
Abstract
Abstract
Background:
Prolonged courses of broad-spectrum antibiotics are often cited as standard care for the prevention of infectious complications in thoracolumbar or sacral (TLS) fractures following penetrating abdominal trauma. Perforation of a hollow viscus in addition to a TLS fracture is believed to be associated with a high incidence of spine infection. Because over use of antibiotics is associated with an increasing prevalence of multi-drug-resistant organisms, this study seeks to define the actual risk of infection of the spine and need for antibiotics in patients with TLS fractures and intraperitoneal injuries following penetrating trauma.
Methods:
A retrospective review of 67 patients with penetrating abdominal trauma and concomitant TLS fracture was performed. Demographics, level of TLS fracture, associated spinal cord injury (SCI), need for operative intervention, presence of concomitant hollow viscus injury, and type and duration of antibiotic coverage were collected. In addition, associated infectious complications were reviewed. Spine infections were defined as spinal or paraspinal abscess, osteomyelitis of the spine, or meningitis. Intraabdominal infections were defined with imaging studies or positive peritoneal cultures.
Results:
Sixty-seven patients (mean age of 27 ± 9 years) had an exploratory laparotomy and one or more TLS fractures. Four patients died within 24 h and were excluded from further study. Thirty-eight patients (60%) had one or more hollow viscus injuries, 13 (21%) had solid organ injuries alone and 12 (19%) had a non-therapeutic laparotomy. All patients received perioperative antibiotics; 92% received 48 h or less of antibiotic prophylaxis and 62% received only 24 h of antibiotics. In one patient with an isolated solid organ injury there was a spine infection (1%).
Conclusions:
In this study, 92% of patients received antibiotics for 48 h or less with no increased incidence of spine infections. Bacterial colonization of the vertebrae was not higher in patients with penetrating gastrointestinal injury. There is insufficient evidence to support the use of prolonged antibiotic prophylaxis to prevent spine infection in patients with penetrating abdominal trauma and TLS fracture.
C
Antibiotic resistance continues to increase and contributes substantially to rising rates of nosocomial infection [4,5]. Increased measures for infection control and more judicious use of antibiotics are being advocated to avoid antibiotic resistance [5–7]. Yet beyond the standards set forth by Rabinowitz et al. in their guidelines for antibiotic use and duration in penetrating abdominal trauma, and the guidelines of the Surgical Care Improvement Project (SCIP), extended prophylactic antibiotic regimens for penetrating spinal trauma appear unwarranted [8,9]. We therefore conducted a retrospective study to define the risk of infection of the spine and the need for antibiotics in patients with penetrating abdominal trauma and associated TLS fractures.
Patients and Methods
With approval by our institutional review board, a retrospective chart review was conducted at an urban Level I trauma center from 2004–2011. Inclusion criteria consisted of patients >17 y of age with one or more TLS fractures who underwent one or more exploratory laparotomies following gunshot wounds. Patients were excluded from further study if they died within 24 h of admission.
Data on patient demographics, Injury Severity Score (ISS), total number of blood transfusions, level of TLS fracture, associated SCI, operative interventions, and intraperitoneal injury were collected. In addition, antibiotic use and associated infectious complications were reviewed both during study participants' in-patient stay and outpatient follow-up. Infections of the spine were defined as spinal or paraspinal abscesses, osteomyelitis of the spine, or meningitis, as diagnosed through positive cerebrospinal fluid (CSF) cultures or imaging studies. Intra-abdominal infections were defined through imaging studies or positive peritoneal cultures. Other infections on which data were collected included pneumonia, bacteremia, urinary tract infection, and surgical site infection. Pneumonia was defined through quantitative cultures containing more than 10,000 microorganisms of specimens collected by bronchoalveolar lavage. Bacteremia was defined by the growth in a blood culture of a microorganism that required antibiotic treatment. Urinary tract infection (UTI) was defined as the presence of more than 100,000 micro-organisms in a clean-catch urine specimen. Surgical site infection was defined by clinical signs of infection (erythema, induration, purulence) requiring intervention.
Antibiotic use was also evaluated. Prophylactic antibiotic use was defined as less than 48 h of appropriate perioperative, systemic administration of an antimicrobial agent. This was subclassified according to the number of doses given as one dose two or three doses (24 h), and 4–6 doses (48 h) based on a q8h schedule of dosing. Extended empiric antibiotic was that given for >48 h (>six doses). Therapeutic antibiotic use was defined as systemic antimicrobial therapy given for an infection with a confirmed source.
