
Abstract
Abstract
Background:
The normal human intravenous endotoxin model has been used for more than 50 years. It was once considered a possible model of sepsis, but, because no infection is present, it is better described as a model of systemic inflammation. We demonstrate herein that at least three of four systemic inflammatory response syndrome (SIRS) criteria are achieved with the model.
Methods:
Otherwise healthy human volunteers were given Escherichia coli endotoxin 2 ng/kg intravenously. Vital signs were monitored, and blood samples were collected over time for assessment of white blood cells (WBCs), cytokines, counter-regulatory hormones, and monocyte receptors.
Results:
The means of three variables (core temperature, heart rate, WBC) met the SIRS criteria. Compared with baseline, cytokines were elevated acutely, with tumor necrosis factor-alpha (TNFα) exhibiting temporal primacy over the other cytokines. Counter-regulatory hormones (cortisol, epinephrine) also were elevated acutely. Finally, the monocyte cell-surface receptors cluster of differentiation molecule (CD) 11b and TNF receptor-II were elevated and decreased, respectively.
Conclusions:
The experimental human endotoxin model satisfies SIRS criteria and probably is best described as a model of Toll-like receptor 4 agonist-induced systemic inflammation.
Steve Lowry's research endeavors began in earnest in the 1970s at the NIH, where he was a Fellow with Doctors Steven Rosenberg and Murray Brennan at the Surgery Branch of the National Cancer Institute. It was during this time that Steve's curiosity and passion for science and research developed, so much so that Doctor Brennan subsequently invited Steve to join him at the Memorial Sloan-Kettering Cancer Center (MSKCC) in New York City. There, Steve completed a fellowship in surgical oncology and was appointed an assistant attending surgeon. While at MSKCC, Doctor Lowry's work and potential came to the attention of Doctor G. Tom Shires, then the Lewis Atterburg Stimson Professor and chair of surgery at CUMC. Doctor Shires recruited Steve as an assistant professor of Surgery and, while at CUMC, Steve blossomed fully as a scientist and researcher. After only three years, he was awarded an R01 grant that continued without interruption for 26 years, including 10 years with Method to Extend Research in Time (MERIT) status. At first, Doctor Lowry's research focused on nutrition and metabolism issues in normal human subjects and in burn patients, but broadened over the years into a multi-pronged approach that included in vitro cellular and whole-animal investigations as well as studies in intensive care unit (ICU) patients. The prong of research that Steve adopted and that became, perhaps, the mainstay of his laboratory was the human endotoxin challenge model, which is the focus of this paper.
Subjects and Methods
All studies were approved by and performed under the guidelines of the Robert Wood Johnson Medical School Institutional Review Board. After giving informed consent and being screened for normality by history and physical examination, healthy human volunteers, 18–35 years and of both genders, were given Escherichia coli O:113 endotoxin (kindly supplied through Doctor Suffredini at the NIH Clinical Center) intravenously (IV) at a dose of 2 ng/kg. The number of subjects evaluated is given in the legends to each of the figures. Symptoms were documented by questionnaires in which the following commonly experienced symptoms were listed: Headache, chills, muscle aches, ocular photosensitivity, and nausea or vomiting. Vital signs and blood samples were obtained at the time points indicated in the figures. White blood cells (WBCs) were counted by the clinical laboratory, and cytokine concentrations were quantified by sandwich enzyme-linked immunosorbent assays using recombinant standards. The plasma cortisol concentration (hydrocortisone) was measured by direct radioimmunoassay using a polyclonal rabbit antiserum. Expression of cluster of differentiation molecule (CD)11b and tumor necrosis factor receptor (TNFR)-II by blood monocytes was determined by two-color fluorescence flow cytometry. Data were analyzed by one-way repeated-measures analysis of variance (ANOVA) to determine statistical significance (p≤0.05).
Results
Symptoms
Symptoms (chills, myalgia, photosensitivity, nausea) were recorded and combined into an omnibus “symptom score” (Fig. 1). The mean symptom score at baseline (0 h) was zero. Substantial symptoms were manifested by 1 h after IV endotoxin administration, peaked at 2 h, and then declined until at least 6 h after endotoxin was given.
