
Abstract
Abstract
Background:
Melioidosis, a lethal infectious disease caused by Burkholderia pseudomallei, an important human pathogen in tropical regions, is notorious for its diverse clinical presentations.
Methods:
We report a case of a 55-year-old woman with a history of total abdominal hysterectomy with bilateral salpingo-oophorectomy for ovarian mucinous cystadenocarcinoma five years back, who presented with complaints of chest pain, abdominal distention, and breathlessness for one week. Ultrasound-guided aspiration of the peritoneal free fluid revealed a thick gelatinous material consistent with pseudomyxoma peritonei. Cytologic analysis of the aspirate was negative for malignant cells, but bacterial culture proved positive for Burkholderia pseudomallei.
Results:
She was started on ceftazidime, and she improved symptomatically and was discharged on oral doxycycline and chloramphenicol after three weeks of intravenous antibiotic therapy.
Conclusion:
This case is being reported to emphasize an unusual presentation of melioidosis and the significance of timely appropriate antibiotic therapy.
Case Report
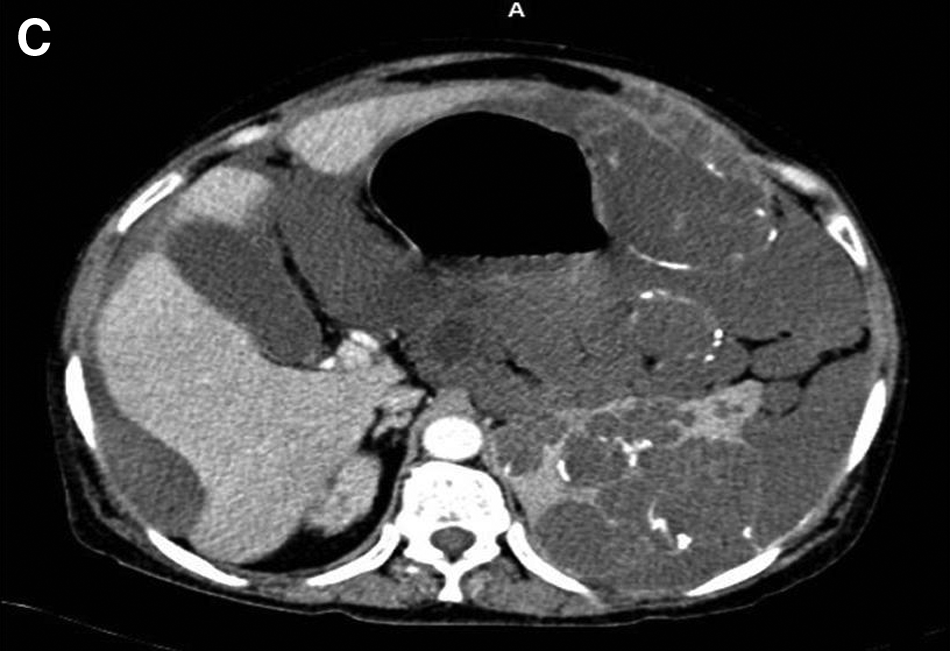
A 55-year-old woman presented to the emergency medical services of our hospital with chest pain, abdominal distention, and breathlessness for one week. She had undergone hysterectomy, bilateral salphingo-oophorectomy with infracolic omentectomy, and appendicectomy for ovarian malignancy five years previously; and the lesion was confirmed on histopathologic examination to be an invasive left ovarian mucinous cystadenocarcinoma. Ultrasonography showed echogenic ascites with multiple thick intra-peritoneal echogenic foci, a few having a star-burst appearance, in the right sub-diaphragmatic region scalloping the liver, with similar foci in the left retro-peritoneal region. Aspiration yielded thick gelatinous material consistent with pseudomyxoma peritonei. Contrast-enhanced computed tomography of the abdomen confirmed the diagnosis of pseudomyxoma peritonei (Fig. 1). Cytology examination was negative, but bacterial culture of the aspirated gelatinous material was positive for B. pseudomallei sensitive to ceftazidime and imepenem. She received intravenous ceftazidime for three weeks, during which she improved symptomatically and was discharged on oral doxycycline and chloramphenicol for four weeks.

