
Abstract
Abstract
Background:
Owing to a lack of current understanding of outcomes and costs by type of hysterectomy procedure, we attempt to quantify the incidence and impact of surgical site infection (SSI) in laparoscopic and non-laparoscopic approaches to abdominal and vaginal hysterectomy.
Methods:
Patients whose data were contained in the Premier Perspectives Database of 600 hospitals in the United States were selected on the basis of a post-operative diagnosis of SSI and treatment with antibiotics. The incidence of SSI and associated hospital length of stay (LOS) and costs were estimated. The effect of SSI on readmission was also analyzed.
Results:
Of 210,916 hysterectomies included in the study, 55% were open abdominal procedures. Although the overall incidence of SSI in hysterectomy was low, its incidence was greater in open abdominal hysterectomy than in other approaches to hysterectomy. Patients with an SSI experienced a three- to five-fold greater LOS, two-fold greater cost, and three-fold greater risk of hospital readmission than those without an SSI.
Conclusions:
This study provides clinical evidence in support of less invasive approaches to hysterectomy. In addition to other documented benefits of such less invasive procedures, the lower incidence of SSIs and lower rates of associated complications and costs with these procedures than with open abdominal hysterectomy should be taken into account when weighing the risks and benefits of a surgical approach for patients whose condition warrants hysterectomy.
A
Clinical evidence supports the notion that less invasive vaginal or laparoscopic hysterectomies are associated with fewer complications, shorter hospitalizations, and a more rapid return of patients to normal activities than is open abdominal hysterectomy [4,5]. The American College of Obstetrics and Gynecology (ACOG) Committee on Gynecologic Practice has reached a similar conclusion. Among the established benefits of a less invasive approach to hysterectomy is the lower incidence of associated wound or abdominal infections than with open abdominal hysterectomy [6].
However, despite the evidence, practice guidelines, and seemingly obvious benefits of less invasive procedures for hysterectomy with regard to clinical, economic, and humanistic outcomes, only one in three hysterectomies are currently performed with such procedures [2]. An analysis of surgical data for the United States shows that abdominal hysterectomy is performed in 66% of cases, vaginal hysterectomy in 22%, and laparoscopic hysterectomy in 12% [7]. It is therefore important to continue to further strengthen the body of evidence for less invasive hysterectomy procedures.
Surgical site infections (SSIs), if they occur, can largely determine the rapidity and ease of recovery after hysterectomy. Although fever in the first 24 h post-operatively may largely be explained by the release of inflammatory cytokines associated with incision, reports have shown that fever caused by abscess and cellulitis from SSI and occurring a few days following gynecologic surgery is not uncommon [8]. Patients undergoing abdominal hysterectomy are more likely to experience febrile morbidity than those who undergo vaginal hysterectomy [9].
Some studies have reported statistically significantly lower overall risks of SSI [10] and nosocomial infection [11], as well as fewer readmissions because of such infection, in association with laparoscopic as compared with open cholecystectomy. However, no studies of the risk of SSI following hysterectomy were found at the time of writing of the present paper.
This issue of SSIs assumes greater importance in light of a recent ruling by the U.S. Centers for Medicare and Medicaid (CMS), which, under the Health Care Reform Act of 2010, includes proposed changes to the regulations governing hospital-acquired conditions (HACs) that in some states, such as Tennessee, require hospitals to report SSIs following hysterectomy procedures as a condition for reimbursement [12]. However, even for other states, monitoring for SSI following hysterectomy procedures, and developing processes to reduce its risk, will become increasingly important. Readmissions associated with SSIs could also offer an efficient measure of the quality of health care provision and the related financial effect on hospitals.
Our study was designed to address the need for a practical assessment of the outcomes of various techniques of hysterectomy, particularly with respect to the risk of SSI, and the costs of these outcomes. This study is the first to quantify the incidence as well as the clinical and economic impact of SSIs in open abdominal hysterectomy as compared with less invasive vaginal and laparoscopic approaches to hysterectomy in the United States through analysis of a large, retrospective inpatient hospital data base.
Patients and Methods
Patient selection
Patients included in the study were drawn from the Premier Perspectives Database (www.premierinc.com; Charlotte, NC), a national administrative data base containing hospital billing data for about 600 hospitals throughout the United States. The study covered the period from January 2007 to December 2009, and therefore captured information about recent clinical practice. Because the study used de-identified hospital claims data, it did not require approval by an institutional review board.