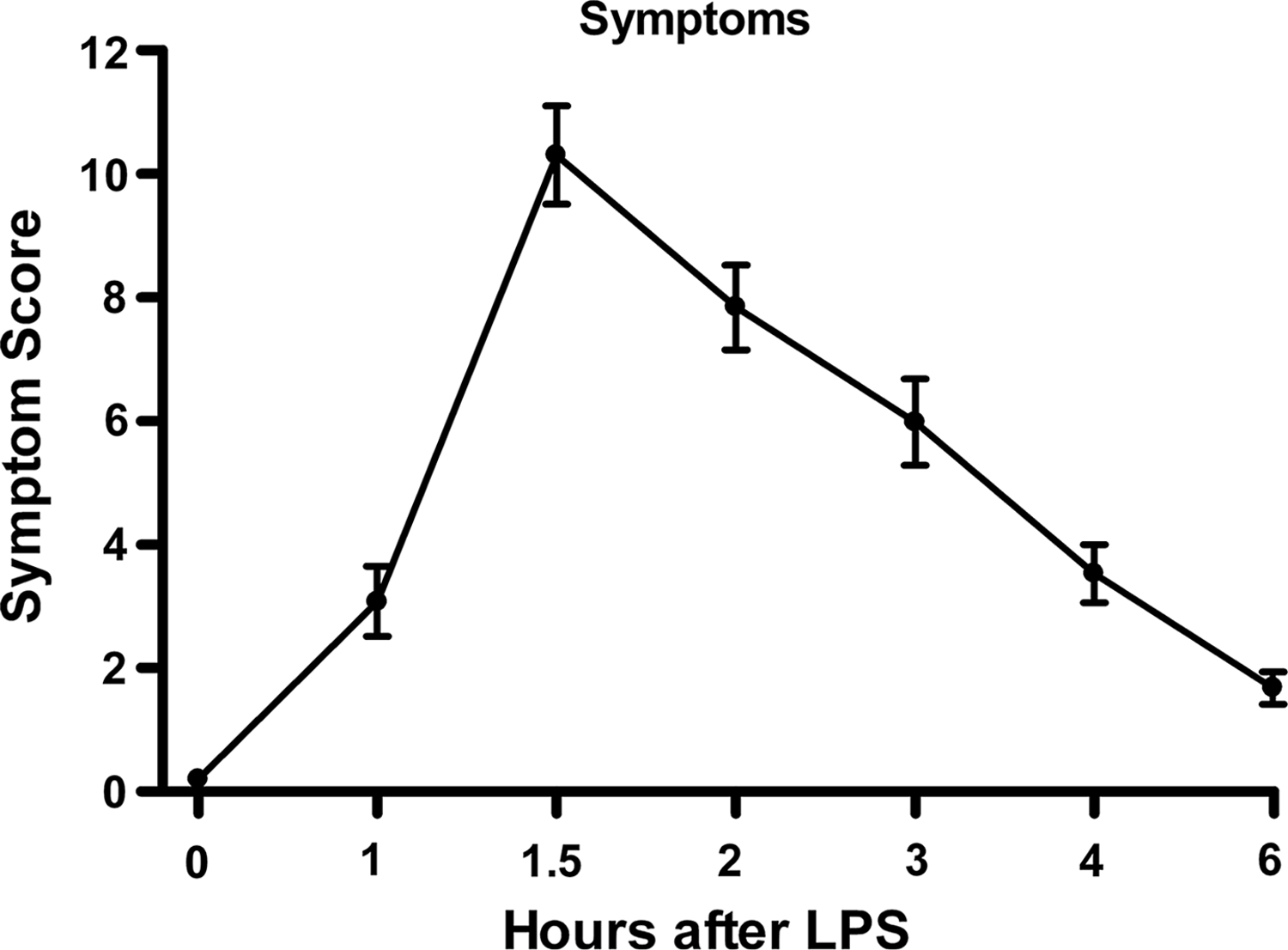
Omnibus symptom scores (mean±standard error) in normal human volunteers (n=66) receiving intravenous endotoxin. One-way repeated-measure analysis of variance was performed; endotoxin effect was significant at p<0.0001.
SIRS variables
The variables that comprise the SIRS definition according to the 1992 Consensus Conference “Definitions for Sepsis and Organ Failure and Guidelines for the Use of Innovative Therapies in Sepsis” [9] and reiterated and refined in 2001 [10] are temperature (hyperthermia or hypothermia), tachycardia, tachypnea, and abnormal WBC count (leukocytosis or leukopenia).
