
Abstract
Abstract
Background:
Laparoscopic cholecystectomy (LC) is the procedure of choice for treatment of cholelithiasis/cholecystitis. Conversion rates (CR) to open cholecystectomy (OC) have been reported previously as 5–15% in elective cases, and up to 25% in patients with acute cholecystitis. We examined the CR in a tertiary-care academic hospital and a statewide surgery quality collaborative, and to compare complications and outcomes in elective and emergency cholecystectomy.
Methods:
Prospective data were obtained from: 1) Non-Trauma Emergency Surgery (NTE) database of all emergent cholecystectomies 1/1/2008-12/31/2009; and 2) Michigan Surgical Quality Collaborative (MSQC) database with a random sample of 20–30% of all operations performed 1/1/2005–12/31/2010, including both University of Michigan (UM) data and statewide data from 34 participating hospitals. Patient characteristics, CR, and outcomes were compared for emergent vs. elective cases.
Results:
Non-trauma ES patients had a mean hospital length of stay (HLOS) of 4.9 d. Open cholecystectomy-HLOS was greater (4.0, LC; 7.9 laparoscopic converted to open cholecystectomy; 8.7, OC, p<0.0001); mortality was 0.35% and CR was 17.5%. In the UM-MSQC dataset, OC-HLOS was greater (6.8 OC vs. 4.6 LC, p<0.001); mortality was 0.65%; CR was 9.1% in elective cases and 14.9% in emergent cases. CR was almost two-fold higher [17.5% of all NTE cholecystectomies vs. 9.1% of UM-MSQC elective cholecystectomies (p=0.00078)]. The statewide MSQC cholecystectomy data showed significantly increased HLOS in emergent cholecystectomy patients (4.34 vs. 2.65 d; p<0.0001). Morbidity (8.8 vs. 3.7%) and mortality (2.6 vs. 0.5%) rates were also significantly higher in emergent vs. elective cholecystectomies (p<0.0001).
Conclusion:
In NTE patients requiring cholecystectomy, CR is almost two-fold higher but is lower than in reports published previously (25%). However, there is a wide variability in mortality and morbidity for emergency cholecystectomy in both unadjusted and risk-adjusted analyses. Further studies are required to determine modifiable risk factors to improve outcomes in emergency cholecystectomy.
W
Although acute gallbladder pathology (e.g. acute cholecystitis, gallstone pancreatitis) and open cholecystectomy (OC) are associated with adverse post-operative outcomes [6], recent data are sparse regarding CR and outcomes in patients requiring emergency surgery. The objective of this study was to examine CRs and outcomes in patients requiring emergent vs. elective cholecystectomy. We hypothesized that patients who required emergent cholecystectomy would have a higher laparoscopic-to-open cholecystectomy CR, associated with increased hospital LOS, morbidity, and mortality, compared with elective cholecystectomy patients.
Patients and Methods
Data for this study were obtained from two sources: 1) the Non-Trauma Emergency (NTE) database at the University of Michigan; and 2) the Michigan Surgical Quality Collaborative (MSQC) database for the state of Michigan.
Non-Trauma Emergency (NTE) database
In July 2005, a NTE surgery service was created at the University of Michigan to be primarily responsible for evaluation and disposition of all urgent and emergent inpatient general surgery consults and emergency department general surgical consults, with admission to the NTE surgery service when appropriate. Data for the NTE database were collected prospectively by a dedicated trauma registrar and intensive care unit (ICU) coordinator daily. Overall case mix and patient characteristics have been reported previously [7]. From this database, we identified patients who had undergone LC or OC between January 1, 2008, and December 31, 2009, and reviewed retrospectively this subset of patients. Patient demographics (age, gender, and race), hospital LOS, and mortality data were extracted from the database. Morbidity data were not available in this database. Patient medical registration numbers were used as a cross-reference to obtain operating room (OR) times from the OR systems database; times reported reflect the total patient room time in the OR. Operative reports were reviewed manually by the authors to verify the procedure performed, and also to screen for conversion to an open procedure and reason for the conversion.