Patients were identified through International Classification of Diseases, Ninth Revision, Clinical Modification (ICD9-CM) and procedural codes for hysterectomy (Table 1). Several exclusion criteria were applied to further select a relevant patient group of interest, with further refinement of this through the exclusion of erroneous records (outliers) showing unrealistic utilization of resources and by reducing the number of confounding cases. These latter cases included those of patients ≤18 y of age at the time of surgery; male patients with obstetric and gynecologic procedure codes (abdominal hysterectomy; vaginal hysterectomy; obstetric delivery by cesarean section); and cases with SSI as the admitting and/or primary diagnosis; with a hospital length of stay (LOS) >150 d; with daily charges≤$1,000; with an operating room time>48 h; with unrelated multiple procedures; and with multiple primary-category-procedures on the same day; and cases of patients with post-operative infections other than SSI (pneumonia patients [480.xx-484.xx] and of patients with catheter-related blood stream infections [CRBSIs; 999.31], urinary tract infections [UTId], [599.0], meningitis [320.0], sinusitis [461.0], endocarditis [424.9], cholecystitis [575.0], and pseudomembranous colitis [008.45]).
In accord with the observational nature of the study and the usual approach to analyses of large administrative data bases, and in view of the high volumes of surgical procedures available for inclusion in the study, a calculation of sample size done through statistical power analysis was deemed unnecessary.
In the study, SSI was defined as an infection occurring after surgery in the part of the body in which the surgery took place. To identify cases of SSI, records selected as candidates for the study were examined subsequently for evidence of SSI through a combination of ICD-9-CM codes (998.5x) for post-operative infection or on the basis of a postoperative prescription of selected antimicrobial drugs begun at least 2 d after the date of surgery and continued for 5 d or more. This algorithm for defining SSIs in large administrative data sets had been found effective previously in distinguishing the more common prophylactic use of antibiotics from antibiotic therapy [13–15].
The following ICD-9-CM codes were used as markers for SSI when that latter was listed as a secondary discharge diagnosis: 998.59 (other postoperative infection), 998.51 (infected postoperative seroma), and 998.5 (postoperative infection not elsewhere classified). Even though ICD-9-CM 998.59 and 998.51 are the only two codes included in the 998.5 category, code 998.5 was included in the list of identifiers because the full two decimal points in the latter code were not always documented; about 10% of presumptive cases of SSI were coded as 998.5.
The types of antibiotics typically used to treat SSIs, obtained from the pharmacy charges recorded on a daily basis in the Premier data base, were used for identifying SSIs as part of the patient-selection algorithm. Patients identified through the above selection process were then grouped into the four categories of abdominal (laparoscopic and non-laparoscopic) and vaginal (laparoscopic and non-laparoscopic) hysterectomy through use of the coding shown in Table 1 for type of surgery.
Outcome measures
The outcome measures in the study included incidence of SSI baccording to type of hysterectomy and operative approach. Length of hospital stay as a proxy for use of hospital resources, and costs of hospital admission, were the two main outcomes used to describe the incremental burden of SSIs above the usual rates of utilization of services and costs of hysterectomy. Length of hospital stay and the cost associated with a specific procedure for patients with and those without SSIs were compared within each category of type of hysterectomy and surgical approach. All-cause readmissions within a month following the index hysterectomy procedure were also examined, to assess the potential effect of SSI on the incidence, LOS, and costs of such readmissions.
Statistical analyses
Descriptive statistics were generated for each type of surgical procedure used for hysterectomy. Reported measures include the number of observations, means, and standard deviations for continuous variables, and frequencies (proportions) for categorical variables. The study population in the Premier Perspectives Database was described by demographic characteristics at the time of each patient's primary procedure, including age, gender, race, geographic location, marital status, primary payer, and the severity of illness (all patient refined [APR]-severity) classification in the All Patient Refined Diagnosis Related Groups (APR-DRGs) system (3M Health Information Systems, Wallingford, CT).
APR_severity is defined as the extent of physiologic decompensation or organ system loss of function, and is divided into four subclasses numbered sequentially from one to four and indicating, respectively, minor, moderate, major, and extreme severity of illness [16]. The clinical principle behind this measure of severity is that it is dependent on the patient's underlying clinical problems, and that patients with a high severity of illness are usually characterized by multiple serious diseases or illnesses. The assessment of the severity of illness based on the patient's complicating or co-morbid conditions is therefore disease-specific. Patients with a high APR-severity are generally expected to have poor outcomes and to incur greater than average health care cost. Accordingly, the APR-severity measure is appropriate for analyses of hospital resource use.
