
Abstract
Abstract
Background:
In the aftermath of a devastating earthquake in early 2011, Haiti fell victim to an outbreak of cholera that claimed thousands of lives and affected populations in nearby Dominican Republic, Venezuela, and even the United States. This was the first time cholera had been reported in Haiti in more than 100 years. The sudden appearance of cholera, a pathogen with no known non-human host, raised the question of how it was introduced to an island that has long been spared this disease. The purpose of this review is to provide an overview of the history of cholera, its pathophysiology and virulence factors, and current recommendations for treatment.
Methods:
Articles published in the past 10 years were identified by a search of the medical literature using PUBMED and reviewed. Bibliographies of each article also were reviewed for additional pertinent articles.
Results:
The recent epidemic was caused by a strain that has been responsible for disease in South Asia since 1961, the seventh and most recent strain identified since 1900. It is transmitted by the fecal–oral route. Once infected, the patient develops a rapidly dehydrating diarrheal illness caused by the cholera toxin, which activates cytoplasmic adenylate cyclase of the intestinal epithelial cells by adenosine diphosphate (ADP)-ribosylation of the stimulatory G protein. The high cyclic adenosine monophosphate (cAMP) concentrations activate the cystic fibrosis transmembrane conductance regulator, causing a dramatic efflux of ions and water from infected enterocytes and leading to watery diarrhea. The first line of therapy is oral hydration with intravenous fluids; antibiotics are reserved for patients with severe dehydration. Spread of cholera is preventable with simple modifications of hygiene and water preparation.
Conclusions:
Cholera has re-emerged as a major infectious disease in the recent past, with a global increase in its incidence. Vaccination should be considered as an adjunct for controlling the epidemics and also for volunteer health care workers who provide services to underdeveloped nations. During an epidemic such as occurred in Haiti, use of antibiotics should be considered for all hospitalized patients. These endeavors should proceed in concert with much-needed improvements in sanitation and accessibility of potable water.
Infection with cholera is an acutely dehydrating diarrheal illness affecting three to five million people and causing 100,000 to 130,000 deaths per year [1]. Cholera is rarely transmitted person to person but rather via contaminated water or foodstuffs. The symptoms of cholera can, in most cases, be treated effectively with fluid rehydration therapy, electrolytes, and antibiotics; but if not recognized early, cholera infection can be fatal rapidly.
Vibrio cholerae is a motile, curved, rod-shaped, gram-negative bacterium whose toxicity is mediated by the cholera enterotoxin (CTX), an oligomeric complex of six protein subunits. This protein induces derangement in electrolyte transfer in intestinal mucosal cells via cyclic adenosine monophosphate (cAMP) production. Traditionally, strains of V. cholerae are classified into serogroups on the basis of outer-membrane antigen structures and into biotypes based on biochemical testing. There have been seven pandemics of cholera recognized historically, including the most recent one (El Tor biotype, serogroup 01) that first appeared in Indonesia in 1961. This strain reached the Americas in 1991. In the wake of the Haitian earthquakes, an already weakened infrastructure (specifically, the failure of sanitation and water management systems) provided the opportunity for contamination of the water supply. Forensic infectious disease methods, including real-time deoxyribonucleic acid (DNA) sequencing, have been used to compare and isolate specific strains that have implicated the human introduction of a Southeast Asian strain as the likely inciting factor for the Haiti epidemic.
Prevention of this disease involves basic and simple modifications in food preparation and sanitation and should be undertaken to avert devastating epidemics in the future. This review updates the history, pathophysiology, epidemiology, clinical aspects of treatment, and tactics for reducing the spread of cholera.
History
Cholera is and has been endemic to south Asia, especially the Ganges delta region, since the beginning of recorded history. Epidemic cholera was described in 1563 by Garcia del Huerto, a Portuguese physician at Goa, India [2]. The first pandemic occurred in 1817, with spread of the disease outside the Indian subcontinent along trade routes as far west as southern Russia. The second pandemic began in 1826 and reached Europe by the early 1830s. When the infection reached the United Kingdom in 1831, the government's response led to the establishment of local Boards of Health and a “Cholera Gazette,” which served as a clearinghouse for tracking the epidemic [3].