Michigan Surgical Quality Collaborative database
The Michigan Surgical Quality Collaborative database (MSQC) is a statewide surgical quality collaborative based on the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) that was created as a partnership among the ACS, 34 participating Michigan hospitals, and Blue Cross and Blue Shield of Michigan/The Blue Care Network, which funds the effort fully, with the goals of establishing an infrastructure for data collection, collaboration, and ad hoc quality improvement efforts within the state [8]. This collaborative is one of several to have demonstrated the effectiveness of regional collaboratives in improving the quality of surgical care [9]. Within the MSQC, there has been an absolute morbidity reduction in elective general and vascular surgery operations of 9.0% [10]. The MSQC has now initiated a focus on quality improvement in emergency general surgery in the state of Michigan.
The MSQC data are collected prospectively by a dedicated Surgical Clinical Nurse Reviewer who reviews operative and anesthesiology notes to stratify cases as emergent or elective, as defined by the ACS-NSQIP. Urgent cases are included in the elective cohort. Approximately 20–30% of all cases performed are entered into the MSQC database, with a robust range of clinical patient data points. Data collected include: Patient demographics, operation performed as defined by Current Procedural Terminology (CPT) codes (Table 1), operative times, preoperative and postoperative laboratory values, comorbid conditions, discharge/disposition information, American Society of Anesthesiologists classification, wound classification, mortality, and morbidity (morbidity parameters listed in Table 2) [11,12]. From January 1, 2005, to December 31, 2010, the MSQC database was queried to extract cholecystectomy data by CPT codes. Cases were identified a priori as emergent or elective at time of data entry. The hospital LOS, 30-d post-operative morbidity, and mortality were assessed. Morbidity was defined as at least one case of the following: acute kidney injury, bleeding leading to transfusion, cardiac arrest, neurologic event (cerebrovascular accident [CVA], coma lasting more than 24 h, or peripheral nerve injury), surgical site infection (superficial, deep, or organ space), deep venous thrombosis, prosthetic graft failure, myocardial infarction, renal insufficiency, pulmonary embolism, stroke, sepsis, septic shock, unplanned intubation, wound disruption, and ventilator dependence for more than 48 h. Urinary tract infection was excluded as a morbidity outcome for the analysis.
CNS=central nervous system; CPR=cardiopulmonary resuscitation; CVA=cerebro-vascular accident; SIRS=systematic inflammatory response syndrome; SSI=surgical site infection.
Statistical Analysis
Descriptive statistics were computed for the study cohort. Continuous variables were summarized by the mean and standard deviation, whereas categorical variables were summarized with frequency tables. Continuous variables were compared using Student's t-test, while chi square and Fisher exact tests were used to compare categorical and dichotomous variables, respectively, with a p value of 0.05 considered significant. Relationships between the proportion of emergent surgery and morbidity or mortality were assessed using linear regression techniques. Logistic regression analysis was used to identify factors associated independently with morbidity and mortality to provide risk-adjusted morbidity and mortality outcome data. A morbid outcome was defined as the incidence of any of the outcomes previously listed. The 42 covariates available in the MSQC included: Age, alcoholism, angina, ascites, race, bleeding diathesis, body mass index, cancer, chemotherapy, congestive heart failure, central nervous system deficit, chronic obstructive pulmonary disease, cerebrovascular accident (CVA) resulting in residual neurological deficit, CVA resulting in no neurological deficit, diabetes mellitus, dialysis, dyspnea, esophageal varices, gangrene, gender, hemiplegia, hypertension, impaired sensorium, open wound, paraparesis, percutaneous transluminal coronary angioplasty, pre-operative myocardial infarction, preoperative sepsis, pre-operative functional status, previous cardiac surgery, peripheral vascular disease, quadriparesis, radiotherapy, renal insufficiency, smoking, steroid use, transient ischemic attack, total operation time, transfer from home, transfusion, unintended weight loss, and ventilator dependence. All candidate predictors were entered into the model, and stepwise backwards selection was used to select a subset of adjustment covariates. The c-statistic was used to gauge the model's predictive accuracy.
The output from the logistic regression analysis was used to derive the adjusted morbidity and mortality ratios. These were calculated by dividing the predicted number of morbidity or mortality cases (sum of predicted frequencies per site) by the total number of observed cases per site. The 95% confidence intervals for these rates were calculated in an identical fashion, by dividing the upper and lower estimates by total cases per site. A two-sided significance level of α=0.001 was used in all analyses. All statistical computations were performed in SAS v9.2 (SAS Institute; Cary, NC).