Data are expressed as mean±standard deviation (SD). Statistical analysis was done through analysis of variance (ANOVA) and the Tukey–Kramer test where appropriate. A value of p<0.05 was considered significant.
Results
Sixty-seven patients sustained gunshot wounds with a spine fracture and underwent a concomitant exploratory laparotomy for intraperitoneal injuries. The charts of all 67 of these patients were reviewed retrospectively. Most of the patients were male (90%), with a mean age of 27±9 y. All 67 patients had one or more TLS fractures, of which 30 (45%) were thoracic, 35 lumbar (52%), and 2 (3%) sacral. Twenty-nine patients had no SCI, whereas 34 patients (51%) had a SCI associated with their fracture, with approximately one-half of these SCIs being complete (18 complete SCIs, 16 incomplete SCIs). The overall mortality was 9% (n=7). However, four patients died within 24 h of injury and were excluded from further study. The mean follow-up of patients was 18 mo. Outpatient follow-up was documented for 74% of the patients. Patient characteristics of the study group (n=63) are summarized in Table 1.
All patients that were included in the study received systemic perioperative antibiotic prior to exploratory laparotomy. Thirty patients (48%) received only one dose of systemic antibiotic. An additional nine patients (14%) received two or three doses of systemic perioperative antibiotic (Figure 1). Nearly two-thirds of the study group received antibiotic for 24 h or less. An additional 30% of patients received systemic perioperative antibiotic for 48 h. Five patients (8%) received 7–15 doses (>48 h) of extended systemic empiric antibiotic (Fig. 1). Fifty-one patients (81%) received cetoxifin, 10 patients (16%) received cefazolin, one patient received (2%) nafcillin, and one patient (2%) received ampicillin-sulbactam.
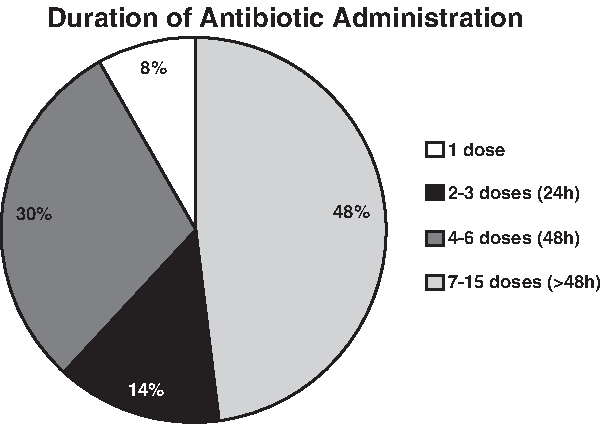
Duration of antibiotic administration in patients with thoracolumbar or sacral fractures of the spine following gunshot wounds.
On the basis of injuries identified during laparotomy, patients were divided into three groups, with 38 patients (60%) having one or more injuries to the gastrointestinal tract, 13 patients (21%) having a solid-organ injury alone, and 12 patients (19%) having a non-therapeutic laparotomy (Table 2). The distribution of gastrointestinal injuries is shown in Table 2. The subgroups with solid-organ injuries, gastrointestinal injuries, and non-therapeutic laparotomy were analyzed separately for the incidence of abdominal and spinal infection on the basis of findings at exploratory laparotomy (Fig. 2). Overall, 29% of the patients in the study had an intra-abdominal infection, of which 78% occurred in patients with injuries to a hollow viscus (Fig. 2). The patients with gastrointestinal injuries had no spinal infections. Only one spinal infection occurred in a patient with an isolated solid-organ injury, who had a complete SCI. There were no significant differences in intra-abdominal or other infections among patients with complete or incomplete SCI or without SCI. In terms of the duration of perioperative antibiotic administration according to type of injury, patients who underwent a non-therapeutic laparotomy received 1.4±1 doses of antibiotic (Table 3), patients with gastrointestinal injuries received an average of 3.6±3 doses of antibiotic, and patients who had solid-organ injuries received 2.8±2 doses of antibiotic (Table 3).

