
Abstract
Abstract
Background:
There is a lack of evidence-based criteria to assist the diagnosis of infection following trauma splenectomy (TS). However, the literature suggests that white blood cell count (WBC) is associated with infection in patients who undergo TS. We sought to find whether there exist key differences in laboratory and clinical parameters that can assist the diagnosis of infection after TS.
Methods:
We evaluated all consecutive trauma patients who had undergone TS at a Level 1 trauma center from 2005 to 2011 for the development of infection. To do this, we compared the values of demographic, laboratory, and clinical variables of infected and non-infected patients on odd post-operative days (POD) in the period from 1–15 days after TS.
Results:
Of 127 patients who underwent TS, 25 died within 48 h after the procedure and were excluded from our analysis, leaving, 102 patients for investigation. In the 41 (40%) patients who developed an infection, the mean day for the first infectious episode was POD 7 (range, POD 4–14). The three most common infections were pneumonia (51%), urinary tract infection (24%), and bacteremia (20%). An evaluation of laboratory and clinical parameters showed no differences in the WBC of the patients who did and did not develop infections at any time in the 15 d after TS. However, the platelet count was statistically significantly higher in non-infected patients on POD 3–9 and on POD 13, and maximal body temperature was statistically significantly higher in the infected group of patients during the first week after TS. Differences in laboratory and clinical values of the infected and non-infected patients were greatest on POD 5.
Conclusions:
Patients who undergo TS have high rates of infectious complications. The WBC is not a reliable predictor of infection in these patients in the 2 wks following TS. However, patients who do not develop infection after TS have statistically significantly higher absolute platelet counts and rates of change in their daily platelet counts than those who develop infection.
T
Critically ill trauma patients have a higher risk of infection than those in a surgical intensive care unit (SICU) [7]. Studies have estimated that the frequency of infectious complications in critically ill trauma patients can range from 5.7% [8] to 45% [6]. The etiology of such infection is multi-factorial. Trauma patients undergo emergency procedures such as intubation, central catheter placement, and tube thoracostomy, in which the use of sterile technique may not be absolute, at higher rates than do patients without trauma. Trauma and blood transfusion may also be associated with transient immunosupression [9,10]. Additionally, trauma ICUs have higher rates of utilization of various devices than do other types of ICUs [11].
Despite the greater frequency of non-operative management for blunt splenic trauma, from 10%–40% [12–14] of patients with such trauma still undergo emergent splenectomy for life-threatening hemorrhage. Patients who undergo splenectomy exhibit immune abnormalities that can increase their susceptibility to infection [15,16]. Overwhelming post-splenectomy infection (OPSI) syndrome is a rare and dreaded condition associated with a high mortality rate [17,18]. However, other post-operative infectious complications of splenectomy are much more common than OPSI and are responsible for high rates of morbidity, mortality, and increased medical expense [19,20].
Prior study has demonstrated a higher frequency of post-operative infectious complications among patients who have had a trauma splenectomy (TS) than in a matched cohort that underwent laparotomy without splenectomy for trauma [21]. The patients who had TS experienced more frequent post-operative pneumonia and had a higher incidence of multiple infections. Physiologic leukocytosis and the high prevalence of SIRS after splenectomy make the early identification and treatment of infection especially challenging in the population that has TS [6]. We sought to identify whether there were additional clinical parameters that might increase the clinical ability to differentiate infected and non-infected patients following TS.
Patients and Methods
The records of all trauma patients who underwent a total splenectomy at a Level 1 trauma center from January 1, 2005 through September 30, 2011 were reviewed retrospectively. Data were collected from patients' paper charts, the electronic medical record system used by the trauma center (Epic Systems Corporation, Madison, WI), and the trauma registry (TraumaBase, Clinical Data Management, Genesee, CO).
Data were recorded for odd post-operative days (POD) for 2 wks. The data collected consisted of patient demographics (age, gender, mechanism of injury), injury information (Abbreviated Injury Scale [AIS] score for head, chest, and abdominal injury; Injury Severity Scores [ISS]); and outcomes (total hospital length of stay [LOS], intensive care unit [ICU] LOS, and mortality). Clinical variables recorded included maximal daily temperature, maximal daily leukocyte count with its corresponding platelet count, maximal and 7AM heart rate (HR), and blood pressure (BP), minimal BP, and net daily fluid balance.
Patients were categorized into an infected group and a non-infected group. Infection was defined using the criteria of the U.S. Centers for Disease Control and Prevention, with confirmation of a positive blood, urine, respiratory, wound, or intra-abdominal fluid culture. The day of infection was determined as the date on which the first positive culture specimen was drawn. Patients who died within 48 h after admission were excluded from the analysis of the study data.
Data were analyzed with SPSS software (SPSS Inc., Chicago, IL). A value of p ≤0.05 was considered statistically significant. Numeric data were expressed as mean±standard error of the mean (SEM). Numeric data for the infected and non-infected patients were compared with through use of the Student t-test or a non-parametric test, as appropriate. Categorical data were compared through use of the χ2 or Fisher exact test. A generalized estimating equation was used to examine the rate of change in platelet counts across time for infected and non-infected patients. The study was approved by the institutional review board of the center at which it was conducted.
Results
General characteristics
Of the 17,767 patients admitted for trauma whose cases we reviewed during the study period, 127 patients underwent TS and 25 patients died within 48 h after TS, leaving 102 patients whose data were eligible for inclusion in the study. Characteristics of the patients in the infected and non-infected groups in the study are shown in Table 1. Patients in the infected and non-infected groups were of similar age, were represented in similar proportions by gender, and had similar rates of blunt trauma. The patients in the infected group were significantly more severely injured than those in the non-infected group, with severe chest injuries. There was no difference in mortality in the two groups, but the LOS of the infected patients in both the hospital and the ICU were significantly longer than those of the non-infected patients.