Contrast-enhanced computer tomography of the abdomen in sagittal (
Discussion
Melioidosis, an infectious disease caused by B. pseudomallei that is endemic in Southeast Asia and northern Australia [1], is notorious for its varied clinical presentation, which can mimic any disease condition [2], ranging from an asymptomatic infection to fulminant sepsis with organ involvement. It is likely to be fatal if not treated appropriately [2].
Melioidosis with multiple organ involvement with or without suppuration has been reported to involve lung; skin and soft tissue; the skeletal, hepatobiliary, genitourinary, lymphatic, cardiovascular, and central nervous systems; the eye; and the parotid gland [3]. In non-endemic areas, the septicemic form, which is the commonest presentation [1], causes leukocytosis alone and frequently is missed. In young and healthy patients, abscesses and septicemia secondary to melioiodsis often are difficult to recognize. In acute presentations, the clinical and radiologic features cannot be discriminated from those of other pyogenic infections. Melioidosis always should be suspected whenever a chronic relapsing infection occurs in immuno-compromised individuals. On histopathologic examination, chronic melioidosis is composed of granulomatous lesions, confined to a single organ, with bacteria rarely being seen in tissue sections. Although B. pseudomallei usually is sensitive to chloramphenicol, trimethoprim/sulfamethoxazole (cotrimoxazole), ceftazidime, and imipenem, the last two agents are the first-line antimicrobial agents employed in treatment [4]. The minimum recommended treatment is a combination of ceftazidime with parenteral cotrimoxazole for three weeks in the acute septicemic stage, followed by oral cotrimoxazole for two months in the non-septicemic stage. The mortality rate of the acute disseminated septicemic form is close to 87% in patients not receiving prompt appropriate therapy [5]. A study that compared a four-drug combination (chloramphenicol, doxycycline, and cotrimoxazole) with ceftazidime alone demonstrated a 50% reduction in the mortality rate with the former [6]. In the sub-group with severe sepsis, the use of meropenem was associated with a lower mortality rate than was ceftazidime. The antibiotic therapy was defined as appropriate when patients receive effective antibiotics within 48 h; delayed antibiotic therapy when patients received effective antibiotics but beyond 48 h; and as no appropriate antibiotic therapy when no antibiotic effective against B. pseudomallei was given [7].
Pseudomyxoma peritonei was first described by Rokitansky in 1842 (cited by Weaver [8]), but the term was coined by Werth in 1884 [9], when he described this condition in a case of ovarian mucinous carcinoma. Often referred as “jelly belly” [10], this is an unusual condition more common in females, where diffuse collections of gelatinous fluid are associated with mucinous implants on the peritoneal surfaces and omentum. The rupture of a primary ovarian mucinous cystadenocancinoma or of metastatic cystic mucin-producing implants in the peritoneum or mucoceles of the appendix is often cited as the cause for this condition. It now is generally accepted that pseudomyxoma peritonei is caused by neoplastic mucus-secreting cells within the peritoneal cavity [11]. Carr believes that, because of the relentless growth of the cells, pseudomyxoma peritonei should always be classed as a malignant condition regardless of its other histologic features [12]. Thorough surgical debulking with removal of the appendix for histopathologic assessment is regarded as the mainstay of treatment [13]. Ultra-radical surgery in the form of systematic excision of affected peritoneal surfaces with diathermy and adjuvant intraperitoneal and systemic chemotherapy also have produced excellent results [14]. Our case was of intra-abdominal melioidosis causing mucinous ascites in an immunocompromised patient with a history of ovarian malignancy, who was initially considered to have pseudomyxoma peritonei. On the basis of the ascitic fluid culture, a diagnosis of intra-abdominal melioidosis was made, and the patient recovered with appropriate antibiotic therapy.
Conclusion
The importance of this case is to stress on the ability of melioidosis, a fatal yet curable condition, to mimic almost any clinical condition and the impact of a timely diagnosis and prompt and appropriate antibiotic treatment on the patient outcome.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest to declare.