pneumonia; such precise data allow the clinician to have confidence in the diagnosis of “no pneumonia” [91–93]. The principles articulated above are part of “antibiotic stewardship” and are designed to improve patient outcomes related to infection and anti-infective therapy.
An antibiotic stewardship program also prescribes tactics to control resistance emergence and spread. A cornerstone of any such program is better infection control spanning barrier precautions as well as before-and-after hand hygiene programs using an alcohol-based gel or foam agent (except for C. difficile infection, which requires soap and water coupled with good hand-washing technique) [94]. A somewhat controversial strategy is the de-restriction of certain agents in a hospital formulary to reduce the selection pressure for resistance generated by the density of use of a particular agent or combination of agents. Planned rotation of empiric agents between classes rather than within a single class (and mechanism of action) is another means to help control resistance. Engaging in an antibiotic cycling program to codify how empiric agents are selected to support antibiotic heterogeneity is an effective means of reducing resistance pressure [95]. Planned tailoring after 72 h of empiric therapy or discontinuation as appropriate further solidifies an integrated resistance control effort in the ICU [65,88,96]. The underpinnings of antibiotic stewardship suggest that regimented, inflexible programs of specific antibiotic restriction or prioritization drive frequent use of a limited number of agents, which encourages and supports the genesis and spread of MDR pathogens. One useful alternative is to have a planned means of utilizing several antibiotics in a programmed fashion to generate antibiotic heterogeneity and reduce selection pressure for resistant pathogens [92,95].
Heterogeneity and gram-positive pathogen coverage
Glycopeptides form the foundation of empiric gram-positive pathogen coverage for nosocomial infection in many ICUs. As a result, and partly in response to the prevalence of resistant gram-positive organisms, the Hospital Infection Control Practices Advisory Committee of the CDC has articulated recommendations for “prudent” glycopeptide use as one means of controlling resistant pathogen genesis and spread [97]. Previously, the lack of appropriate alternatives to vancomycin led to a dearth of studies addressing heterogeneity for the control of gram-positive pathogens. Antimicrobials such as linezolid and quinupristin-dalfopristin that target resistant gram-positive pathogens specifically have enabled such studies to be conducted. In one such investigation in a surgical ICU, cycling a glycopeptide (vancomycin) with a non-glycopeptide agent (linezolid) had a salutary effect on overall ICU infection rates, as well as on infections specifically attributed to MRSA or VRE [98]. Importantly, this study highlights the fact that an antibiotic management scheme that cycles two classes of agents can meet individual patient needs for effective antibiotic therapy as well as address public health concerns about the adverse consequences of antibiotic use that are being reported with increasing frequency. The clinician might expect that such a straightforward intervention would decrease antimicrobial resistance in gram-negative pathogens as well [95].
Heterogeneity, gram-positive and gram-negative pathogen coverage, and heterogeneity index
A prospective cohort study spanning 44 months was undertaken in a single ICU to address the value of antibiotic heterogeneity in preventing the development of MDR pathogens [99]. The authors compared the impact of four antibiotic prescription strategies for the management of ventilator-associated pneumonia (VAP) on microbial ecology in a mixed medical–surgical ICU, and ranked the heterogeneity of each regimen using a “heterogeneity index.” The time periods were as follows:
1. Months 1–10 were characterized by the usual practice in which antibiotics were patient-specific, and multiple agents were permitted. Agent selection often was related to the duration of hospitalization and prior antibiotic exposure. 2. Months 11–22 were termed a “prioritization period.” Anti-pseudomonal antibiotics were implemented in the following order: Carbapenem, cephalosporin, and a beta lactam/beta-lactamase inhibitor combination. 3. Months 23–34 were termed a “restriction period.” The three aforementioned anti-pseudomonal antibiotics were restricted but in reverse order. Of note, an anti-pseudomonal fluoroquinolone or aminoglycoside was added to the regimen if there was high suspicion of P. aeruginosa. 4. Months 35–44 were termed a “mixing period.” The first-line anti-pseudomonal agent was changed in consecutive patients following a prescribed scheme (carbapenem→lincosamide plus cephalosporin→beta-lactamase inhibitor combination→reinitiate the cycle with the carbapenem). This scheme ensured equal use among patients requiring therapy.
In this study of nearly 3,000 patients, significant increases in carbapenem-resistant A. baumannii were noted during the carbapenem prioritization period. Greater numbers of Enterobacteriaceae were recovered, with an increase in ESBL-producing isolates noted during prioritization that returned to baseline with restriction and mixing. Smaller increases were noted in the number of P. aeruginosa isolates without any increase in MDR-isolates. An upstroke in E. faecalis isolates also was noted during prioritization that likewise returned to baseline during the remainder of the study. Of note, S. aureus isolates remained stable with no change in the likelihood of MRSA isolate recovery throughout.
This study's greatest value may be identified by exploring the “heterogeneity index” of each period. The antibiotic heterogeneity index (AHI) is a measure of the diversity of antibiotic use for any period of interest. Perfect heterogeneity generates a value of 1.0, with lower values indicating greater (presumably undesirable) homogeneous antibiotic prescription practice. Both the patient-specific initial 10 months (AHI 0.93) and the mixing period of the last 10 months (AHI 0.95) generated an AHI close to unity. The AHIs for each agent or regimen during prioritization and restriction were lower than in the first and last 10 months, and spanned 0.53 to 0.79, indicating a less heterogeneous prescriptive practice. It is important to note that multiple interventions may have been occurring at the same time in this single-center study, and significant increases in total antibiotic use were identified during the prioritization (6%) and restriction (18%) periods. Whereas it appears that a certain proportion of dissimilarity in prescribed antibiotics must be reached to garner the benefits of antibiotic heterogeneity, the AHI is a potentially useful tool in evaluating a given ICU's antibiotic practice paradigm with regard to quality improvement. This study did not employ genotyping techniques that are part of the tool set that may be brought to bear on specific outbreaks in a quality improvement approach.