Results
Non-trauma Emergency Surgery Data
Between January 2008 and December 2009, there were 1708 NTE admissions, and 1202 patients required surgical intervention. Cholecystectomy was performed in 279 (23%) patients: 217 (77.8%) were laparoscopic (LC), 16 (5.7%) were open (OC), and 46 (16.5% of all NTE patients, 17.5% of all laparoscopic attempts) were laparoscopic converted to open cholecystectomy (CONV; Table 3). Overall, female gender was more common (34.4% male, 65.6% female). Mean age was 45.4 y (range 18–91). Operative times were significantly less in laparoscopic cases; however, the range in OR times was similar. HLOS was significantly greater in patients undergoing open cholecystectomy (mean HLOS 4.9 days overall, 4.0 LC, 7.9 CONV, 8.7 OC; p<0.0001 LC vs. OC and p=0.0036 in LC vs. CONV). Overall hospital mortality was 0.35%; the incidence of death was too small to detect any significant differences identified amongst the three cohorts.
CONV was 16.5% of all NTE cholecystectomies; conversion rate was calculated as CONV/(LC+CONV)=17.5% of all laparoscopic attempts.
Operative times were significantly less in laparoscopic cholecystectomy: LC vs. OC (p<0.0001); LC vs. CONV (p=0.0036).
HLOS significantly greater in open cholecystectomies: LC vs. OC (p<0.001); LC vs. CONV (p<0.0001).
CONV=laparoscopic surgery cases converted to open cholecystectomy; HLOS=hospital length of stay; LC=laparoscopic cholecystectomy; NTE=non-trauma emergency; OC=open cholecystectomy.
Michigan Surgical Quality Collaborative Data
Statewide MSQC Data
From January 2005 to December 2010, 190,826 operations were entered into the MSQC database. Cholecystectomies accounted for 18,106 cases (9.52% of total cases; Table 4), with 16,697 (92.22%) elective and 1,409 (7.78%) emergent cases. Laparoscopic cholecystectomy was performed in 90.9% of elective cases vs. 78.7% of emergent cases. Hospital LOS was significantly increased in emergent cholecystectomy patients (4.34 vs. 2.65 d). Morbidity (8.8 vs. 3.7%) and mortality (2.6 vs. 0.5%) rates were also significantly higher in emergent vs. elective cases (p<0.0001).
p<0.0001 for HLOS, morbidity and mortality in statewide MSQC elective vs. emergent cholecystectomy patients.
CONV=laparoscopic surgery cases converted to open cholecystectomy; HLOS=hospital length of stay; LC=laparoscopic cholecystectomy; MSQC=michigan state quality collaborative.
Unadjusted and risk-adjusted mortality (Figs. 1 and 2) and morbidity (Figs. 3 and 4) data were examined for the statewide MSQC data for all emergent cholecystectomy patients. In the unadjusted analysis, OC was associated with higher mortality and morbidity rates, but significant site-dependent variability was noted among the 34 hospitals.
