
Abstract
Abstract
Background:
Cefazolin remains the preferred preoperative antibiotic for the majority of surgical procedures. However, outcome evidence supporting current dosing recommendations for pre-operative prophylaxis is scarce, particularly for obese patients. With more than 33% of adults in the United States classified as obese, it is crucial that we determine the correct dosing regimen in order to maximize the potential to prevent surgical site infections (SSIs). The purpose of this study was to evaluate whether surgical prophylaxis with cefazolin 2 g, as recommended by practice guidelines, is as effective in preventing SSIs in obese as compared to non-obese patients.
Methods:
In retrospective fashion, data were collected from the electronic medical records of patients who received 2 g of cefazolin preoperatively during a 13-mo period. Patients who met the inclusion criteria were allocated to an obese (n=99) and non-obese (n=96) group according to body mass index (BMI). Charts were reviewed for identification of SSIs as defined by the U.S. Centers for Disease Control and Prevention. For the primary outcome, the numbers of SSIs in the two groups were compared using the Pearson χ2 test.
Results:
Patient characteristics were similar in the two groups with the expected exception of weight (mean 90 vs. 110 kg; p<0.001) and BMI (27 vs. 35 kg/m2; p<0.001). The highest patient weight was 182 kg with a BMI of 55 kg/m2. The most common surgical service was orthopedics/hand, accounting for 35% of patients. No significant difference was found in the number of SSIs in the two groups (7 vs. 5; p=0.56). No differences between weight and BMI were seen in patients with or without a SSI.
Conclusions:
Obese patients may continue to receive 2 g of cefazolin preoperatively until large-scale controlled trials show differently.
I
Cefazolin is the preferred pre-operative antibiotic, endorsed by several guidelines for the majority of surgical procedures, owing to its established safety, favorable cost, and narrow spectrum of activity [4,5]. Pre-operative dosing recommendations for intravenous cefazolin are based on weight such that adult patients weighing <80 kg and >80 kg receive 1 and 2 g, respectively. Moreover, evidence is accumulating highlighting the importance of tailoring dosing regimens based on body weight because of the altered pharmacokinetics and pharmacodynamics [6–8]. This is important because obesity is a major risk factor for SSI, and more than 33% of adults in the United States are classified as obese; thus, it is crucial that we determine the correct dosing regimen in order to maximize the potential to prevent SSIs [9,10].
Pharmacokinetic studies evaluating the adequacy of current and investigational pre-operative cefazolin dosing regimens in obese patients have yielded conflicting results [11–14]. One small study found 2 g of cefazolin produced subtherapeutic tissue concentrations [14]. However, a study of morbidly obese patients undergoing gastric bypass surgery found a 2-g pre-operative cefazolin dose did not differ from 3 g in mean total serum cefazolin concentration or fraction of time above the targeted minimum inhibitory concentration (MIC) [11]. Despite the lack of outcome evidence guiding cefazolin dosing in obese patients, the clinical practice guidelines for pre-operative antibiotic prophylaxis released in 2013 state that a pre-operative cefazolin dose of 3 g can be justified for patients weighing ≥120 kg [4].
Nonetheless, although pharmacokinetic data suggest that 2 g of cefazolin preoperatively may produce subtherapeutic tissue concentrations, no studies have specifically evaluated whether 2 g is ineffective in preventing SSIs in obese patients. The primary objective of this study was to evaluate whether surgical prophylaxis with cefazolin 2 g is as effective in preventing SSIs in obese patients (body mass index [BMI] ≥30 kg/m2) as compared to non-obese patients who receive the same cefazolin dose.
Patients and Methods
This study was a retrospective electronic chart review conducted with the approval of the research and development committee and the Institutional Review Board of our institution. A waiver of informed consent was granted for the study. The James A. Haley Veterans' Hospital (JAHVH) is a 415-bed academic medical center with more than 6,500 surgical procedures performed annually on site while maintaining 96% compliance with the Surgical Care Improvement Project (SCIP) core measure addressing prophylactic antibiotic given within 1 h prior to surgical incision.