Incidence of abdominal and spine infections stratified by type of injury.
p<0.05 vs. non-therapeutic laparotomy.
Patients with gastrointestinal injuries had an average of 3±4 laparotomies and an average ISS of 28±11 points, and received an average of 14±23 units of blood and 5±9 units of fresh-frozen plasma during their hospitalization (Table 3). The group with solid-organ injuries underwent more laparotomies (4±5) and had a higher average ISS (33±10) but received fewer average blood and plasma transfusions (10±9 and 4±4 units) than did those without such injuries. The patients who had non-therapeutic laparotomies had 1±0.3 such laparotomies and an average ISS of 24±12 points, and received 5±12 units of blood and 2±4 units of fresh-frozen plasma. There were no differences in frequency of pneumonias, bacteremias, or UTIs in the three injury subgroups (Table 3); however, there was a higher frequency of surgical site infection in patients with gastrointestinal injuries (Table 3).
Only three patients (5%) underwent operative intervention for their TLS fractures. Of these patients, one had a non-therapeutic laparotomy, one had a gastric and colon injury, and one had a liver injury. No spinal infections occurred in patients who underwent spine surgery. Only one spinal infection (meningitis) occurred in a patient with an isolated solid-organ injury (liver). This patient had a number of infections and a complicated, prolonged hospital course. He had sustained gunshot wounds to the chest and abdomen resulting in a complete SCI at T6, right lung laceration, liver laceration, and injury to the common hepatic duct requiring cholecystectomy and repair of the duct. This patient had an ISS of 35 points and received five doses of perioperative cefazolin. He developed cholangitis and meningitis on post-operative day 10. His biliary and CSF cultures differed in the microorganisms they grew (biliary: Escherichia coli, Serratia spp., and Klebsiella pneumoniae; CSF: Propionibacterium acnes). He received a 14-d course of meropenem, after which his CSF cultures were negative. The patient had subsequent infectious complications including necrotizing fasciitis of his abdominal wall and retroperitoneum, necrotizing pancreatitis, colonic ischemia and perforation, multiple intra-abdominal abscesses, empyema in his left chest, and multiple UTIs secondary to neurogenic bladder. He received a total of 30 units of blood and underwent 20 laparotomies during his 211-d hospitalization.
Discussion
No current consensus or guideline exists for the appropriate duration of prophylactic antibiotic administration for patients sustaining penetrating trauma resulting in concomitant peritoneal injuries and TLS injuries to the spine. The orthopedic and neurosurgical literature on the spine advocates the use of extended antibiotic prophylaxis (7–14 days) for such patients [3]. This literature is based on retrospective studies and small case series, with predominantly low rates of spinal infections (Table 4). The true incidence of spinal infection in these patients is unknown, because all of the studies relating to this have been underpowered in terms of answering this question (Table 4). Our study found that patients who sustained gunshot wounds with peritoneal injuries and TLS fractures and who received systemic perioperative antibiotic for 48 h or less did not have an increased incidence of spinal infection. In fact, 62% of the patients in our study received an antibiotic for 24 h or less, and 48% received just a single dose of antibiotic without showing an increased incidence of spinal infection. In the subgroup of patients who had gastrointestinal injuries, the rate of intra-abdominal infection was a 37%, but there were no spinal infections in this group. Of the patients in this subgroup, 87% received systemic standard perioperative antibiotics for 48 h or less. Not only was there no greater incidence of spinal infection during these patients' inpatient stays, but in the 74% of patients who had outpatient follow-up (mean duration 18 mos) there were no reports of spine infection. The reason for this high percentage of outpatient follow-up was probably both the presence of SCI in 51% of the patients and the need for laparotomy. Therefore, there is insufficient evidence to support the use of extended prophylactic antibiotic administration in patients with penetrating abdominal trauma and TLS fractures of the spine.
Authors do not advocate any specific antibiotic course but state there is an increased risk of infection.