As shown in Figure 2A, the core temperature increased beginning as early as 1 h after endotoxin administration, with maximum temperatures attained at 3–5 h and resolution by 9 h. The maximum mean core temperature approached 38.5°C, above the SIRS criterion for hyperthermia (38.3°C). To meet the SIRS criterion for tachycardia, the heart rate must exceed 90 beats/min. As shown in Figure 2B, by 3–4 h after endotoxin injection, the mean heart rate met or exceeded this value and then diminished, although it had not normalized completely by the end of the 24-h study period. The respiratory rate (Fig. 2C) approached the SIRS criterion of 20 breaths/min by 4 h after endotoxin administration. However, the small number of subjects and relatively large variability among subjects make a definitive statement difficult as to whether the SIRS criterion for respiratory rate was satisfied. Unfortunately, PaCO2 data were not collected. The mean WBC count was ∼5,800/mm3 at baseline, decreased below the SIRS leukopenia criterion of 4,000/mm3, and then increased to more than 12,000 mm3 at 9 h post-endotoxin (Fig. 2D), thus also fulfilling the SIRS leukocytosis criterion for this parameter (12,000 mm3). Table 1 summarizes the fulfilment of the SIRS criteria, or lack thereof, after endotoxin administration for core temperature, heart rate, respiratory rate, and WBC number. Only the variable of respiratory rate may not meet the consensus criteria for SIRS in this model, although a Type II error cannot be ruled out in view of the small number of subjects. Fulfilling only two of the consensus criteria is sufficient to diagnose SIRS clinically.
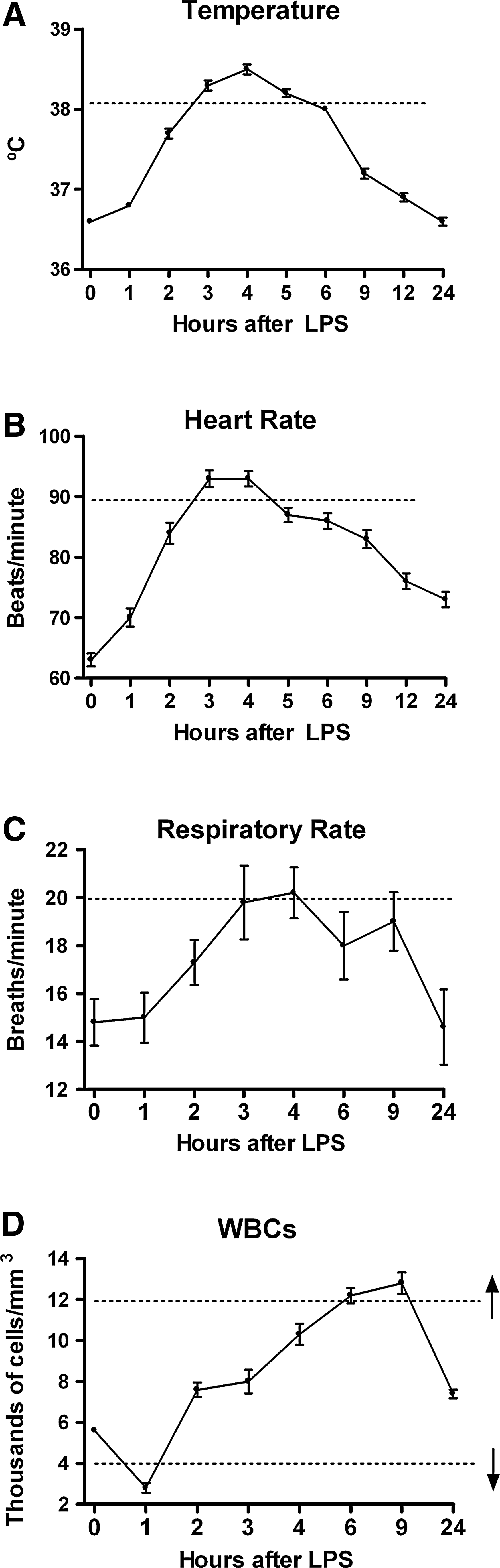
Response of systemic inflammatory response syndrome (SIRS) variables in normal human volunteers receiving intravenous endotoxin (LPS, 2 ng/kg) at time 0. (
Inflammatory mediators
Doctor Lowry and his colleagues and collaborators played a pivotal role in the discovery and characterization of several inflammatory mediators (e.g., cytokines, chemokines, interleukins [ILs]) [11–15]. Of special importance was the discovery of cachectin/tumor necrosis factor (TNF)-alpha, one of the most potent and proximal mediators, which is believed to be an important driver of the inflammatory response, as espoused in the cytokine theory of inflammatory disease [11,12].
