
Abstract
Abstract
Background:
The lung is the most common site of coccidioidomycosis, with extrapulmonary sites of infection being described rarely. To date, the pancreas has not been reported as an isolated site of coccidioidomycosis.
Methods:
Case report and literature review
Case Report:
Computed tomography (CT)-guided biopsy and gram staining of the pancreatic lesion of an immunocompetent patient without known risk factors revealed coccidioidomycosis of the head of the pancreas without malignant neoplasm or atypia. Serologic tests yielded positive titers for antibodies to Coccidioides lmmitis. The patient responded to treatment with fluconazole, as evidenced by regression of her pancreatic lesion by CT and negative serologic test results for Coccidioides upon completion of treatment.
Conclusions:
Solid masses in the head of the pancreas encountered in surgical practice are challenging in terms of both surgical technique and diagnosis. Although malignant disease remains a high possibility in the differential diagnosis of such masses, and must always be considered until proved to be absent, non-malignant etiologies should also be considered. In a number of patients with benign lesions of the pancreatic head, unnecessary surgical exploration and resection is avoidable. Although they are rare, several fungal infections of the pancreas have been reported in the literature. The unusual case of coccidioidomycosis of the pancreatic head presented here adds to the list of uncommon causes of pancreatic lesions. Surgeons and physicians managing patients in areas in which coccidioidomycosis is endemic should be aware of this rare entity.
N
Case Report
