
Abstract

A 72-
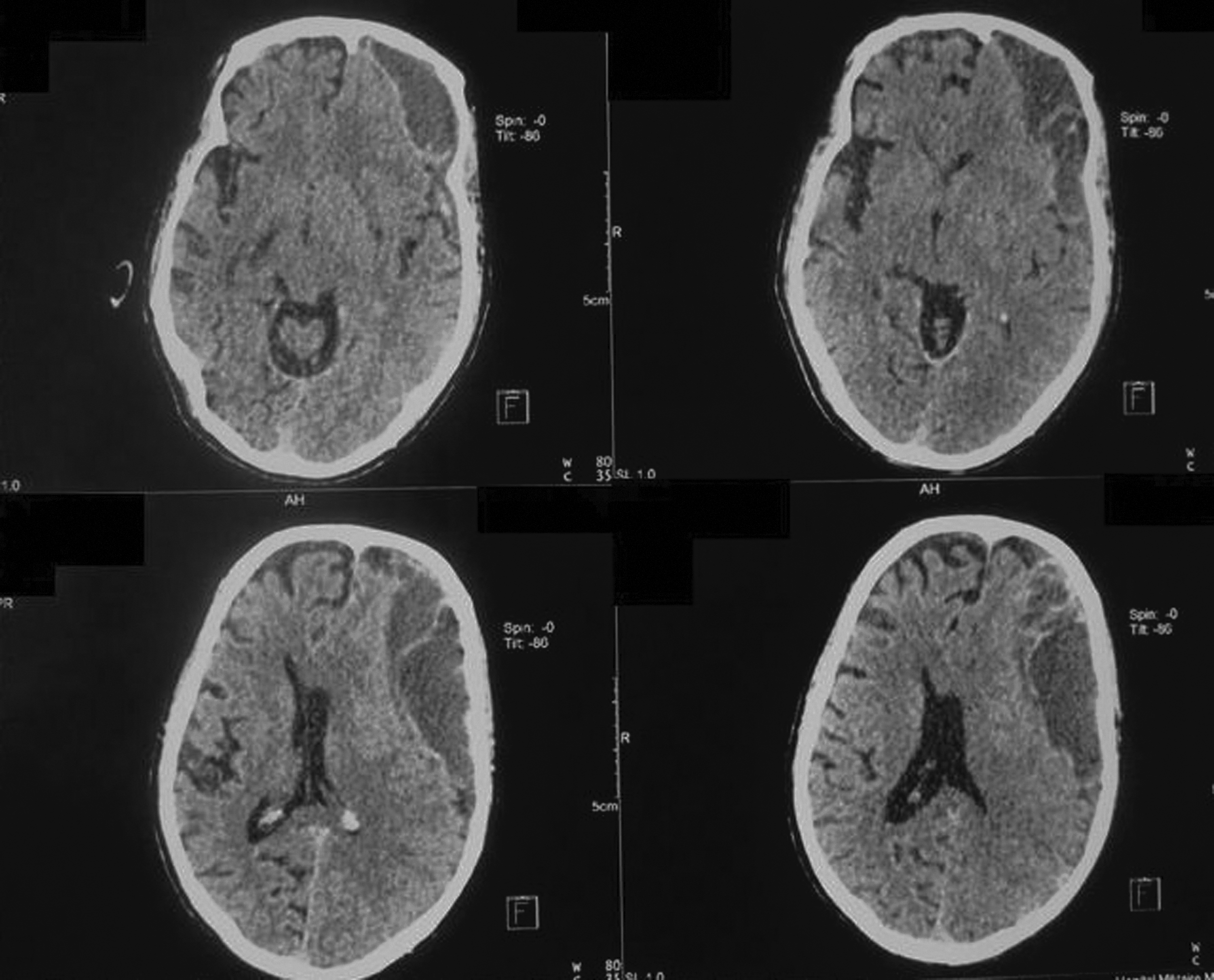
Initial cranial computed tomography scan, showing a large chronic subdural hematoma and a significant midline shift.

Intraoperative aspect of the patient's empyema with a thickened inner shell.
The fluid evacuated from the patient's head yielded sterile cultures, but in view of the earlier presence of C. fetus bactermia, gene amplification of a specimen of the fluid was done through the polymerase chain reaction (PCR) with specific primers, and confirmed the presence of C. fetus. The regimen of combined antibiotic therapy with amoxicillin (8 g/d) and clindamycin (1800 mg/d IV) was maintained for 3 wks, after which amoxicillin alone was continued without a change in dosage for an additional 3 wks. The patient's fever disappeared rapidly and his neurologic status became normal. His clinical improvement persisted with a satisfactory CT scan at 5 wks after surgical revision (the second intervention or the craniotomy) (Fig. 3).

Post-operative computed tomography scan showing evacuation of the patient's subdural collection.
Infection of a chronic subdural hematoma is rare, occurring in 1% of all such hematomas [1]. The case of our patient merits the discussion of infection of a hematoma as a mode of initiation of empyema. Campylobacter spp. is a gram-negative bacillus with trophism for the digestive tract. To our knowledge, five cases of chronic subdural hematoma infected by C. fetus have been reported [2]. The issue raised by this clinical presentation in our patient is the role of C. fetus in the onset, perpetuation, or aggravation of chronic subdural hematoma. The failure of the initial intervention of evacuation of the patient's hematoma was coincident with the reactivation of his C. fetus infection through the selection of organisms resistant to fluoroquinolones. In the first case of an infected subdural hematoma reported in the literature, in which the infecting organism was Escherichia coli, the patient did not benefit from antibiotic therapy and the organism was identified post-mortem [3].
A review of the literature shows the rarity of infection of chronic subdural hematoma by C. fetus. However, the frequency of such infection is probably underestimated because of the technical difficulty in identifying this bacterium. The organism initially isolated from our patient was a wild-type C. fetus sensitive to fluoroquinolones. However, the blood cultures done subsequent to this showed that the organism had become resistant to fluoroquinolones. This is probably explained by the infection of a subdural hematoma, which constitutes a profound reservoir of pathogens in a poorly vascularized milieu, setting the stage for the development of resistance to fluoroquinolones. In conclusion, the identification of a C. fetus isolate resistant to fluoroquinolones should suggest the existence of a deep vascular reservoir, including a chronic subdural hematoma in an elderly patient.