Potential patients were identified using a computer report generated by the Veterans Health Information Systems and Technology Architecture program, extracting all patients who received cefazolin 2 g during the 13-mo period between July 1, 2009 and August 1, 2010. A sample size of 183 patients was calculated as being necessary to complete the study with a 5% margin of error and 95% confidence. This figure was rounded to aim for a sample of 100 obese and 100 non-obese patients. Obese patients were defined as having a BMI ≥30 kg/m2 according to the standards of the World Health Organization [15]. Patients were then selected for inclusion by a systematic review of every fifth patient in the report until approximately 100 patients had been identified in each group.
To qualify for inclusion in either group, patients must have undergone surgery at the JAHVH, weighed at least 80 kg regardless of BMI at the time of surgery, and received cefazolin 2 g within 1 h of surgical incision. If no weight was available at the time of surgery, the most recent weight recorded within 30 d of surgery was used to determine inclusion. Patients were excluded if they were receiving antibiotics for an active infection, received another pre-operative antibiotic concurrently with cefazolin, had undergone urologic surgery, or lacked medical follow-up within 30 d of surgery. Urologic surgery patients were excluded because of the inability to differentiate SSIs accurately from urinary tract infections in such cases.
Data collected from the Department of Veterans Affairs' Computerized Patient Record System included presence of an SSI, age, height, weight, BMI, blood glucose concentration closest to the time of surgery, tobacco use, surgical service performing the procedure, surgical procedure including whether it was laparoscopic, incision class, duration of surgery, number of cefazolin doses administered intraoperatively, whether the patient remained an inpatient or was discharged home postoperatively, and the name and duration of post-operative antibiotic. The SSIs were confirmed in agreement with the U.S. Centers for Disease Control and Prevention, which defines a SSI as an infection occurring within 30 d of a surgical procedure if no implant is placed and involving either the skin or subcutaneous tissue around the incision, deep soft tissue such as muscle, or an organ or space other than an incised body wall [16,17]. If an implant is inserted, then an SSI may be identified as long as one year after the surgical procedure. Using SAS® Enterprise Guide Version 4.3 (SAS Institute Inc., Cary, NC), the Pearson χ2 and Fisher exact tests were used to compare nominal data, including the primary outcome as appropriate. The Student t-test was used to compare continuous variables such as patient characteristics. Results were considered statistically significant at p<0.05.
Results
Over a three-month period, 345 charts were reviewed to identify 195 patients who met the criteria for inclusion in the study. The non-obese and obese groups consisted of 96 and 99 patients, respectively. Most exclusions were for urologic surgery; only a handful of patients were deemed ineligible because of lack of follow-up.
Patient characteristics are presented in Table 1. Overall, patients in the non-obese and obese groups were similar with the expected exception to average weight (90±11 vs. 110±18 kg; p<0.001) and BMI (27±2 vs 35±5 kg/m2; p<0.001). For the primary outcome, there were seven SSIs in the non-obese group and five SSIs in the obese group (p=0.564). Of the 12 SSIs, 10 were superficial incisional and two were organ space.
All values represent mean±standard deviation unless otherwise stated.
As seen in Table 2, non-obese and obese patients with SSIs differed only in average BMI (28±2 vs. 37±5 kg/m2; p=0.037) and tobacco use (0 vs 60%; p=0.046). The characteristics of patients with SSIs did not differ from those of patients without SSIs (Table 3). The average weight of patients with and without an SSI was 101 kg and 100 kg, respectively. No association with weight or BMI and SSIs was observed (Fig. 1).