A 19-year-old female presented with a coccidioidal infection manifested as a mass in the head of the pancreas. Her history was notable for a laparoscopic roux-en-Y gastric bypass 1 mo earlier, which required post-operative endoscopic dilatation of an anastomotic stricture. On presentation, she had recurrent symptoms of nausea, vomiting, epigastric pain, and abdominal distension with diffuse abdominal tenderness on palpation. She denied having a history of fever, hemoptysis, or cough. She was a non-smoker and lived in the Central Valley of California, where she was a student. Her past medical history was notable for diabetes mellitus.
A computed tomographic (CT) scan of the patient's abdomen demonstrated free air and an incidental large, multicystic, partly septated mass of the pancreatic head measuring 37×38 mm (Fig. 1). The patient underwent diagnostic laparoscopy, which did not demonstrate a site of perforation. Postoperatively her pain resolved and she was discharged to her home with plans for further work-up of the mass in her pancreatic head on an outpatient basis. At an outpatient follow-up visit 1 wk after her discharge, she was asymptomatic, with an unremarkable abdominal examination. She had no rash or jaundice. A positron emission tomographic (PET)/CT scan showed a hypermetabolic uptake of 2-[fluorine-18]fluoro-2-deoxy-d-glucose (FDG) in the pancreatic head with a standardized uptake value (SUV) of 10.7 (Fig. 2), as well as non-specific mediastinal and right hilar adenopathy. The patient's serum concentration of CA19-9 was normal at 29 U/mL (normal <37 U/mL), and her white blood cell (WBC) count was 6×103/mcL, aspartate aminotransferase (AST) 20 IU/L, alanine aminotransferase (ALT) 14 IU/L, alkaline phosphatase 50 IU/L, and total bilirubin concentration 0.9 mg/dL.
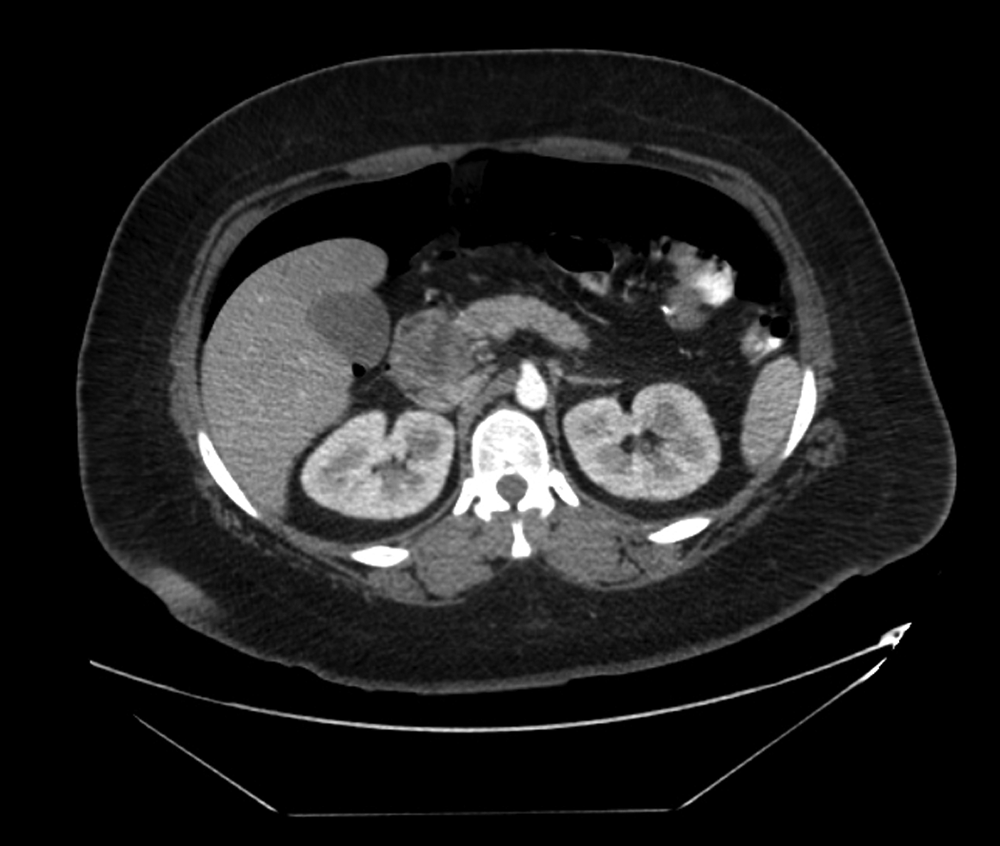
Contrast-enhanced axial computed tomography scan demonstrating a complex, partly septated mass of the pancreatic head. 227×192 mm (72×72 DPI).
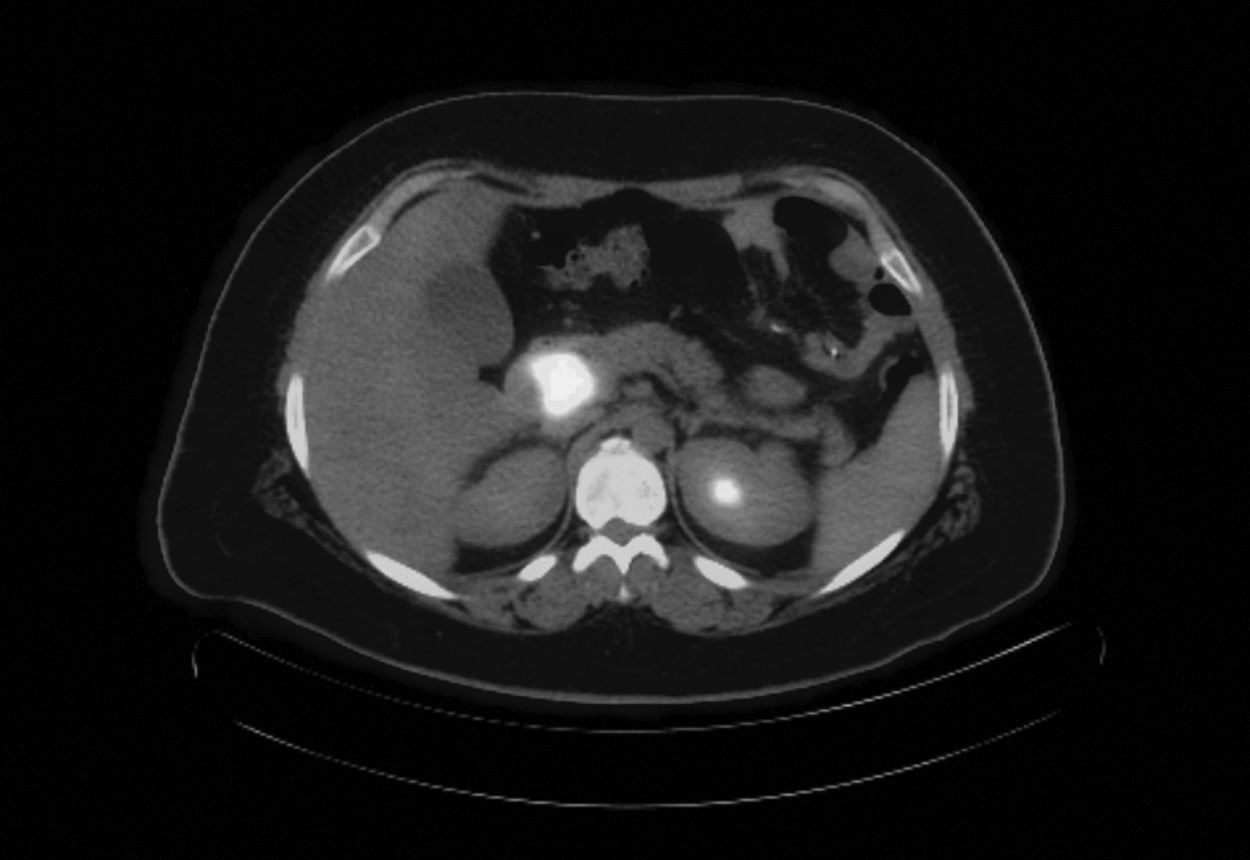
Positron emission tomography/computed tomography scan showing a hypermetabolic focus corresponding to a mass in the pancreatic head. 266×183 mm (72×72 DPI).