Figure 3A depicts the plasma TNF-α response to endotoxin administration in normal human volunteers. The mean TNF-α concentration, which was zero at baseline, increased beginning 1 h after endotoxin administration, peaked at 1.5 h, and again became undetectable by 4 h. By contrast, the mean concentrations of other pro-inflammatory mediators such as IL-6 (which also has anti-inflammatory effects) and IL-8 peaked at 2 h after endotoxin administration, later than TNF-α. The potent anti-inflammatory mediator IL-10 peaked at 3 h (Fig. 3B–D). These relations point to the temporal primacy of the TNF-α response to endotoxin in this model.
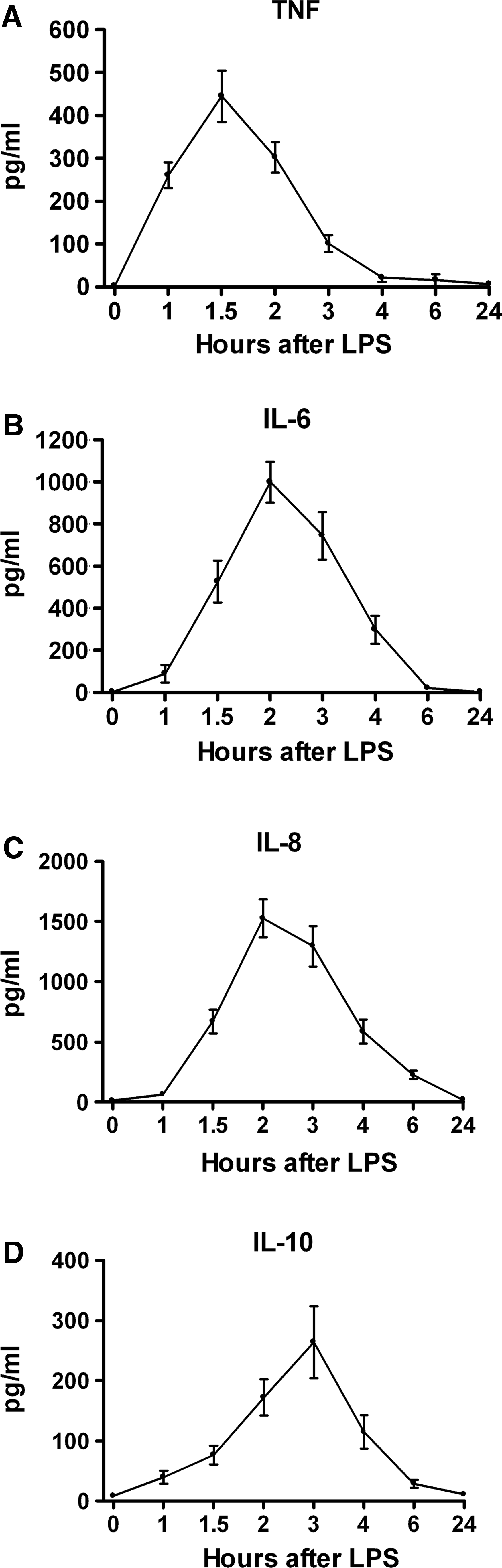
Plasma cytokine responses in normal human volunteers receiving intravenous endotoxin (LPS, 2 ng/kg) at time 0. (
Counter-regulatory hormones
These hormones, including cortisol and epinephrine, have potent and pleiotropic physiological influences (e.g., metabolic, fluid balance, cardiovascular) and additionally have well-established anti-inflammatory effects [16–19]. In Fig. 4A and B, plasma cortisol and epinephrine concentrations are shown. Cortisol concentrations, already at their circadian high point because of the morning (9:00

Plasma counter-regulatory responses in normal human volunteers receiving intravenous endotoxin (LPS, 2 ng/kg) at time 0. (
Leukocyte inflammatory receptors
Blood leukocytes respond to inflammatory stimuli by up-regulating or down-regulating certain receptors that participate in the response to inflammation or infection. Two such receptors are CD11b and TNFR-II. The CD11b moiety is the alpha-M subunit of an integrin named macrophage-1 antigen or complement receptor 3. This integrin is expressed on phagocytic cells (neutrophils and monocytes) and is conformationally up-regulated rapidly and robustly in response to inflammation. The TNFR-II protein is expressed weakly by neutrophils and strongly by monocytes and is down-regulated strikingly in response to inflammation [20].