Least-mean-square statistical tests were conducted for between-group comparisons of the continuous variables in the study, and were adjusted for errors in multiple comparisons through the Tukey–Kramer method. The distributions of proportions of count variables between groups were compared through χ2 tests adjusted for multiple comparisons by Bonferroni corrections.
Certain features of health care cost and utilization data, such as their typically highly skewed distribution, makes it difficult to use ordinary regression analyses to analyze such data for reliable interpretation. In particular, a relatively small proportion of patients may experience very high costs and long LOS, which can bias the mean for the patient population as a whole. Such cases are more appropriately addressed by the generalized linear model having a log-link function fitted to the gamma distribution [17]. Models of this type provide robust estimators in the presence of non-normal data that show significant skewing. In addition, such models can be applied in a multi-varible setting to include covariates to account for differences that may occur in claims-based, non-experimental data, such as those for the comparison groups in the present study. Covariates in the data analysis in the present study included patient-level surgical risk factors (age, race, marital status, APR-severity score) and hospital characteristics (hospital size, teaching or non-teaching function, geographic location [national region and local urban/rural], and type of payer). Means, standard errors, and 95% confidence intervals were reported.
On the basis of the structure of the database, all patients who had had one of the index procedures during the 2007–2009 observation period were followed for one additional month after the month of their index surgery to capture all-cause readmissions.
Results
Demographic and clinical characteristics
For the purpose of the study, 218,437 hysterectomies were identified in the data base. The patients who underwent 210,916 (96.6%) of these procedures were retained in the analysis following application of the inclusion/exclusion criteria described above. Overall, a large proportion (74%; abdominal: 55%; vaginal: 19%) of the surgeries were done without the use of laparoscopic technique. A greater proportion of vaginal than of abdominal procedures were done laparoscopically. Figure 1 is a flow diagram for attrition of the original study population, and Table 1 provides a categorization of the study population according to procedure code, type of surgical approach, and method of hysterectomy.
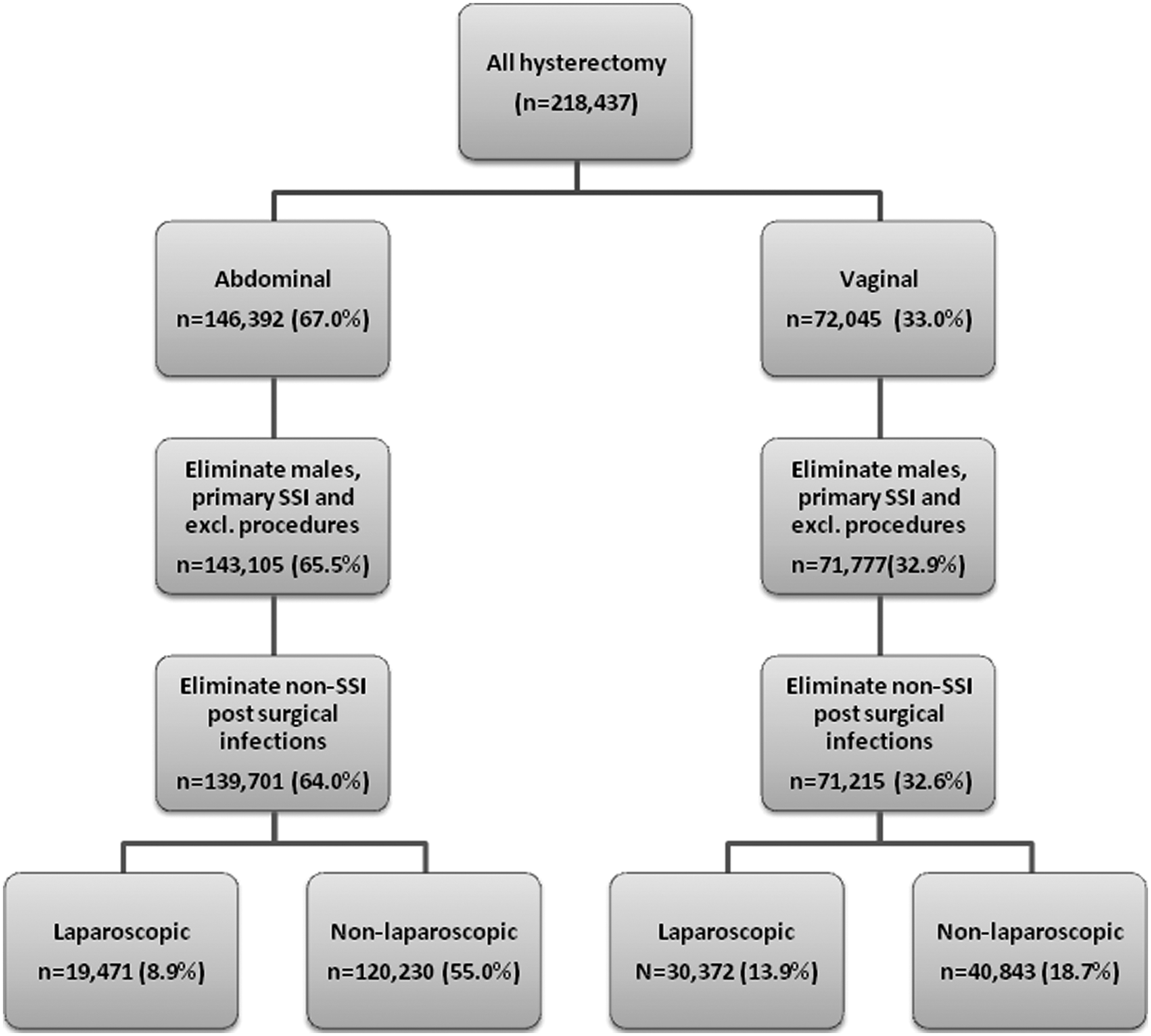
Selection of study cohorts for hysterectomy surgery.
Table 2 provides a description of the patients and providers involved in the hysterectomy surgeries investigated in the study. Patients who had vaginal non-laparoscopic surgery tended to be older than those in the other groups (mean age±standard error [SE] 49.6±0.056 y), followed by those in the abdominal non-laparoscopic group (47.1±0.033 y), abdominal laparoscopic group (46.4±0.082 y), and vaginal laparoscopic group (45.1±0.065 y). The vaginal surgery group had a lower severity-of-condition burden than did the abdominal hysterectomy group irrespective of the surgical approach adopted. Patients who underwent laparoscopic vaginal surgeries had the least mean APR-severity score (1.24±0.001), whereas those who had non-laparoscopic abdominal surgery had the greatest APR-severity score (1.38±0.001).