Computed tomography-guided needle biopsy of the patient's pancreatic mass demonstrated epithelioid granuloma with necrosis (Figs. 3 and 4). Gram stain showed coccidioidomycosis with no malignant cells or atypia. Titers of anti-Coccidioides antibody (IgG) were positive at 1:32, confirming the diagnosis of coccidioidomycosis, and antibiotic treatment was begun with a regimen of fluconazole. A repeat CT scan done 1 mo later demonstrated partial resolution of the mass in the head of the pancreas (Fig. 5), with eradication of her infection verified by negative serologic tests. She continued to do well 2 y later.
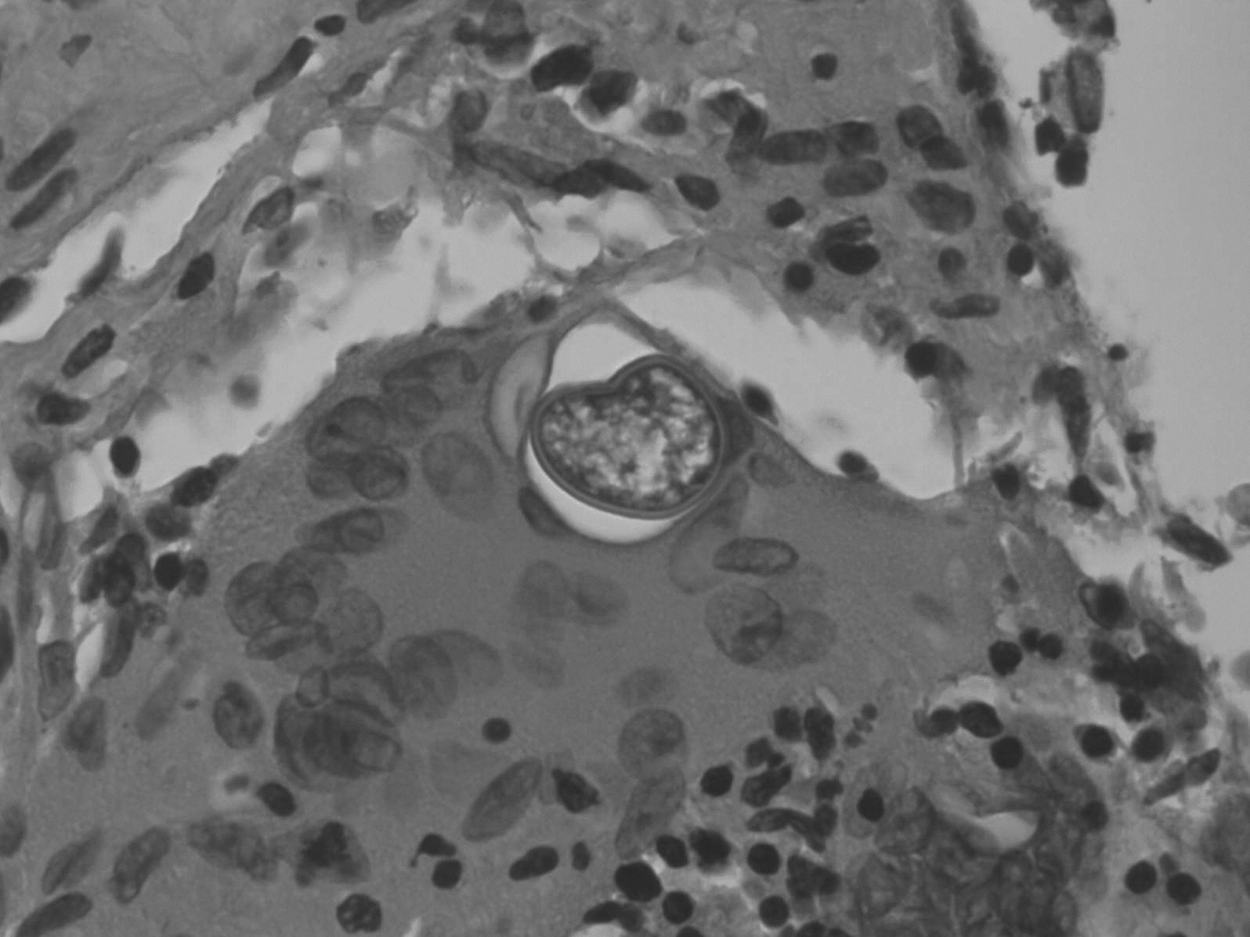
Core needle biopsy of mass in the pancreatic head showing spherules characteristic of coccidioidomycosis within the pancreatic parenchyma. 135×101 mm (300×300 DPI).