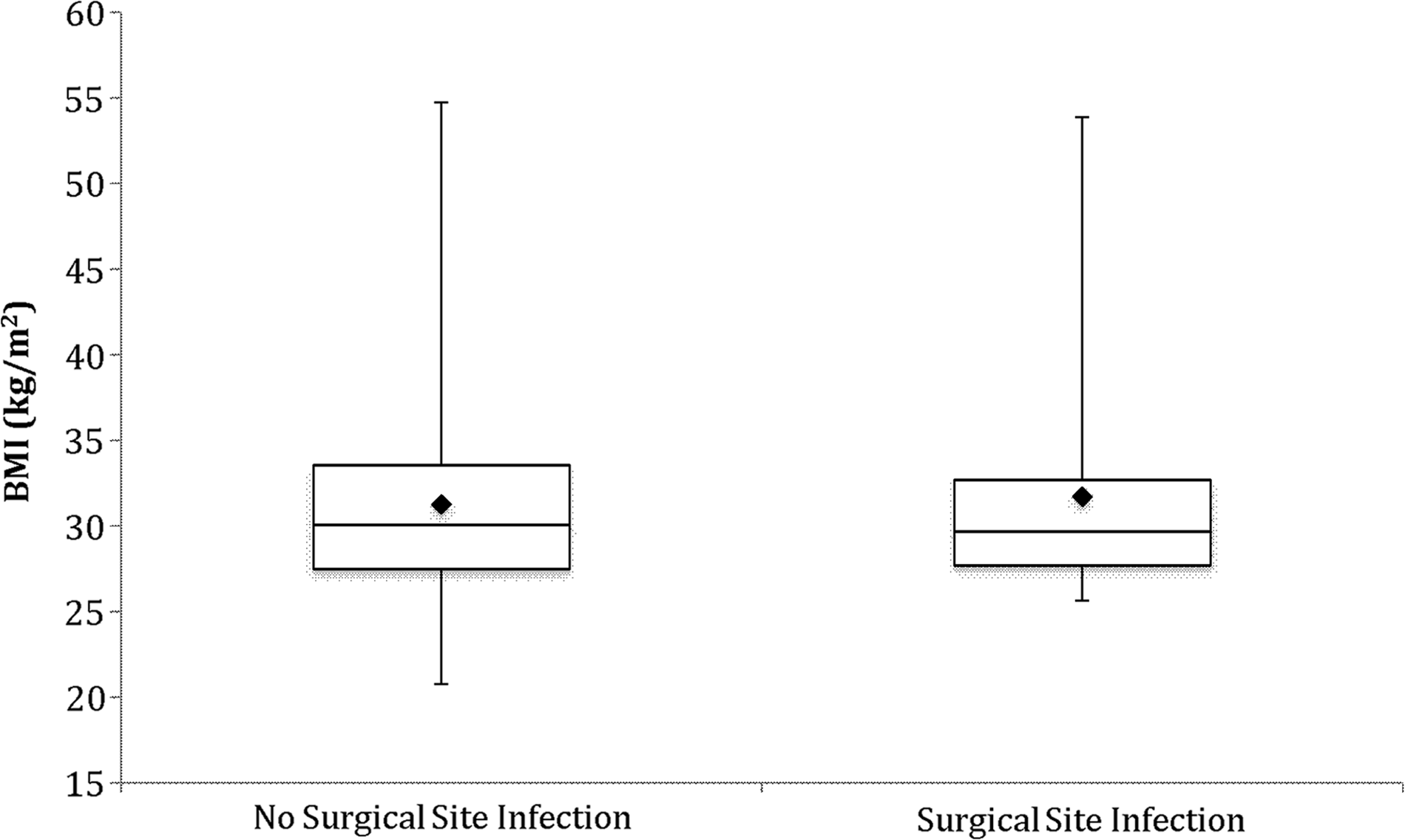
Relation between surgical site infections and body mass index. No difference was found between the mean BMI of patients with or without a surgical site infection (p=0.783).
All values represent mean±standard deviation unless otherwise stated.
N/A=not applicable.
All values represent mean±standard deviation unless otherwise stated.
Approximately 50% of the patients in each group received post-operative antibiotic, with 88% of the non-obese and 85% of the obese patients receiving intravenous and the rest oral drug. There was no statistical difference between the groups in post-operative antibiotic selection. The most common intravenous and oral post-operative antibiotic was cefazolin (75%) and amoxicillin/clavulanic acid (10%), respectively. Orthopedics/hand operations accounted for the highest proportion (35%) of surgical procedures in both groups; moreover, placement of implants occurred in 40% of all cases. Types of surgical procedures were no different in the two groups, with equal distributions of aortic valve replacements, coronary artery bypass graft surgery, total hip replacement, and total knee replacement.
Organisms were isolated in six patients with an SSI: methicillin-sensitive Staphylococcus aureus, S. haemolyticus, S. lugdenensis, Enterococcus faecium, Klebsiella pneumoniae, Acinetobacter baumannii, and Propionobacterium acnes.
Discussion
Additional or alternative pre-operative cefazolin dosing strategies may not be necessary for obese patients, as demonstrated by the absence of a significant difference in the SSI rate for non-obese and obese patients in this study. In 1989, Forse et al. demonstrated that 2 g of cefazolin was more effective than 1 g at preventing SSIs in morbidly obese patients with a mean BMI 47 kg/m2 (16.5% to 5.6%; p<0.03) [18]. However, since then, no study has been conducted to determine whether 2 g is sufficient to prevent SSIs for all obese patients. Like those investigators, we found that the 2-g dose remains an acceptable option to reduce the incidence of SSIs; however, we question whether 80 kg is the appropriate weight cutoff for the use of a 2-g dose or whether 1 g would be effective for patients weighing between 80 and 100 kg.