Our findings are supported by a recent retrospective review by Rabinowitz et al. [8], who also questioned the practice of extended antibiotic coverage in patients with gunshot wounds through the gastrointestinal tract and into the spine, and who advocated the use of an antibiotic for only 24–48 h. Their review of 51 patients with hollow-viscus injuries and spine fractures identified only one patient who developed a CNS infection, at four days after discharge, following a 2-wk course of piperacillin-tazobactam for an E. coli bacteremia [8]. Our results substantiate this management strategy. The patients in both studies were of similar gender and age, had similar ISS values, and similar mortalities. In their study, Rabinowitz et al. [8] had one instance of delayed spinal infection (2%), resembling the incidence of this in our study. In our study, the gastrointestinal injury group had a higher incidence of intra-abdominal infection (78%) than the solid-organ injury group, and a zero incidence of spinal infection, despite receiving only 3.6±3 doses of antibiotic. Overall, 87% of the patients in our study who had gastrointestinal injuries and TLS fractures received an antibiotic for ≤48 h without developing spinal infections. The gastrointestinal injury group had a high average number of blood transfusions, but despite this there was no greater incidence of spinal infection in this subgroup than in the other two subgroups. The one patient in our study who developed meningitis appears to be an outlier, because this patient had multiple, repeated infections throughout a prolonged course of hospitalization, suggesting that either uncontrolled intra-abdominal sepsis or underlying immunosuppression related to his complete SCI may have contributed to his poor outcome.
Most of the orthopedic and neurosurgical spine literature advocate the use of long courses of antibiotics. One of the earliest such publications, by Romanick et al. [2], is often cited as an argument against short-duration antibiotic therapy in spinal infection resulting from missile injuries. Their case series had a 35% incidence of spinal infection after gunshot wounds that caused hollow viscus injuries and TLS fractures in which operative spinal intervention was delayed. Most of the patients who developed their infections did so at 2–11 wks after initial injury and after antibiotic treatment had been stopped [2]. Of the seven patients stated to have spinal infections, only three had documented positive cultures [2]. The authors concluded only that there is an increased risk of infection of the spine in patients with injury to the colon and TLS fractures of the spine, and suggested watching these patients closely, and that they may benefit from early surgical debridement of the spine [2].
Kumar et al. [10] reported the use of antibiotics in a small series of patients who had colorectal injuries accompanied by injuries to the spine. Although no spinal infections were identified in these patients, the authors advocated 7 d of antibiotic administration to protect against the high load of contaminants resulting from colonic injury [10]. In a review of the management of gunshot wounds to the spine, Bono et al. [3] similarly recommended 7–14 d of antibiotic administration. Their review cited the case series described by Kumar at al. [10], and another report, of 42 patients with gunshot wounds to the spine accompanied by injuries to hollow viscera [11], for support of their practice.
The more recent trend in the literature has moved toward antibiotic prophylaxis of shorter duration for gunshot wounds to the spine [12–14]. Lin et al. [12] reviewed 29 patients with transperitoneal gunshot wounds to the spine and concluded that 5 d of antibiotics are sufficient to prevent infection. Twenty-one of the 29 patients in their review had parenchymal or non-colonic injuries to hollow viscera, of whom 17 received antibiotics for 5 d. Eight patients had colonic injuries, all of whom received antibiotics for at least 5 d. None of the patients in their study developed spinal infections [12]. Kihtir et al. [13], in a review of 21 patients with trans-abdominal gunshot wounds to the spine, advocated thorough irrigation of the bullet track and only 48 h of antibiotic administration. With this management protocol, there were no infectious spinal complications, even in those patients with colonic injuries [13].
Our study has a number of inherent weaknesses in being a single-center, retrospective review with a relatively small sample size that could be subject to type II error. Our conclusions are therefore only observational, and based on retrospective data. Similarly, all previous literature on the topic of antibiotic prophylaxis in patients with gunshot wounds to the spine consists of small case series and retrospective reviews, rather than randomized, prospective studies. Despite our small sample size, our study is among the largest of previous retrospective reviews of this patient population, except for the latest study by Rabinowitz et al (n=51 patients) [8].
In summary, this retrospective study found no evidence of a need for more than 48 h of perioperative antibiotic administration for preventing infections of the spine in patients with penetrating intra-abdominal injuries and spinal fractures. In fact, 62% of our patients received a perioperative antibiotic for only 24 h or less, suggesting that 24 h of antibiotic prophylaxis may be sufficient for patients with penetrating intra-abdominal injuries accompanied by spinal fractures. These conclusions are consistent with the current practice advocated in SCIP guidelines across the range of surgical disciplines.
Author Disclosure Statement
No competing financial interests exist.