After IV endotoxin administration to human volunteers, an increase in monocyte mean CD11b expression was detected by 1 h, became maximal at 2–3 h, and returned to baseline by 24 h (Fig. 5A). By contrast, blood monocyte TNFR-II expression declined ∼80% from baseline by 2 h after endotoxin administration, returned to baseline by 6 h, and increased by ∼35% over baseline at the 24-h time point (Fig. 5B).
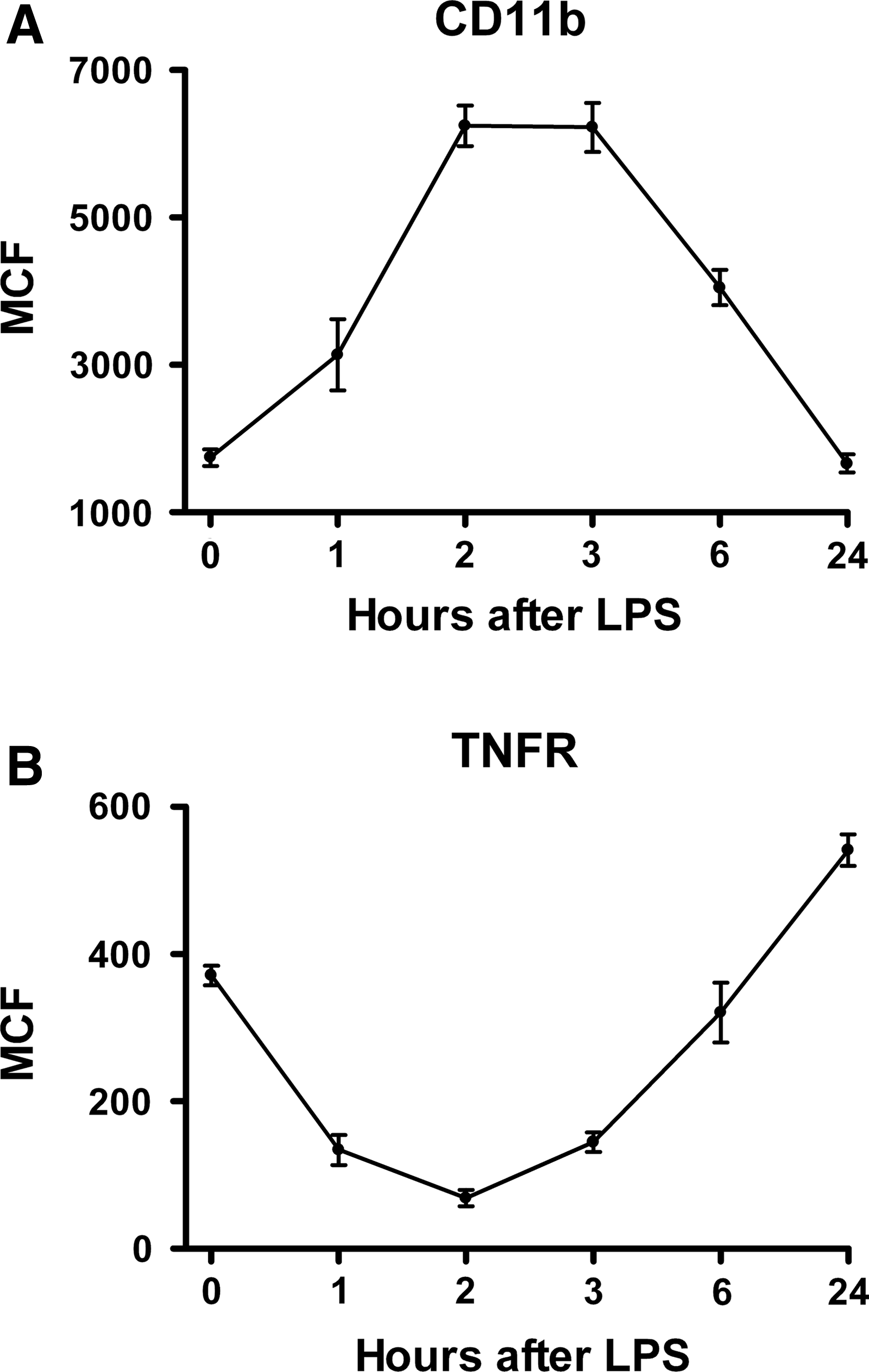
Blood monocyte cell-surface inflammatory receptor responses in normal human volunteers given intravenous endotoxin (LPS, 2 ng/kg) at time 0. (
Discussion
In view of these results, generated using an IV 2 ng/kg endotoxin challenge in normal human volunteers, the responses support this model strongly as one of moderate systemic inflammation in which the SIRS criteria [9,10] are met for core temperature (hyperthermia), heart rate, and WBC count (leukocytosis). The respiratory rate approached but perhaps did not satisfy the SIRS criterion, although, because of the relatively small number of subjects, a Type II error cannot be ruled out. Furthermore, the responses to endotoxin occur in a consistent temporal sequence, although the magnitudes may differ among individuals. Most effects resolve by 6–24 h after endotoxin administration. It should be emphasized firmly that, whereas this model appears to simulate systemic inflammation fairly well, it is not a model of sepsis because no infection is present, and patterns of cytokine responses are different in patients with, and animal models of, sepsis [21]. Because endotoxin is a well-characterized pathogen-associated molecular pattern (PAMP) that signals through Toll-like receptor-4 (TLR4), perhaps the most succinct way to describe this model is as a model of TLR4 agonist-induced systemic inflammation.
