
Abstract

A computed tomography scan of the abdomen (Fig. 1) revealed emphysematous cholecystitis with possible gallbladder perforation. Intravenous metronidazole was added to the empiric antibiotic regimen. The patient developed atrial fibrillation with rapid ventricular response in the emergency department, which required pharmacologic management and admission to the intensive care unit. Due to hemodynamic instability, initial source control was achieved with a percutaneous cholecystostomy, and 40 mL of brown foul-smelling drainage was aspirated from the gallbladder. Empiric antibiotics were changed to meropenem and vancomycin. Blood and bile cultures were positive for two isolates of Clostridium perfringens and bile culture also was positive for Enterococcus faecium (sensitive to ampicillin and vancomycin).

Computed tomography of emphysematous cholecystitis (arrow). Circumferential mural emphysema involving the gallbladder, which contains multiple gallstones. There is extension of inflammation into the adjacent liver with a small oblong fluid collection measuring 19×8 mm reflecting an intrahepatic abscess. Inflammation containing gas measuring 3×2 cm between the gallbladder and liver may reflect a site of perforation. There are a few locules of extraluminal gas seen within the right upper quadrant. Inflammation extends along the right paracolic gutter and medially to the pancreas.
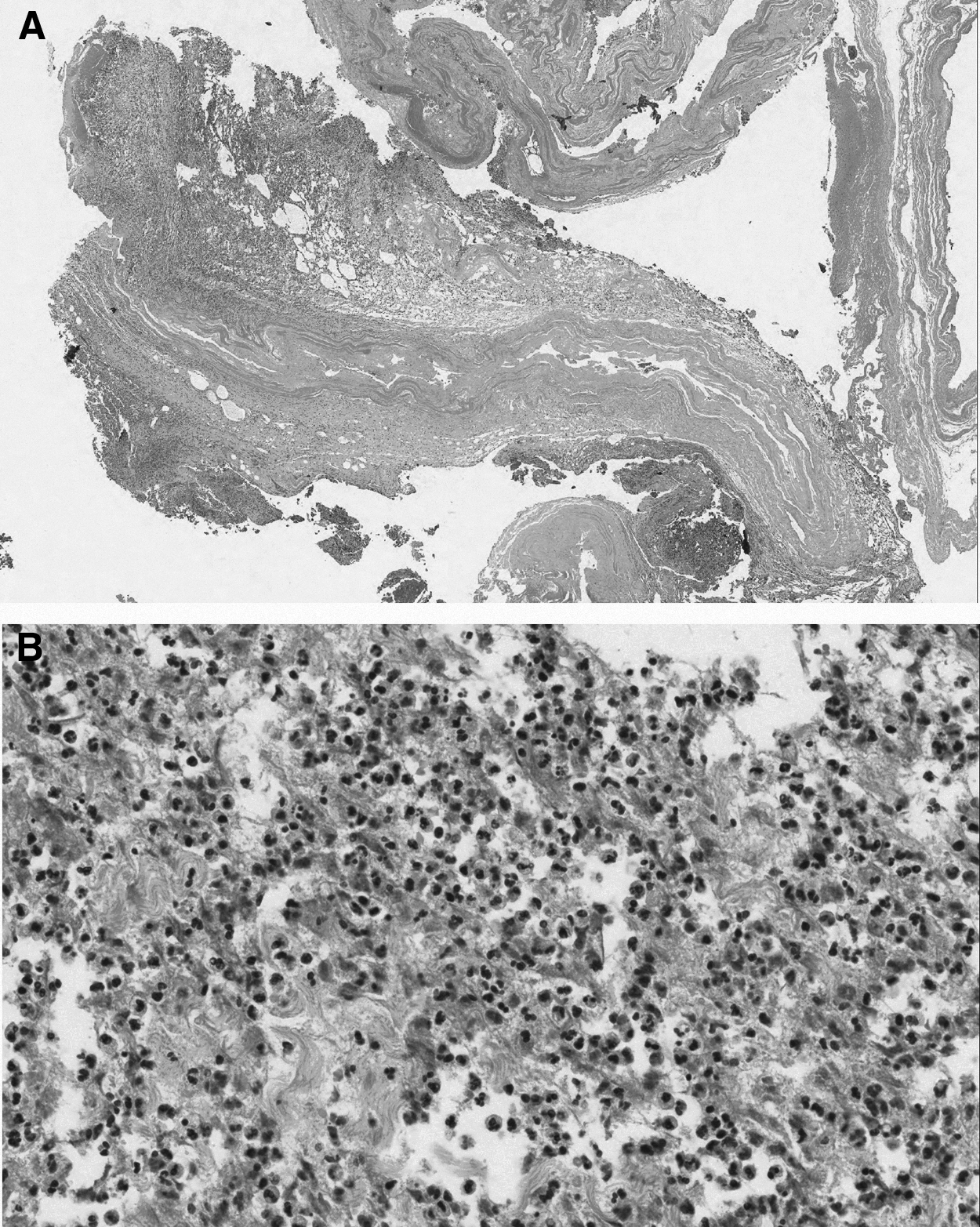
The patient failed to improve, exhibiting persistent abdominal pain and leukocytosis, and open cholecystectomy was required for definitive source control. At surgery, the omentum encased the gallbladder containing the perforation, and dense inflammatory adhesions to the colon and duodenum required adhesiolysis. Pathology of the surgical specimen (Fig. 2) revealed histologic evidence of acute gangrenous cholecystitis with cholelithiasis and a transmural scar indicating previous ulcerating disease. She was discharged home on post-operative day 4 with an oral course of metronidazole (500 mg PO QID×7 d) to complete two weeks of antimicrobial therapy for C. perfringens bacteremia. It was confirmed on subsequent clinic visits that she recovered fully with no recurrence of abdominal infection.
Emphysematous cholecystitis is characterized by the presence of gas within the wall or lumen of the gallbladder in the absence of an abnormal biliary-enteric communication. The pathophysiology is an acute infection caused by gas-producing organisms with local ischemia. It was first described by Stolz in 1901 in three patients at post-mortem examination [1]. The first pre-operative diagnosis was made by C.F. Hegner in 1931 with abdominal radiographs in a 62-year-old male who underwent cholecystectomy but died of a pulmonary embolus on the fourth post-operative day [2].
Although the condition is relatively rare, it is of great importance to surgeons as the reported mortality rate is high (15%–20%) [3] and the standard treatment is emergency cholecystectomy, with percutaneous drainage reserved for patients not stable for surgical intervention [4–6]. Early diagnosis is necessary. However, it is difficult to differentiate typical acute cholecystitis from emphysematous cholecystitis based on clinical presentation; radiologic imaging (abdominal radiograph, ultrasound, computed tomography) is required. Early surgical intervention may precede development of gangrenous cholecystitis and perforation, thereby greatly reducing mortality in this population [7].
Unlike acute cholecystitis, which is more frequent in females, emphysematous cholecystitis is more frequent in males (male-female ratio, 4:1), many of whom have diabetes mellitus [8]. The causative pathogens in emphysematous cholecystitis are gas-producing bacteria (e.g., C. perfringens, Escherichia coli, Klebsiella spp.) with a high rate of concomitant bacteremia. Early initiation of empiric broad-spectrum empiric antibiotics to cover these pathogens is required for successful outcome. Bile and blood cultures are necessary to provide pathogen-directed antimicrobial therapy. The recommended duration of antimicrobial therapy is longer (two weeks recommended) if bacteremia is present.