A related study addressed the development of resistant gram-negative bacilli using a hospital-wide antibiotic heterogeneity management program [100]. The approach included a yearlong development period to establish a robust infection control program. There was a six-month period of some antibiotic intervention, followed by a rigorous 18-month domain of Periodic Antibiotic Monitoring and Supervision (PAMS) by a team comprising two infectious disease physicians, a pharmacist, and a dedicated infection control nurse that benefited from periodic input by a microbiologist. The PAMS team intervention for suspected or proved gram-negative infection came at the request of the prescribing physician, in the presence of gram-negative bacteremia, or when isolate resistance to two or more classes of supervised antibiotics was identified. Antibiotics were changed every three months and were either recommended, restricted, or off-supervision. Determinations were made by calculating the relative antibiotic usage density (%AUD), defined as the daily doses of a supervised class divided by the cumulative doses of all six classes. Low-use classes (%AUD<12.5%) were recommended in the following three months for all classes except carbapenems. Frequent use (%AUD>20.9%) led to restriction in the next three-month cycle. The PAMS team also restricted an agent for the next three-month cycle if P. aeruginosa resistance to that class increased >15%. Off-supervision classes were characterized by a %AUD between 12.5% and 20.9%. These thresholds were not random, but rather were designed specifically to achieve an AHI>0.85.
The hospital-wide program was an unqualified success in that the percentages of resistant gram-negative bacilli, MDR P. aeruginosa, and MDR gram-negative bacilli as a function of total gram-negative isolates decreased significantly during the period of intense PAMS activity. The pre-establishment and preparation period that preceded PAMS achieved a decrease in P. aeruginosa-mediated patient infections, but PAMS did not impact the proportion of patients with ESBL-producing organisms. Interestingly, no VRE was isolated during any time period. The resistance rates of P. aeruginosa to imipenem-cilastatin, ciprofloxacin, piperacillin-tazobacam, cefepime, and gentamicin were all impacted favorably by the end of the three sequential PAMS six-month intervention periods (total 18 months). Tracking the AHI during the study periods, one finds the following values: Pre-establishment (0.657), preparation (0.737), PAMS 1 (0.841), and PAMS 2/3 (>0.85). Thus, the study's articulated method of promoting, restricting, or not supervising (but monitoring) antibiotics on a class-by-class basis is another useful strategy to control resistance and achieve a heterogeneous antibiotic prescription practice. Recognizing the benefits of a heterogeneity program, one must determine how best to deploy such a program within a given institution. Useful lessons may be garnered from the “bundle approach” that has been successful in the management of sepsis and reduction of VAP [101,102].
Deploying an Antibiotic Heterogeneity Program
One approach to deploying an antibiotic heterogeneity program is to utilize the “care bundle” approach. This bundle embraces the data that have been reviewed above to promote an integrated approach to antibiotic management. Four key principles have been identified: (1) Use the fewest agents initially to treat the likely pathogens; (2) encourage prudent use of cephalosporins (especially the GC-3 agents), fluoroquinolones, and clindamycin; (3) re-evaluate the empiric regimen as culture data accrue but no later than 72 h after the start of therapy; and (4) optimize dosing (including duration of therapy) on the basis of patient characteristics, causative pathogen, infection site, and pK/pD of the prescribed agent(s) [103–107].
Not uncommonly, in concert with deploying a new antibiotic management program, one must address existing non-evidence-based but perhaps ingrained practices, which influence the antibiotic management that is to be replaced with a stewardship program. One such belief set is that of “double coverage,” especially of gram-negative pathogens, using combination therapy regimens, as explored above. Regardless of the setting, substantial change in antimicrobial prescription practice undoubtedly is a challenging task, but one that is incumbent on all healthcare providers to reduce the driving pressure and selection of MDR gram-positive and gram-negative pathogens alike as one means of enhancing patient outcomes.
Conclusions
Antibiotic resistance is an increasingly prevalent global problem. The major increases in the prevalence of MDRO pathogens that have been noted are related in large part to antibiotic prescription practice and geographic mobility of patients and healthcare providers. Careful evaluation of the data demonstrates that traditional practices such as combination therapy are ineffective in reducing MDR pathogen emergence. Whereas prophylactic antibiotic use may be driven in part by regulatory agency imperatives, therapeutic courses of antimicrobials are tied strongly to MDRO selection pressure. In conjunction with modifications of existing antimicrobial prescription practices, all successful methods of addressing MDR rely on a strong infection control program. Tools such as deoxyribonucleic acid fingerprinting may supplement standard investigative methods to evaluate the clonality of MDRO outbreaks and further refine infection control practices. Evaluating current antibiotic prescriptive practices with structured tools such as the AHI may allow precise exploration of a single institution's practice paradigm with regard to the genesis of MDRO pathogens. Careful design of an antibiotic heterogeneity program that is tempered by local microbial ecology is one successful tactic to reduce selection pressure and control both gram-positive and gram-negative MDR pathogens.
Footnotes
Author Disclosure Statement
No competing financial interests exist.