A major goal of using the human endotoxin model is to understand the etiologic factors of systemic inflammation so that rational clinical therapies to prevent or attenuate amplified or uncontrolled SIRS could be developed and investigated. Indeed, over approximately the last 25 years, Doctor Lowry and his colleagues employed the human endotoxin model to assess the effects of nutrition (enteral vs. parenteral, low lipid vs. high lipid) [22–25], cytokine antagonists (IL-1 receptor antagonist [RA], TNFR constructs) [26–29], endotoxin antagonists (PEGylated polymyxin B) [30], hormones (cortisol, epinephrine, growth hormone, insulin-like growth factor [IGF]) [16–19,31], and modulators of coagulation (e.g., activated protein C) [32,33]. Many of these compounds and approaches tested in the human endotoxin model have graduated to clinical trials in ICU patients (e.g., low-dose cortisol, IL-1-RA, TNF antagonists). One, activated protein C, was approved by the U.S. Food and Drug Administration for use in sepsis for a decade before the manufacturer withdrew it as ineffective [34–36]. Ironically, although these clinical trials were performed in the context of infection and sepsis, the “cytokine antagonist therapies” did not prove to be efficacious in sepsis [37–39], although several have become mainstream therapies for other inflammatory diseases, including rheumatoid arthritis, inflammatory bowel disease, and gout [40–45].
This paper has focused on the systemic inflammatory aspects of the human endotoxin model. However, a plethora of other physiological responses have been investigated in the model over the years by Doctor Lowry and others. Hormone effects also include modulation of thyroid and growth hormones [29,31,46]. Metabolic and coagulation effects [7,47–51] are prominent, as are cardiovascular and pulmonary effects, including attenuation of heart rate variability [19,52–55]. Finally, gut barrier function is compromised acutely in the model [8], although, curiously, gastrointestinal distress is not reported commonly by volunteers given IV endotoxin.
Footnotes
Acknowledgment
This work was supported by U.S. Public Health Service grant GM034695. We gratefully acknowledge all of the fellows, students, and staff members who have participated in the human endotoxin studies in the Lowry Laboratory over the past 25 years.
Author Disclosure Statement
No competing financial interests exist.