
Abstract

To the Editor:

Magnetic resonance image showing pararenal collection in relation to the lower aspect of left kidney.
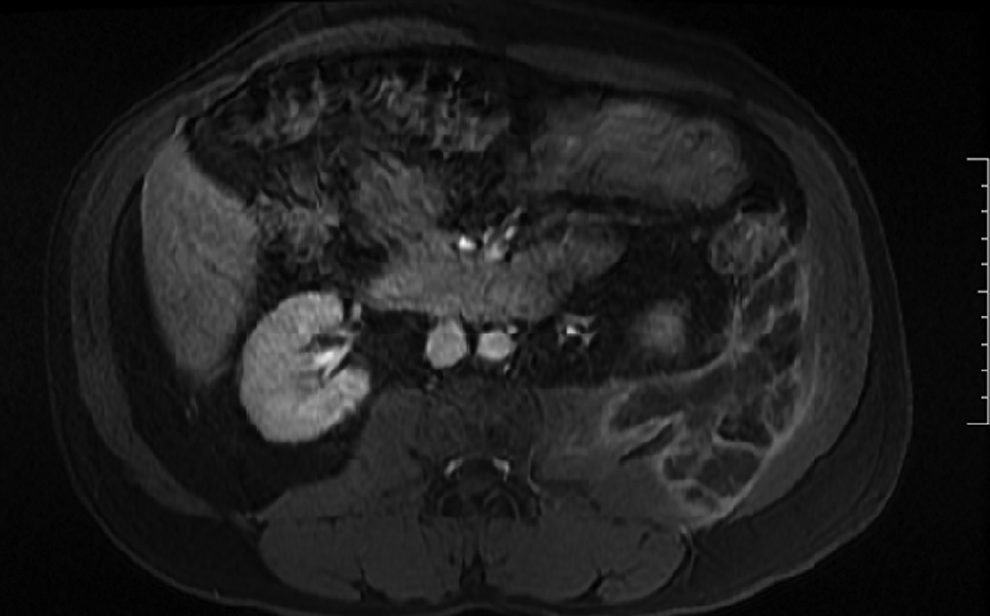
Magnetic resonance image showing pararenal collection extending to the left psuas, quadratus and adjacent oedematous abdominal wall.
The pus sample sent for culture yielded growth of non-fermenting gram-negative bacilli, identified by VITEK® 2 compact system (bioMérieux, Inc., St Louis, MO) as Achromobacter xylosoxidans with a 99% probability and an “excellent identification” confidence level. The isolate was susceptible to piperacillin, levofloxacin, co-trimoxazole, ceftazidime, cefoperazone-sulbactam, and meropenem, but resistant to aminoglycosides and tetracycline using Clinical and Laboratory Standards Institute (CLSI) break points for non-Enterobacteriaceae.
The drain was removed on the fifth post-operative day and the patient was discharged on oral levofloxacin and co-trimoxazole. Three days after discharge, the patient returned in sepsis with similar complaints and pus draining from the incision. On retaking the history, it was determined that the patient had stopped taking the antibiotics after discharge. On examination, his temperature was 101.6°F and he had tenderness of the left flank. Abdominal ultrasonogram showed minimal residual collection at the abscess site. A second incision and drainage was performed immediately under cover of intravenous cefoperazone-sulbactam. A small amount of purulent material was drained and the abscess wall was debrided. The benign-looking small cortical cyst towards the upper pole was left undisturbed on both occasions. After 1 wk of intravenous antibiotic and supportive therapy, the patient was discharged in good health on oral co-trimoxazole and levofloxacin for 2 wks. On clinic follow-ups at 1 mo and 3 mos, there was no evidence of any continuing infection or any local symptom or abnormal findings on imaging studies other than the unchanged cortical cyst.
Achromobacter xylosoxidans is a non-fermenting gram-negative, motile oxidase-positive bacillus belonging to the Alcaligenaceae family [1]. It is characterized by the ability to utilize xylose and glucose oxidatively. Identification using traditional phenotypic test often is unreliable and A. xylosoxidans can be mistaken for non-aeruginosa strains of Pseudomonas or for strains of Burkholderia cepacia complex. Achromobacter xylosoxidans is an opportunistic pathogen capable of causing nosocomial and community-acquired infections, with the source being either endogenous or from a contaminated aquatic hospital environment [2]. It frequently has been isolated from blood, cerebrospinal fluid, pus, and urine. Central venous catheters, mechanical ventilators, tubing of apparatus used for dispensing disinfectants (didecyl dimethyl ammonium chloride), and contaminated dialysis fluids have been implicated as sources of infection in many hospitalized patients [3]. It is also known to colonize and infect the respiratory tract in cases of cystic fibrosis [4]. Achromobacter spp. has been reported to cause abscesses in the liver [2], pancreas [5], urinary bladder [6], skeletal muscle [6], and aortic root [12]. A complicated intra-abdominal abscess caused by A. xylosoxidans following surgery in an acute cholecystitis patient was reported from Taiwan in 2009 [13]. The mortality rate ranges from 15% to 48% and is found to be high in patients with risk factors such as neutropenia, advanced age, nosocomial infection, and polymicrobial infection [3].
To the best of our knowledge, A. xylosoxidans infection as a cause of perinephric abscess has not been reported perviously. Moreover, this abscess occurred in the absence of any foreign body in an otherwise immunocompetent individual. There is one report of A. xylosoxidans causing pelvic and paravesical abscess about 25 years after hernia repair with mesh [6].
Achromobacter xylosoxidans shows high-level resistance to aminoglycosides, cephalosporins, and quinolone antibiotics. Our patient presented with the infection 2 y after de-roofing of a renal cyst. He is likely to have acquired a nosocomial strain of the pathogen during the operation. Perinephric abscess may remain silent and may be detected only during incidental imaging [9]. They usually occur because of parenchymal disruption as a consequence of raised intra-pelvic pressure caused by an obstructing stone. Hematologic dissemination may result in the formation of abscess in 30% of cases, which may rupture subsequently. The choice of therapy is to drain all but the smallest collection and correct any treatable underlying cause. For a large abscess with septae and loculation, a drain should be left in situ with repositioning as needed for complete evacuation. In culture-positive abscess cases, only 67% usually grow the same organism in urine or blood [10]. In our case, there was no simultaneous isolation of the pathogen from another samples. Apart from making the first report of a perinephric abscess due to A. xylosoxidans, our article also highlights the possibility of developing such an infection in the absence of any residual foreign body in an otherwise immunocompetent individual.