As previously mentioned, published outcome studies evaluating cefazolin dosing regimens in obese patients are sparse. However, there are several cefazolin pharmacokinetic trials that have been used to guide recommendations. In 2004, Edmiston et al. found that after a single 2-g pre-operative dose of cefazolin, the tissue concentration was therapeutic in only 48.1%, 28.6%, and 10.2% of obese patients with a BMI of 40–49 kg/m2 (n=17), 50–59 kg/m2 (n=11), and ≥60 kg/m2 (n=10), respectively [14]. Unfortunately, the series was not large enough to determine whether suboptimal tissue concentrations translated into SSIs, nor was there a non-obese control arm.
In 2011, Pevzner et al. reported inadequate adipose tissue concentrations of cefazolin in obese women (n=29) undergoing cesarean delivery who received 2 g of the drug preoperatively [13]. Significantly lower cefazolin concentrations were seen in patients with a BMI 30–39.9 kg/m2 (6.37 mcg/g; p=0.009) or ≥40 kg/m2 (4.25 mcg/g; p<0.001) compared with non-obese patients (9.37 mcg/g), yet the cefazolin concentrations in each arm are ahove the MIC for susceptible wound pathogens. This study, as with the studies discussed previously, was not designed nor powered to evaluate SSIs; in addition, the altered pharmacokinetics of pregnancy would have affected the distribution of cefazolin. Although the last two studies suggest 2 g of cefazolin results in subtherapeutic tissue concentrations, it is difficult to apply the data to the general population given the small sample sizes and without knowing the impact on the rate of SSIs.
A single 2-g dose of cefazolin was shown to maintain therapeutic concentrations against methicillin-sensitive S. aureus for at least 4 h in 20 morbidly obese patients weighing as much as 260 kg in a study by van Kralingen [12]. However, those authors did not investigate tissue samples, nor did they comment on achieving the target MIC for gram-negative pathogens encountered commonly in SSIs.
Ho et al. conducted the only pharmacokinetic study that analyzed a pre-operative 3-g dose of cefazolin in obese patients [11]. Their analysis, in patients with a BMI >50 kg/m2, revealed no difference in the mean total concentration or fraction of time above the targeted MIC for the 2- and 3-g doses. It is important to note that the cefazolin concentrations examined in their study reflect serum and not tissue concentrations. Considering the results from our investigation and the pharmacokinetic evaluation of 3 g in morbidly obese patients, it appears that increasing the pre-operative cefazolin dose to 3 g does not provide an incremental effect.
No patient characteristics were identified as risk factors for the development of an SSI in this study; however, obese patients who developed an SSI tended to be tobacco users. Previously recognized risk factors include older age, poor nutrition, diabetes mellitus, tobacco use, duration of surgery, obesity, steroid use, duration of hospitalization prior to the procedure, and transfusion of blood products during the perioperative period [16].
Overall, the SSI rate in our study appears slightly higher than national estimates [1], which may have been secondary to the advantage of using the nationwide Veterans Health Administration's electronic health record system. The extensive database facilitated accessibility to each patient's care and also minimized exclusion of patients because of lack of followup data.
Our study is limited by its retrospective design; consequently, we must rely on provider documentation and accurate reporting of SSIs. In order to gain a practical view, we included a plethora of surgical procedures and specialties, which may have made it difficult to detect a difference.
Conclusion
Pre-operative surgical prophylaxis with 2 g of cefazolin was as effective in obese as in non-obese patients. The benefit of increasing the prophylactic dose of cefazolin is unknown until prospective studies can be conducted.
Footnotes
Author Disclosure Statement
This manuscript has been seen and approved by both authors, and the material is previously unpublished. The authors have nothing to disclose concerning financial or personal relationships with commercial entities (or their competitors) referenced in this presentation.
This material is based on work supported by the Office of Research and Development of the Department of Veterans Affairs.
Disclaimer: The contents do not represent the views of the Department of Veterans Affairs or the United States Government.