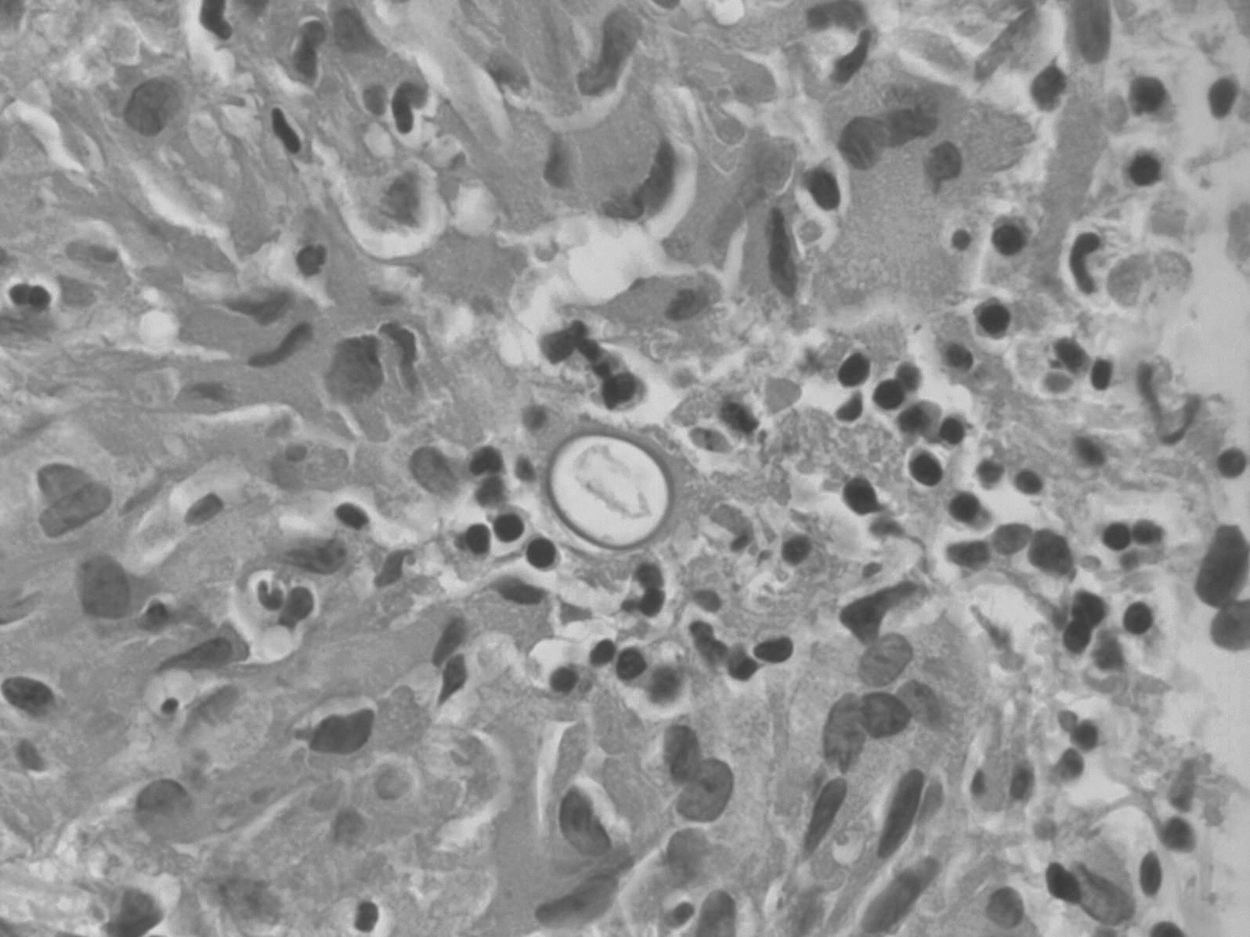
Core needle biopsy of mass in the pancreatic head mass showing spherules characteristic of coccidioidomycosis within the pancreatic parenchyma. 135×101 mm (300×300 DPI).