At that time, cholera was believed to be spread by the “miasma” (like a fog) coming from the river, but the classic 1854 epidemiologic study of John Snow, a surgeon from London, revealed the association of the disease with contaminated drinking water—before bacteria were known to exist. A New York cholera epidemic led to the creation of the first Board of Health in the United States in 1866, and cholera became the first reportable disease. In 1883, Robert Koch isolated the causative microorganism from the intestinal discharge of infected patients and proved conclusively that it was the agent of the disease. Three more pandemics ensued, the latest of which continued up to 1925 and involved Africa, Australia, Europe, and all the Americas [4].
The current (seventh) pandemic began in Indonesia but has expanded globally. The causative strain was a biotype of V. cholerae serogroup O1 called El Tor, named for El Tor, Egypt, the site of a quarantine station where the bacterium was isolated in 1905 from Indonesian pilgrims traveling to Mecca [5]. The El Tor serotype spread to India in 1964, to Africa in 1970, to southern Europe in 1970, and to South America in 1991. In 1992, O139 Bengal, a newly described, non-O1 serogroup of V. cholerae, caused unusual cholera outbreaks in India and Bangladesh (Fig. 1).

Vibrio cholerae (O group 1 antigen). Reprinted with permission from Baron S, ed. Cholera, Vibrio cholerae O1 and O139, and other pathogenic vibrios. Medical Microbiology, chap 24. 4th edition. Galveston, TX. University of Texas Medical Branch at Galveston. 1996.
In April 1997, a cholera outbreak occurred among 90,000 Rwandan refugees living in temporary camps in the Democratic Republic of Congo. During the first 22 days of the outbreak, 1,521 deaths were recorded, most of which occurred outside healthcare facilities [4]. The epidemic in Haiti in 2010 is the first recorded outbreak in that country in 100 years.
Etiology
In the wake of the most recent outbreaks, debate rekindled about the origin and transmission of the offending cholera strain. We know that transmission of cholera is primarily by fecal contamination of food and water; it is rarely person-to-person. Interestingly, however, the bacterium lives naturally in both fresh and salt waters; fish and shellfish often are vehicles of transmission. To cause illness in an otherwise-healthy adult, about 100 million bacteria typically must be ingested [3]. However, various host factors influence the inoculum necessary for infection. The dose is less in persons with reduced gastric acid (for instance, those using proton pump inhibitors). Younger children also are more susceptible to infection, with the highest rates occurring in 2- to 4-year-olds.
There is evidence that susceptibility to cholera also is affected by blood type, with persons having type O blood being the most susceptible. The cystic fibrosis genetic mutation in humans may confer a selective advantage over cholera: Heterozygous carriers of the mutation (who are unaffected by cystic fibrosis) are more resistant to infection [6]. In this model, the deficiency in the cystic fibrosis transmembrane conductance regulator channel proteins causes interference with bacteria binding to the gastrointestinal epithelium, thus reducing the effects of an infection.
In the developed world, the cholera bacterium usually is transmitted through consumption of contaminated seafood, whereas contaminated water is more often the source of the bacterium in developing countries. Cholera has been found in only two animal populations: Shellfish and plankton. Coastal cholera outbreaks can follow zooplankton blooms, making cholera a zoonotic disease. Patients infected with cholera typically have profuse diarrhea, and disease transmission occurs when this highly liquid stool, historically referred to as “rice water,” contaminates water used by others. Drinking any contaminated water, eating any foods washed in the water, or consuming shellfish from the affected waterway can cause infection.
Both toxic and non-toxic strains of cholera exist naturally. Non-toxic strains acquire toxicity through bacteriophages that infect the bacteria. Until genetic sequencing allowed researchers to isolate the strain that caused the recent Haitian outbreak, the mode of transmission and route of introduction were sources of controversy. One contention was that climactic and local aquatic factors led to the outbreak (a theory that has been postulated in other outbreaks), but this idea was dispelled later [7].
Pathophysiology
Vibrio cholerae is a comma-shaped, gram-negative aerobic or facultatively anaerobic bacillus that ranges from 1 to 3 micrometers in length by 0.5 to 0.8 micrometers in diameter. It is identified easily by its unique, single, polar flagellum. Infection with V. cholerae appears to be limited to the mucosa of the small bowel of its host. Resistant to bile salts, V. cholerae can penetrate the mucus layer of the small intestine, possibly aided by secretion of neuraminidases and proteases (mucinases). The vibrios withstand propulsive gut motility by their own swimming ability and chemotaxis directed against the gut mucosa (Fig. 2.)