Column numbers indicate which cohorts show statistically significant differences; e.g., 67.1234 indicates that the distribution of races in cohort column one is statistically significantly different (p≤0.05) from the comparable racial distributions in cohort columns two, three, and four.
LMS Statistical tests are adjusted for multiple comparisons by the method of Tukey-Kramer.
Chi-square statistical tests are adjusted for multiple comparisons by the method of Bonferroni.
APR=all-patient refined.
A majority of patients within each hysterectomy surgery group were white, with the greatest proportion (72%) of these being in the vaginal laparoscopic group. The greatest proportion (20%) of black women were in the open abdominal hysterectomy group. Greater proportions of the patients who underwent laparoscopic hysterectomy in both the abdominal (79%) and vaginal (77%) surgery groups were Medicare recipients. A significant majority of patients in all of the study groups were from the southern region of the United States, and most underwent their surgeries in hospitals in urban areas. Most of the hospitals at which the patients in the study underwent hysterectomy were teaching institutions, each with 200 to 500 beds.
Surgical site infections
Table 3 presents the incidence of SSI by type of hysterectomy and surgical approach. In terms of total numbers, only patients who underwent open abdominal hysterectomies had an incidence of SSI exceeding 1%; the incidences in the other groups were between 0.2% and 0.3%. When the incidences of SSI were adjusted for baseline differences of patients' age, race, APR-severity, and geographic location, patients undergoing open abdominal hysterectomy were found to have SSI at twice the frequency (0.44%; CI 0.40,0.48) of those who underwent less invasive procedures.
The incidence of SSI as a percentage (%) of the overall incidence is adjusted for patient characteristics (age, race, APR_severity and geographic location), hospital characteristics (hospital location, bed size, teaching/non-teaching hospital, national hospital projection weights), and primary payer type.
LCL=lower confidence limit; SSI=surgical site infection; UCL=upper confidence limit.
Length of hospital stay
Patients who underwent open abdominal hysterectomy had a longer LOS than those who underwent vaginal or laparoscopic hysterectomy irrespective of whether they had an SSI or not (Table 4). However, patients who had an SSI following hysterectomy had a mean LOS that was between three- and fivefold the LOS of those who did not have an SSI irrespective of the approach to and method of hysterectomy used. Patients who had SSIs following open abdominal hysterectomies had the longest mean LOS (7.2 d; 95% CI 7.0–7.4) of those in any of the other study groups, and had a clear and significant additional LOS.