Repeat computed tomography (CT) scan 11 months after original CT scan demonstrating residual mass in the pancreatic head with interval improvement after treatment. 298×203 mm (72×72 DPI).
Discussion
Early cases of coccidioidomycosis were recognized first in the 1890s among agricultural workers in central California as diffuse, progressively disfiguring skin lesions [1]. The condition was fatal universally [1]. In early 1900, with California's population increasing, an acute respiratory illness known as valley fever was observed and named after the San Joaquin Valley of central California. Not until 1937 did the cause of this acute respiratory syndrome become recognized as the same organism responsible for the progressive skin disease in California agriculture workers [2].
The lung remains the most common site of coccidioidomycosis, and extrapulmonary manifestations are seen in fewer than 1% of cases [4]. Although extrapulmonary infection by Coccidioides can affect any area of the body, the most common sites of infection are the skin, lymph nodes, bones, and joints [3]. The most severe extra-pulmonary manifestation of coccidioidomycosis is meningitis. Other, less common extrapulmonary sites of infection include the uterus and popliteal area, in the form of popliteal cysts [4].
Dissemination of coccidioidomycosis is well described in immunocompromised patients (e.g., solid-organ transplant recipients or patients with immunodeficiency syndromes). However, most such infections occur primarily in the lung, even in patients with pancreas transplants [5]. The patient in the case described did not show any evidence of immunocompromised status, and did not have any other opportunistic infection. The gastric bypass procedure that she had previously undergone is not a known risk factor for opportunistic infection or immunocomprised status.
To our knowledge, coccidioidomycosis has never been reported in the pancreas. The patient presented here represents the first reported case of coccidioidomycosis of the pancreatic head. Although tissue culture of masses in the pancreatic head is an uncommon practice, the finding of epithelial granuloma with necrosis, demonstrating the spherules characteristic of coccidioidomycosis, is consistent with a diagnosis of the disease [6]. The diagnosis was confirmed by positive serum titers for anti-Coccidioides antibodies with the latex agglutination test.
Our patient was treated with fluconazole, and a repeat CT scan showed progressive resolution of the mass in the head of her pancreas (Fig. 4). Serologic tests done 3 wks after the start of treatment confirmed eradication of her infection. At a 2-y follow up, she continued to do well.
The absence of documented pulmonary coccidioidomycosis in our patient, although uncommon, has been reported previously. Skeletal, pericardial, and retroperitoneal coccidioidomycosis are examples of non-pulmonary occurrences of the disease [7,8]. Wascher et al. [3] reported a case of coccidioidomycosis occurring as a popliteal cyst in a patient without any evidence of pulmonary coccidioidomycosis. Blair, in 2007, postulated that pulmonary coccidioidomycosis usually resolved before the development of skeletal coccidioidomycosis [7].
Solid masses in the head of the pancreas are chiefly malignant, and in many instances pre-operative histologic diagnosis is not secured before their surgical exploration. The literature, however, reports a wide variety of non-malignant pathologies in surgically resected or biopsied pancreatic masses. Benign but “clinically suspicious” Whipple resections are relatively common in high-volume surgical practices. Up to 10.6% of cases of pancreatic masses in one series of 447 successive Whipple resections were found to be non-malignant post-operatively [9]. Furthermore, the pancreas, and specifically the head region, has been reported as the site of a wide variety of uncommon infections (e.g. actinomycosis, tuberculosis, nocardiosis and sarcoidosis) [10–13]. Table I summarizes the rare reported cases of unusual infections of the pancreatic head and the methods used for their diagnosis [14].
The case described herein represents a further rare instance of a mass in the pancreatic head of infectious etiology, in the form of coccidioidomycosis.
Although exceedingly rare, coccidioidomycosis of the pancreatic head should be added to the differential diagnostic possibilities for pancreatic masses, especially in patients living in areas endemic for the disease. The case report described here illustrates the advantage of pre-operative histologic diagnosis in presentations of masses in the pancreatic head. Our patient was treated medically and showed progressive post–treatment resolution of the lesion in the head of her pancreas (Fig. 5).
In conclusion, the pre-operative histologic diagnosis of pancreatic lesions can potentially avoid unnecessary surgical intervention. Nevertheless, in cases of equivocal lesions for which pre-operative histology fails to provide a diagnosis, prompt surgical exploration and resection of a localized pancreatic mass, when feasible, remains the appropriate means for achieving a cure.
Author Disclosure Statement
No competing financial interests exist.