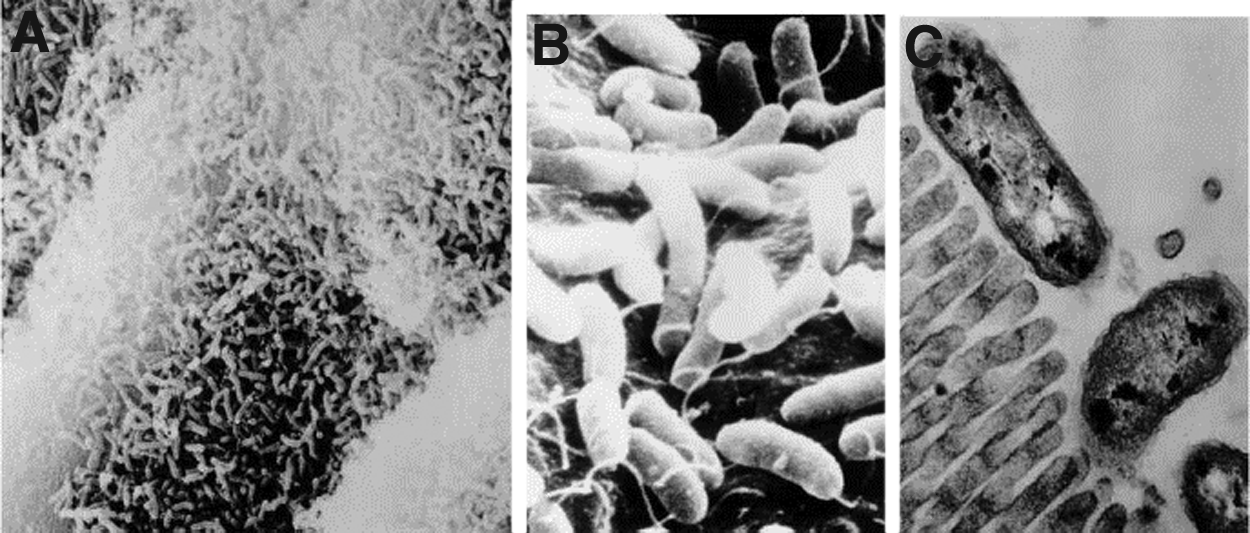
Vibrio cholerae attachment and colonization in rabbits. Events are assumed to be similar in human cholera. (
Specific adherence of V. cholerae to the intestinal mucosa is mediated by long filamentous fimbriae that form bundles at the poles of the cells. Once the bacteria pass from the stomach into the small bowel, there is upregulation of codons for the synthesis of both pili and enterotoxin. The vibrios elaborate CTX, a polymeric protein (Mr 84,000) consisting of two (A and B) major domains or regions. The A region (Mr 28,000), which is responsible for the biologic activity of the enterotoxin, is linked by disulfide bonds to the B region (Mr 56,000), which is composed of five identical non-covalently associated peptide chains of Mr 11,500 each. The B region, also known as choleragenoid, binds the toxin to its receptors on host cell membranes [8]. This also is the immunologically dominant portion of the toxin.
The structural genes that encode CTX reside on a transposon-like element in the cholera chromosome, in contrast to those for the heat-labile enterotoxins of Escherichia coli, which are encoded by plasmids. The amino acid sequences of these structurally, functionally, and immunologically related enterotoxins are similar. Their differences are responsible for variations in physicochemical behavior and antigenic distinctions that have been noted. There are at least two antigenically related but distinct forms of cholera enterotoxin, called CT-1 and CT-2. Classical O1 V cholerae and the Gulf Coast El Tor strains produce CT-1, whereas most other El Tor strains and O139 produce CT-2. V. cholerae exports its enterotoxin, whereas the E. coli enterotoxins occur primarily in the periplasmic space.