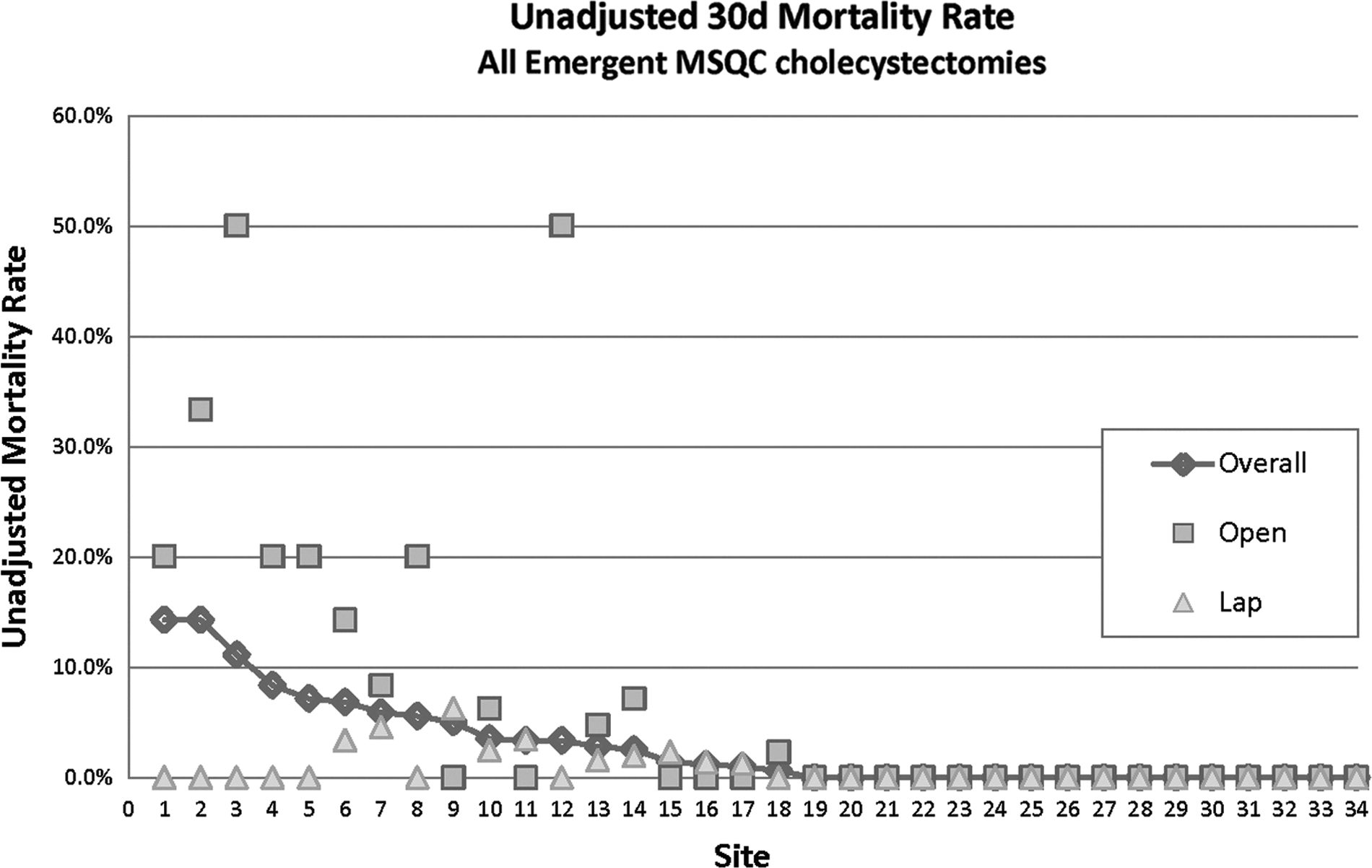
Unadjusted 30-d mortality rate among all emergent Michigan Surgical Quality Collaborative database cholecystectomies performed between 2006–2010.

Risk-adjusted 30-d mortality rate among all emergent Michigan Surgical Quality Collaborative database cholecystectomies performed between 2006–2010. Adjustment covariates: pre-operative sepsis, age, pre-operative functional status, pre-operative ventilator, pre-operative ascites.

Unadjusted 30-d morbidity rate among all emergent Michigan Surgical Quality Collaborative database cholecystectomies performed between 2006–2010.

Risk-adjusted 30-d morbidity rate among all emergent Michigan Surgical Quality Collaborative database cholecystectomies performed between 2006–2010. Adjustment covariates: Laparoscopic approach, total operating room time, pre-operative sepsis, age, pre-operative functional status, pre-operative pneumonia, pre-operative ascites, pre-operative sensorium, pre-operative cerebral vascular accident resulting in neurologic deficit.
In the risk-adjusted analysis of emergent (Fig. 2 and Fig. 4) and elective cholecystectomy patients (Fig. 5 and Fig. 6), independent variables that impacted outcomes were adjusted to assess further the differences in mortality and morbidity. For mortality risk adjustment, adjustment covariates included pre-operative sepsis, age, pre-operative functional status, pre-operative ventilator, and pre-operative ascites. For morbidity risk adjustment, adjustment covariates included laparoscopic approach, total OR time, pre-operative sepsis, age, pre-operative functional status, pre-operative pneumonia, pre-operative ascites, pre-operative sensorium, and pre-operative CVA resulting in neurologic deficit. These risk-adjusted data validate the unadjusted data and confirm significant site-dependent mortality rates (ranging from 0.1 to 10.0%) and morbidity rates (ranging from 0.1 to 25%). Furthermore, there is an overall increase in mortality and morbidity in patients who had emergency status or underwent OC.