Length-of-stay (LOS) outcomes are weighted to reflect the Premier national hospital distribution.
Length of stay and cost are also adjusted for patient age, race, APR_severity, and geographic location.
APR=all-patient refined; LCL=lower confidence limit; SSI=surgical site infection; UCL=upper confidence limit.
Cost of care
On average, patients who had an SSI following hysterectomy surgery incurred twice the cost of care of their counterparts who did not have an SSI, irrespective of the approach or surgical method used (Table 4). The incremental cost was greater in the abdominal than in the vaginal surgery group for both laparoscopic and non-laparoscopic hysterectomy. The highest cost owing to SSI ($19,203; 95% CI 17,260–21,365) was for abdominal laparoscopic hysterectomy, although the increment was similar to that for SSI following non-laparoscopic surgeries. Average incremental costs of care were lower for vaginal hysterectomy than for abdominal hysterectomy for both laparoscopic and non-laparoscopic surgeries.
Hospital readmissions
Although all-cause readmissions soon after the index surgery occurred in about 5% of the study population, SSI following the index surgery was associated with a significantly greater percentage of readmissions (Table 5). Moreover, despite a relatively low overall incidence of SSI, the risk of readmission of patients who did experience an SSI was more than threefold that of those who did not have an SSI irrespective of the surgical approach to hysterectomy, ranging from 4.5%–6.2% for patients without SSIs to 16.0%–23.5% for those with SSIs.
Readmission rates, LOS, and cost are adjusted for age, race, APR-severity, geographic location, hospital bed size, and payer type.
APR=all-patient refined; LCL=lower confidence limit; LOS=length of stay; SSI=surgical site infection; UCL=upper confidence limit.
For patients who had an SSI, the LOS and costs (Table 5) related to readmissions were also significantly greater for all types of hysterectomy than for patients who did not have an SSI. Patients who developed an SSI after open hysterectomy, through either a vaginal or abdominal approach, also had a significantly greater LOS and cost of readmission than those who had an SSI after laparoscopic hysterectomy though either approach.
Additional analyses were conducted to estimate the mean LOS and costs of readmissions among patients who were readmitted. In these analyses as in those described above and shown in Table 4, the LOS and costs of readmission were greater for non-laparoscopic than for laparoscopic hysterectomy whether by the abdominal or vaginal approach. The longest mean LOS (8.9 d; 95% CI 5.5–14.3) and readmission costs (13,779; 95% CI 8,118–23,385) were found in the vaginal non-laparoscopic surgery group, followed by the open abdominal surgery group ([LOS: 7.8 d; 95% CI 6.9–8.7]; [cost: $12,143; 95% CI 10,642–13,854]).
Discussion
This study confirms earlier findings of a disproportionately higher number of hysterectomies being performed via the open, non-laparoscopic abdominal route than through either the laparoscopic abdominal route or vaginally. Approximately half of the patients in the present study of patients in an active clinical data base underwent open abdominal hysterectomies and there therefore not availed of the documented benefits of less invasive procedures.
At less than one percentage point, the overall incidence of SSI after hysterectomy found in this study may be considered low, especially in view of the data shown for such SSI in other reports, such as that of the National Healthcare Safety Network (NHSN; www.cdc.gov/nhsn). The differences are probably on the result of the data sources and the methodology used to derive the incidence rates. Thus, for example, the NHSN report is based on information reported directly by hospitals and specifically intended for clinical assessment of the observed rates of infection. In view of this it may be fair to assume that such data are coded and reported by the clinical staff at a hospital. On the other hand, administrative data bases are meant primarily for payer claims and are often coded by non-clinical staff personnel with a primary focus on the coding of a particular procedure. Our identification of SSIs was based on explicit coding to that effect or on the use of antibiotics that may suggest an SSI, in contrast to the NHSN data, in which occurrences of SSI itself are reported. Also, the NHSN offers an observed incidence of SSI, whereas the incidences of SSI in our study were adjusted for several variables so as to address the inherent variability in the types of patients undergoing different hysterectomy procedures. In addition, our rates were weighted to reflect a national, population-level incidence of SSI as opposed to the rate of SSI derived from the data base.