The molecular events in this and other diarrheal diseases involve an interaction between the enterotoxins and intestinal epithelial cell membranes. The toxins bind through region B to a host membrane glycolipid, the GM1 ganglioside, which is ubiquitous on eukaryotic cell membranes. The bacterium produces an invasin, neuraminidase, during the colonization stage. This has the interesting property of degrading gangliosides to the monosialosyl form, which is the specific receptor for the toxin. Following this binding, the A region or a major portion of it known as the A1 peptide (Mr 21,000) penetrates the host cell membrane and transfers ADP-ribose enzymatically from nicotinamide adenine dinucleotide (NAD) to a target protein, the guanosine-5′-triphosphate (GTP)-binding regulatory protein associated with membrane-bound adenylate cyclase (Fig. 3). The final effect of the subsequent cAMP-mediated cascade is hypersecretion of chloride and bicarbonate followed by water, resulting in the characteristic voluminous isotonic cholera stool, which can contain 20 L or more of fluid per day.
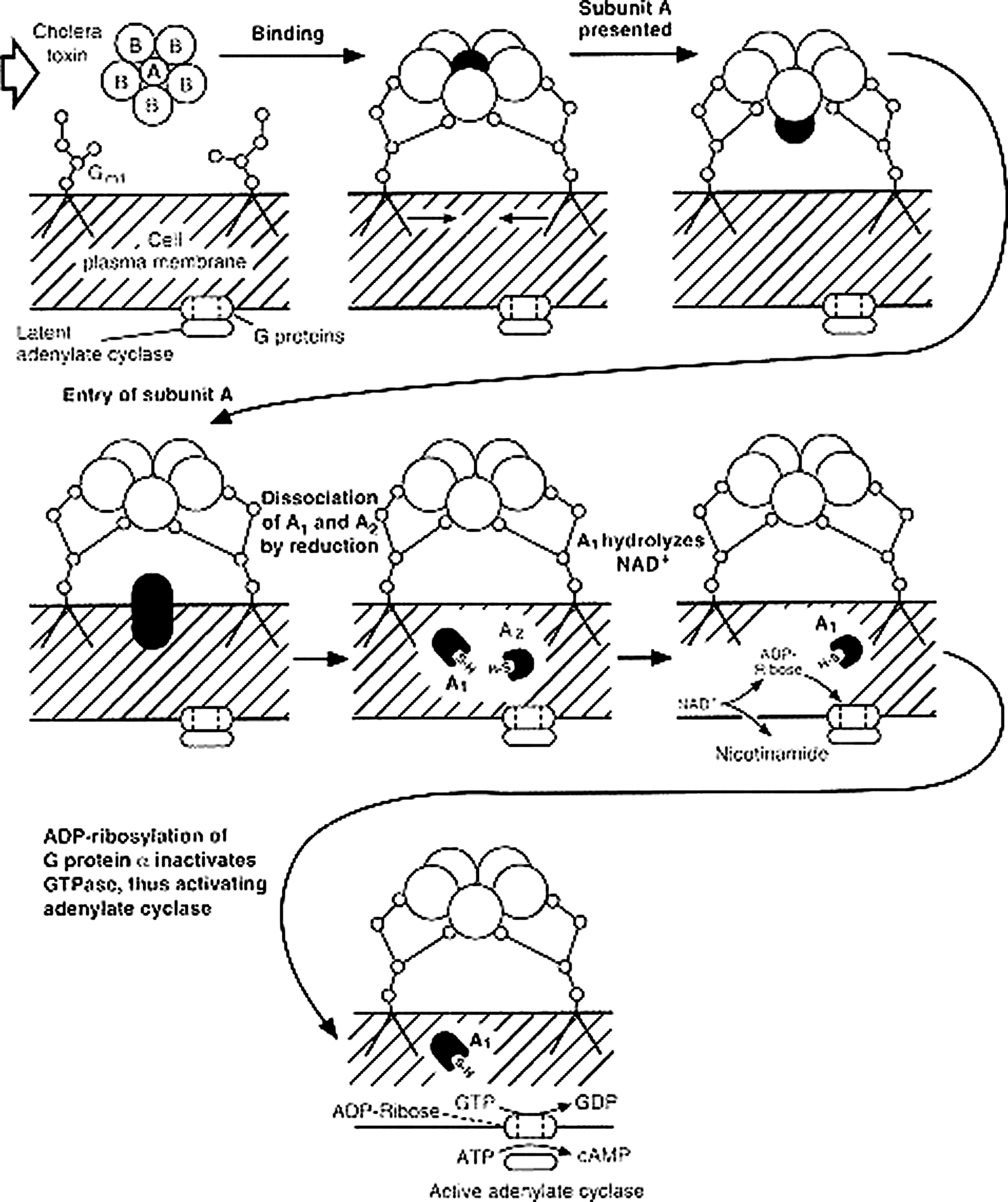
Mechanism of action of cholera enterotoxin. Toxin approaches target cell surface. The B subunits bind to oligosaccharide of GM1 ganglioside. Conformational alteration of holotoxin occurs, allowing presentation of A subunit to cell surface. The A subunit enters the cell. Disulfide bond of A subunit is reduced by intracellular glutathione, freeing A1 and A2. Nicotinamide adenine dinucleotide is hydrolyzed by A1, yielding adenosine diphosphate (ADP)-ribose and nicotinamide. One of the G proteins of adenylate cyclase is ADP-ribosylated, inhibiting the action of guanine-5′-triphosphate (GTP)ase and locking adenylate cyclase in the “on” mode. (Modified with permission from PH Fishman. Mechanism of action of cholera toxin: Events on the cell surface. In: Field M, Fordtran JS, Schultz SG, eds. Secretory diarrhea. Baltimore. Waverly Press. 1980:85.)