Risk-adjusted 30-d mortality rate among all elective Michigan Surgical Quality Collaborative database cholecystectomies performed between 2006–2010. Adjustment covariates: Pre-operative sepsis, age, pre-operative functional status, pre-operative ventilator, pre-operative ascites.
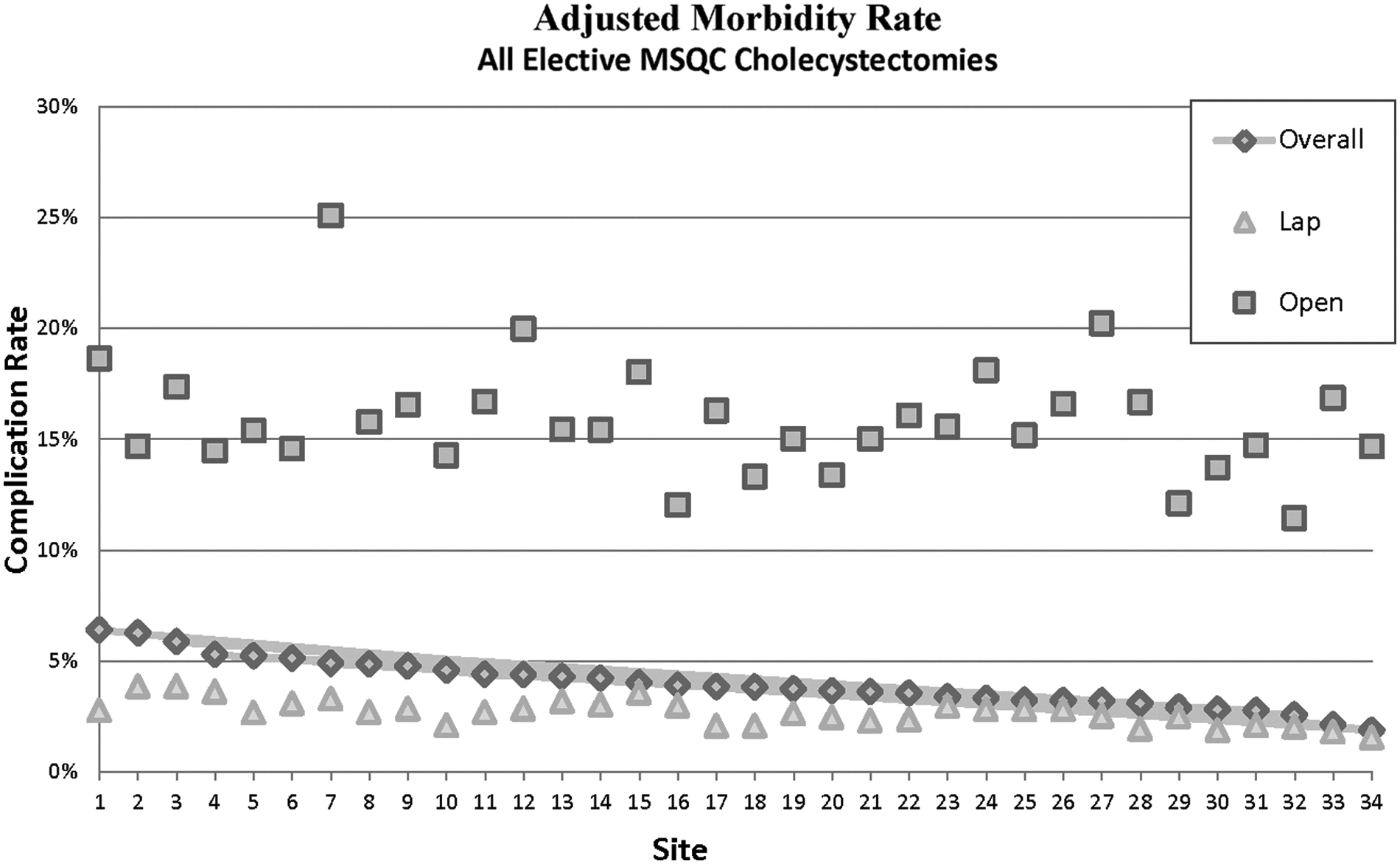
Risk-adjusted 30-d morbidity rate among all elective Michigan Surgical Quality Collaborative database cholecystectomies performed between 2006–2010. Adjustment covariates: Laparoscopic approach, total operating room time, pre-operative sepsis, age, pre-operative functional status, pre-operative pneumonia, pre-operative ascites pre-operative sensorium, pre-operative cerebral vascular accident resulting in neurologic deficit.