However, even with the low incidences of SSI that it found, the present study demonstrates that an SSI not only increases significantly the utilization of services and costs above those for the primary surgery done for hysterectomy, but also drastically increases the rates of readmission and associated utilization and costs of inpatient medical services. These numbers offer support for policies that advocate the use of less invasive approaches to hysterectomy and demonstrate the substantially lower burden of SSI that can result from such policies.
The finding of a higher overall incidence of SSI with abdominal than with vaginal hysterectomy, and with non-laparoscopic procedures generally, resembles that in a study of SSI following cholecystectomy, which found a 1% incidence of SSI during the study period [10]. Also, the finding in the present study that more invasive, non-laparoscopic operations were generally accompanied by a longer LOS than were laparoscopic surgeries resembles the findings reported in two studies reported in 2005, respectively involving hysterectomy for benign gynecologic disease and laparoscopic versus open surgery for suspected appendicitis [18,19]. As compared with open abdominal surgery, vaginal hysterectomy in one study and laparoscopic appendectomy in the other demonstrated the benefits of less invasive surgeries in the form of a shorter LOS; more rapid return to normal activity, work, and athletics; and fewer unspecified infections or febrile episodes. Although our study did not specifically examine outcomes in terms of work- or health-related quality of life, its finding of a shorter LOS with less invasive operations, combined with a lesser burden from SSI, can perhaps be safely extrapolated to offer benefits in quality of life and productivity similar to those found in thes other two studies.
The present study also confirms the findings in an earlier report that laparoscopic hysterectomy was also associated with statistically significantly fewer readmissions than were non-laparoscopic procedures [11]. Our study also demonstrated that the risk of readmission exceeded the average by more than threefold in the event of an SSI. However, the estimated mean LOS and cost of readmission were greater among patients who had a non-laparoscopic vaginal hysterectomy than among those of had an open abdominal procedure. A similar trend was observed in another study of SSIs in cholecystectomy procedures, in which most SSIs following a laparoscopic procedure were detected during post-discharge follow-up or on readmission, whereas most SSIs following open abdominal cholecystectomy were detected during the primary procedure, suggesting that SSIs may become manifest at a slightly later point after laparoscopic surgery than after an open abdominal procedure [19].
Several limitations of our study should be kept in mind when using it and its findings in clinical and economic decision making. First, it was not known whether a relatively small number of radical procedures (such as those related to diagnoses of cancer) were done on the patients included in the study, but no additional criteria were utilized to identify and exclude such procedures. The differences in characteristics of patients, including the primary severity of their conditions and the potentially different levels of risk incurred by co-morbid conditions, were adjusted by including the patients' APR-severity scores in the multi-variable analyses of SSI incidence and outcome across the study groups. However, although the multivariable analyses adjusted for observed differences in patient characteristics, unobserved differences not included in this model may bias the results. For example, the study data analysis did not control for surgeon skill and experience in performing abdominal, laparoscopic, or vaginal hysterectomy, although such factors are considered widely to affect outcomes of surgery. In addition, although claims data are valuable tools for evaluating health care utilization and costs, they are collected for payment purposes and not for research. An SSI code does not provide insight into the type of SSI to which it is being applied in terms of the tissue structures or organ spaces in which the infection occurred. Coding errors are possible, and the presence of a claim for a medication, for example, does not necessarily translate into its use. Further, since the Premier data base captures data on episodic care provided in hospital inpatient and outpatient settings, the readmission data in the data base are likely to be limited to those patients who return to the same hospital at which they had their index procedure, and are therefore likely to underestimate true readmission figures. Lastly, research based on data, such as in the present study, allows only an assessment of associations, and the findings in our study should therefore not be interpreted as reflecting clinical causality.
In conclusion, this study provides clinical evidence in support of the use of less invasive approaches to hysterectomy than open abdominal surgery. Policy makers and the clinical community should consider the constantly increasing evidence for the benefits of such less invasive procedures as opposed to open abdominal hysterectomy. In addition to other documented benefits of such less invasive procedures, the lower incidence of SSI with these procedures than with open abdominal hysterectomy, and lower incidence of associated complications and costs, should be taken into account when weighing the risks and benefits of a surgical approach for patients whose conditions warrant a hysterectomy.
Footnotes
Acknowledgments and Author Disclosure Statement
This study was funded by the Johnson & Johnson Global Surgery Group. At the time of the study, all of the authors were employees of the Johnson & Johnson Global Surgery Group. The authors were responsible for developing the study design, and for the data analysis and writing of the manuscript. Johnson & Johnson, Inc., manufactures devices that are used in both open and minimally invasive surgeries. However, no specific device was in conflict of interest with respect to the subject of this study.