The stool of an actively purging, severely ill cholera patient resembles “rice water”—the supernatant liquid of boiled rice. Because the stool can contain 108 viable vibrios/mL, the patient can shed, or “purge,” 2×1012 colony-forming units into the environment per day. Relatively little is known about the extent to which a “carrier state” in asymptomatic human beings plays a role in disease transmission. Studies have identified two carrier states: Convalescent carriers, who continue to shed vibrios for weeks to months after symptoms have resolved, and chronic carriers, who can shed bacteria asymptomatically for years [9].
Epidemiology
Cholera has been studied closely since the birth of epidemiology, and it is still a subject of intense interest for modern-day epidemiologists. Tracking the spread of cholera has led to the development of new epidemiologic methods that have illuminated, not only cholera transmission but also the science of infectious diseases epidemiology. John Snow's seminal work on cholera was fundamental in many ways; he proposed methods and ideas that are still part of the foundation of modern epidemiology, such as time–spatial analysis and notions of source of exposure and incubation periods.
As we now know it, cholera is vastly underreported, with an estimated 3–5 million cases and 100,000–130,000 deaths annually [1]. Cholera is endemic in the developing countries of Asia and Africa and is responsible for epidemics in Asia, the Middle East, and South and Central America. In 2009, the number of cases of cholera reported to the World Health Organization (WHO) increased by 16% over the previous year (221,226 cases from 45 countries). Globally, the high incidence in the Americas in the early 1990s has shifted to a high incidence in Africa in the 2000s, with few cases in Asia.
Recent cholera epidemics include the 2008–2009 epidemic in Zimbabwe and the 2010 epidemic following the January earthquake in Haiti. In the United States, approximately 10 laboratory-confirmed cases of cholera are reported to the U.S. Centers for Disease Control and Prevention (CDC) each year. Of these infections, about one-half are related to travel outside the United States, and the remainder are acquired via consumption of contaminated seafood. Toxigenic V. cholerae infection was reported in Louisiana in October 2005, related to consumption of contaminated and improperly cooked seafood after Hurricanes Katrina and Rita.
The cholera strain responsible for the Haiti epidemic is nearly identical to the El Tor O1 strains predominant in Southeast Asia; the ancestry is distinct from the strains circulating in Latin American and East Africa, suggesting introduction of the strain from Asia. The same strain was identified subsequently in cholera cases in the Dominican Republic and in Florida. This finding was described in a study using third-generation, single-molecule DNA sequencing to sequence the genomes of two clinical cholera isolates from the current outbreak, one strain from an index case in Latin America in 1991, and two strains from South Asian cases reported in 2002 and 2008 [10]. Comparing these five strains, single-nucleotide variations and the presence of hypervariable chromosomal elements led to the conclusion that the Haitian strain was a variant of the South Asian El Tor 01 strain.
These techniques also have provided insight into genetic and phenotypic diversity among circulating strains that likely contribute to microbial mechanisms of pathogenicity and antibiotic resistance. These include the acquisition, loss, or alteration of mobile genetic elements, such as the CTX bacteriophage (which contains the genes that encode the toxin), genomic islands (previously mobile regions of chromosomes that have been acquired by horizontal gene transfer), and integrative/conjugative elements. Self-transmissible mobile genetic elements with plasmid-like and phage-like components also may be responsible for the transmission or reproduction of genes that encode antibiotic resistance [11].