University of Michigan MSQC Data
The University of Michigan MSQC data included 10,960 operations, of which 773 (7.05%) were cholecystectomies. One case was dropped due to CPT/charting discrepancy. Of the remaining 772 cases, 672 were classified as elective and 100 as emergent cases (Table 4 and Table 5). Cholecystectomy patients were 67.4% female, with a mean age of 47.5 y (range 18–94). Laparoscopic cholecystectomy was performed in 82.8% of elective cases vs. 80% of emergent cases, similar to the statewide MSQC data. Hospital LOS (5.44 vs. 3.73 d), morbidity (10.0 vs. 4.9%), and mortality (1.0 vs. 0.6%) rates were all higher in emergent cases.
p<0.0001 for laparoscopic vs. open cholecystectomies. p=0.055 for elective vs. emergent cases.
HLOS=hospital length of stay; LC=laparoscopic cholecystectomy; OC=open cholecystectomy.
We next compared LC vs. OC outcomes (Table 5). Hospital LOS was greater for the OC group (6.8 OC vs 4.6 LC, p=0.006). Overall hospital mortality was 0.65% (0.6% elective, 1% emergent). Conversion rate from LC to OC was higher in the emergent cases (14.9% in emergent cases vs. 9.1% in elective cases; p=0.053). Operative time was also higher in the emergent group vs. the elective group (p=0.055) and in OC vs. LC (p<0.0001). Post-operative complications occurred in 56 (7.3%) of 772 elective cholecystectomy patients, with superficial incisional (SSI) being the most common post-operative complication reported (Table 6).
CPR=cardiopulmonary resuscitation; DVT=deep venous thrombosis; SSI=surgical site infection.
Comparison of NTE and University of Michigan MSQC data
Conversion rates (LC to OC) were similar for NTE emergency patients (17.5%) and University of Michigan MSQC emergency patients (14.9%), and significantly higher than the CR in elective patients (9.1%; p=0.00078; Table 7).
Conversion rate was calculated as a ratio of converted cases to all laparoscopic attempts: CONV/(LC+CONV). Conversion rates were statistically significant for emergent vs. elective cases: 1) NTE vs. elective MSQC cases (p=0.00078); 2) MSQC elective vs. MSQC emergent cases (p=0.0941); 3) no statistically significant difference for NTE vs. MSQC emergent cases (p=0.63).
Operative times were defined as total patient time in room for the NTE database; for the MSQC database operative times were defined as surgical incision to close: 1) NTE vs. elective MSQC cases (p<0.0001); 2) MSQC elective vs. MSQC emergent cases (p=0.055); 3) NTE vs. MSQC emergent cases (p=0.036).
NTE=Non-Trauma Emergency Surgery database; MSQC=Michigan Surgical Quality Collaborative; CONV=laparoscopic surgery cases converted to open cholecystectomy; LC=laparoscopic cholecystectomy.
Operative duration was also significantly increased for NTE vs. MSQC elective cholecystectomy cases (p<0.0001). No differences in age or gender were identified between these groups.
Discussion
Cholecystectomy is one of the most common operations performed on emergency surgical services. We described previously that cholecystectomy comprised 24% of all surgical cases on the NTE service at the University of Michigan. In this current study, we examined CR (LC to OC) and outcome in elective vs. emergent cholecystectomy patients at our institution and in the state of Michigan. Evaluation of outcomes in emergency surgery is an important initiative, because it provides the foundation of data for performance improvement in this group of patients. Previous performance improvement efforts have focused only on elective general surgery, but recent data confirm that a far greater proportion of morbidity and mortality occurs in emergency general surgery patients, providing support for more in-depth analyses of our emergency general surgery cases [5,13].