The findings of these innovative epidemiologic investigations suggest that molecular determinants of fitness and resistance affect which strains become dominant in a given area. The revelation of the origin of the Haitian epidemic suggests that predicting future outbreaks will require assessment of both global and local risk factors.
Clinical Presentation
After ingestion of bacteria, there is an incubation period of between 18 h and five days, after which the onset of symptoms generally is abrupt. The predominant clinical features are sudden onset of painless, high-volume, watery diarrhea. The volume of diarrhea can exceed 250 mL/kg in the first 24 h [12]. The discharge has a characteristic appearance: Non-bilious, non-bloody, gray, slightly cloudy fluid with flecks of mucus. There is a somewhat sweet, inoffensive odor (hence the term “rice-water” stool).
Vomiting can occur, as well as muscle cramps. Typically, fever is absent. Signs of severe dehydration develop rapidly and include diminished peripheral pulses, poor skin turgor, sunken eyes, wrinkling of the skin on the hands and feet (as seen after prolonged immersion in water), and, eventually, hypotension. Patients can become restless and extremely thirsty, but as shock progresses, mental status may change, with effects ranging from agitation to obtundation (Table 1).
Repeat once if radial pulse is still weak or not detectable. Reassess the patient every 1 h and continue hydrating. If hydration is not improving, give the intravenous drip more rapidly. During the first 24 h of treatment, ≥200 mL/kg may be needed. After 6 h (infants) or 3 h (older patients), perform a full reassessment. Switch to oral rehydration solution if hydration has improved, and the patient can drink.
Many patients also show signs of metabolic acidosis with Kussmaul breathing. Most patients have oliguria or anuria until fluid losses are repleted. The fluid loss may be so rapid that the patient is at risk of death within a few hours of disease onset, and most deaths occur on the first day.
Several complications are possible, but these generally are sequelae of inadequate resuscitation. They include kidney injury from protracted hypotension, hypoglycemia, and electrolyte imbalance, especially hypokalemia.
Diagnosis
The diagnosis of cholera is confirmed through culture of a stool specimen or rectal swab. A number of media have been employed. Cary Blair medium is ideal for transport, and the selective thiosulfate–citrate–bile salts agar (TCBS) is ideal for isolation and identification. Cholera vibrios produce flat, yellow, nucleated colonies measuring 2–3 mm in diameter. Direct microscopy of stool is unreliable and therefore not recommended. Microscopy is preferred only after enrichment and reveals the characteristic motility of Vibrio species and its inhibition by appropriate antiserum. Diagnosis can be confirmed using serotyping by agglutination with specific sera.
A rapid dipstick test is available to determine the presence of V. cholerae in a rectal swab or stool specimen. Investigators have documented sensitivity and specificity exceeding 92% and 91%, respectively [13]. This test is still being validated by the WHO but would be an important development if it proves satisfactory, as it would lessen the current infrastructural requirements (i.e., microscopic evaluation, culture media) for diagnosis. Of note, a clinical diagnosis in the context of an epidemic may be made by taking a history and doing a brief examination [14].
Treatment usually is started without or before confirmation by laboratory analysis. Stool and swab samples collected in the acute stage of the disease, before antibiotics have been administered, are the most useful specimens for laboratory diagnosis. If an epidemic of cholera is suspected, the most common causative strain is V. cholerae O1. If V. cholerae serotype O1 is not isolated, the laboratory should test for V. cholerae O139. If neither of these organisms is isolated, stool specimens should be sent to a reference laboratory. Infection with V. cholerae O139 should be reported and handled in the same manner as that caused by V. cholerae O1. The associated diarrheal illness should be referred to as cholera, and U.S. cases must be reported to the CDC [15].