In this study, we reviewed cholecystectomy data from two different perspectives and two different databases available at the University of Michigan. The NTE database captured all patients admitted or seen in consultation for acute gallbladder pathology (most commonly acute cholecystitis or gallstone pancreatitis) who underwent cholecystectomy subsequently. By comparison, we examined University of Michigan institutional data from the MSQC database, which includes a random sampling that captures both outpatient elective cholecystectomies for symptomatic cholelithiasis, as well as patients undergoing emergency cholecystectomy. These data confirmed that CRs for the emergent cases were higher than the elective cases but surprisingly there was no significant difference in morbidity or mortality in cases performed at the University of Michigan.
The University of Michigan institutional data also confirmed lower morbidity and mortality rates than previously reported. In their review of the ACS-NSQIP data for emergency cholecystectomies performed from 2005–2008, Ingraham et al. reported overall morbidity and mortality rates of 8.64% and 1.80% respectively [5]. By comparison, our overall morbidity and mortality rates for the University of Michigan MSQC database were 5% and 1% for emergent cholecystectomies, with even lower rates in the elective cholecystectomy group. Morbidity data were not available for the NTE database, but mortality was 0.35% in this specific emergency cholecystectomy cohort.
In contrast to our University of Michigan institutional data (NTE and MSQC data), the statewide MSQC data confirmed that morbidity (8.8 vs. 3.7%) and mortality (2.6 vs. 0.5%) rates were significantly higher in emergent vs. elective cases. Risk-adjusted mortality/morbidity data also confirmed wide variability and significant differences in site-dependent mortality rates (ranging from 0.1 to 10.0%) and morbidity rates (ranging from 0.1 to 25%) in all emergency cholecystectomy cases.
There are several limitations to our study. All data for both the NTE and the MSQC database were collected prospectively, but analyzed retrospectively. The MSQC database did not include all cholecystectomy cases, either at the University of Michigan or statewide, thus selection bias is a possible confounding variable. In the case of the NTE database, operations were identified via the electronic medical record. It is possible that not all cholecystectomies performed were captured and the total number of cases may be under-represented.
Additionally, although the service is designed to care for urgent and emergent general surgical patients, on occasion outpatient cases may be scheduled into the NTE service time. There is no a priori definition in the NTE database for what constituted elective, urgent, or emergent surgical intervention. Additionally, one-half of the NTE faculty also cover the Trauma, Burn, and Emergency Surgery (TBE) service, and it is possible that some cases performed by the TBE service and therefore not captured properly into the NTE database. Operative times in the NTE database were extracted from the operating room system records retrospectively, and reflect total room time rather than actual surgery start-to-end time. Thus, the operating room times may be an over-estimate of the actual length of surgery. The University of Michigan MSQC data is a much broader sampling of all cases performed at the University Hospital, both on the elective general surgery services as well as the NTE and TBE services. The method for data entry is to capture all cases during a portion of each month, with a cap for the types of cases captured per month. The premise is to establish a random sampling of the total case load, but theoretically could result in sampling error. Some of the patient cases included in the University of Michigan MSQC database also overlap with the NTE database, but whereas the NTE data include all cholecystectomies from the NTE service, the University of Michigan MSQC database only has a partial inclusion of the NTE emergent cases.
In conclusion, although patients requiring emergent cholecystectomy have an almost two- fold higher risk CR (17.5% NTE vs. 9.1% elective MSQC), this is lower than in previous published reports (25%) and supports the initial attempt at laparoscopy even in the emergent setting. Further, whereas emergency cholecystectomy is associated with longer operative times and hospital LOS, there was no difference in mortality identified in our NTE and MSQC institutional data. In contrast, statewide MSQC data confirm wide site-specific variability in risk-adjusted outcomes (30-d mortality and morbidity) for emergency cholecystectomy, and additional in-depth analyses are underway to determine the factors associated with high-outlier vs. low-outlier hospitals. Data from these analyses will be able to be used to initiate performance improvement efforts in emergency cholecystectomy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.