Treatment and Prevention
Perhaps the most frustrating element in the persistence of cholera as an epidemic is the ease with which it can be treated and cured if diagnosed early. The mainstay of treatment is fluid resuscitation. Close monitoring of fluid intake, urine output, and hydration status should be performed. Resuscitation is similar to that for any patient in hypovolemic shock. The first phase of rehydration should be completed within the first 3–4 h. This is followed by maintenance fluids at rates to match the continued losses. The route and speed of fluid administration will depend on the degree of dehydration. Patients with severe dehydration should receive fluids intravenously, as should those patients who do not tolerate oral rehydration solution (ORS). Ringer's lactate is the preferred intravenous solution, although normal saline may be used along with ORS [16]. For most patients with cholera, an ORS using one of the higher sodium-containing solutions and plain water optimally provide the fluid and salt needed (Table 1).
Antimicrobial therapy is indicated in moderately and severely ill patients to decrease the volume of fluids lost and to shorten the period of excretion of vibrios. The WHO guidelines for assessment and treatment are shown in Table 1. With effective antibiotic therapy, the duration of illness, excretion of toxin, and resuscitation requirement can be reduced by 50% [17].
Prior to the Haiti epidemic, WHO guidelines recommended antibiotic therapy only for those patients judged to have “severe” illness, described as volume loss >10%–20% of blood volume [18]. However, recent recommendations suggest that patients with both moderate and severe disease should be treated with an antibiotic, as recommended by the International Centre for Diarrhoeal Disease Research in Bangladesh. Tetracycline, doxycycline, ciprofloxacin, or azithromycin may be used as an adjunct to rehydration therapy for severely ill patients to reduce the rate of stool output, assuming sensitivity [19]. Resistance to nalidixic acid, sulfisoxazole, and trimethoprim–sulfamethoxazole has been observed in the Haitian strain and is a matter of concern. Anti-diarrheal medications are not recommended. Many anti-secretory drugs have been tried as adjunctive therapy; unfortunately, none is useful in the treatment of cholera.
Data are not available to determine whether direct patient contacts are protected when the index case is treated with an antibiotic; however, decreasing the purging time with antibiotic therapy has been hypothesized to decrease the extent of exposure, thereby decreasing the number of secondary cases [3]. Despite this theory, routine treatment of a community with an antibiotic, or mass chemoprophylaxis, has no effect on the spread of cholera and in fact can have adverse effects by increasing antimicrobial resistance.
Appropriate measures for the prevention of cholera consist mainly of providing clean water and proper sanitation to populations that do not yet have access to basic services. Health education and good food hygiene also are important. Communities should be reminded of basic hygiene behaviors, including the necessity for systematic handwashing with soap after defecation and before handling food or eating, as well as tactics for safe preparation and conservation of food. In addition, strengthening surveillance and early warning helps greatly in detecting the index cases and initiating control measures [20].
With respect to vaccination, use of the available parenteral cholera vaccine has not been recommended by the WHO because of its low protective efficacy and the high incidence of severe adverse reactions. An oral cholera vaccine (OCV) is available for travelers. This vaccine is safe and effective and can be given to individuals 2 years of age and older. It is administered in two doses 10–15 days apart with 150 mL of water. Its public health use in mass vaccination campaigns is relatively recent. Official WHO recommendations for its use in complex emergencies have been issued and state the following [21]:
OCV should always be used as an additional public health tool and should not replace usually recommended control measures such as improved water supplies, adequate sanitation, and health education. It needs also to be linked to strengthened surveillance and early warning. The current internationally available pre-qualified vaccine is not recommended once a cholera outbreak has started due to its two-dose regimen and the time required to reach protective efficacy, high cost, and the heavy logistics associated with its use.
Conclusions
Cholera has plagued mankind seemingly since time immemorial, costing countless lives and driving tremendous advances in epidemiology and knowledge of infectious diseases. The 2010 resurgence in Haiti in the wake of an earthquake inspired a great outpouring of global initiative and another opportunity to expand our understanding of this epidemic. As the global community responded with relief efforts, volunteers also became infected.
Specific recommendations for those planning on traveling to impacted communities worldwide include the following: (1) Refer to the WHO factbook/treatment guidelines for the most up-to-date country-specific treatment information; (2) consult a local infectious diseases or traveler's clinic for OCV; (3) plan to obtain or import a supply of ORS or lactated Ringer's solution and equipment for intravenous access, as may apply; (4) supplies of azithromycin and ciprofloxacin will be of use in protracted cases; and (5) be conscious of food and water preparation services in the area of your travel. Packaged food and bottled water may be safest and should be used if possible.
Footnotes
Author Disclosure Statement
No competing financial interests exist.