AIS=abbreviated injury scale; ICU=intensive care unit.
The study population and infectious complications are summarized in Figure 1. Infection was identified in 41 (40%) patients. The mean day of diagnosis of infection was post-operative day (POD) 7 (range, POD 4–14), and six patients had multiple infections. There were 21 cases of pneumonia, 10 urinary tract infections, 8 cases of bacteremia, 4 cases of intra-abdominal infection, and 4 wound infections.
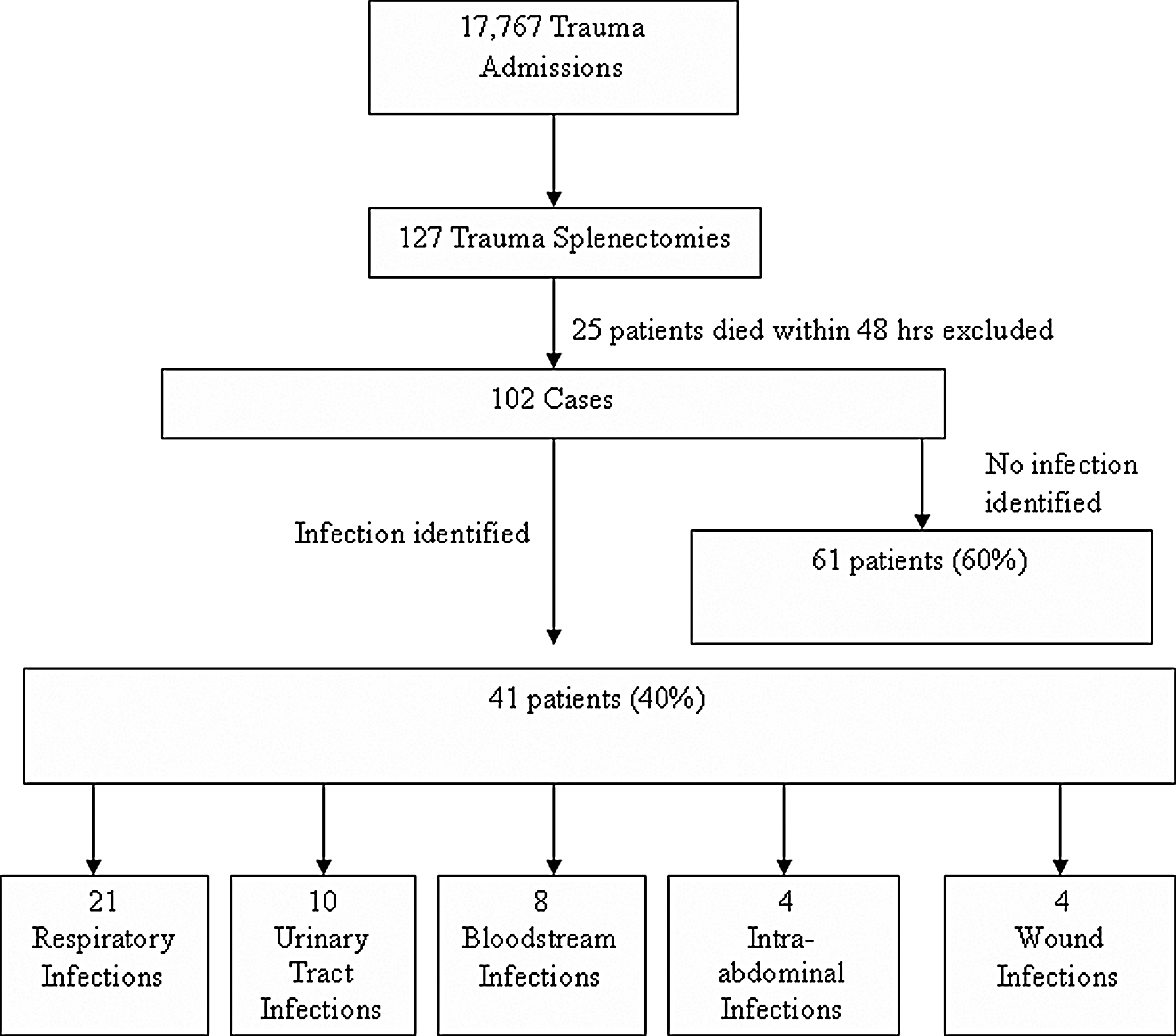
Flow diagram of steps in selection of the study population, and number of patients at each step and of patients with different types of infections following trauma splenectomy.
Analysis of clinical parameters of infected and non-infected trauma splenectomy patients
The infected and non-infected patient groups had significant differences in various clinical parameters, as summarized in Table 2. Infected TS patients had significantly higher maximal daily body temperatures (Tmax) (range 38.1°C–38.5°C) than their non-infected counterparts (range 37.4°C–37.8°C) on every day of the study period except for POD 15. This difference in temperature became most pronounced on POD 7 (mean Tmax 38.5°C for the infected patients vs. 37.5°C for the non-infected patients, p<0.01).
BP=blood pressure; POD=post-operative day; WBC=white blood cell count.
Infected TS patients also had higher peak HRs than the non-infected group during the study period. As with temperature, this difference was also greatest on POD 7 (mean peak pulse 121 beats/min vs. 100 beats/min, respectively, p<0.01). Additionally, heart rates at 7 AM were also greater in the infected than in the non-infected group on POD 1, 7, and 11.
A comparison of mean daily maximal WBC in the infected and non-infected patient groups during the study period, with the SEM for each group, is shown in Figure 2. There was no statistically significant difference in daily maximal WBC in the two groups on any day of the study period.
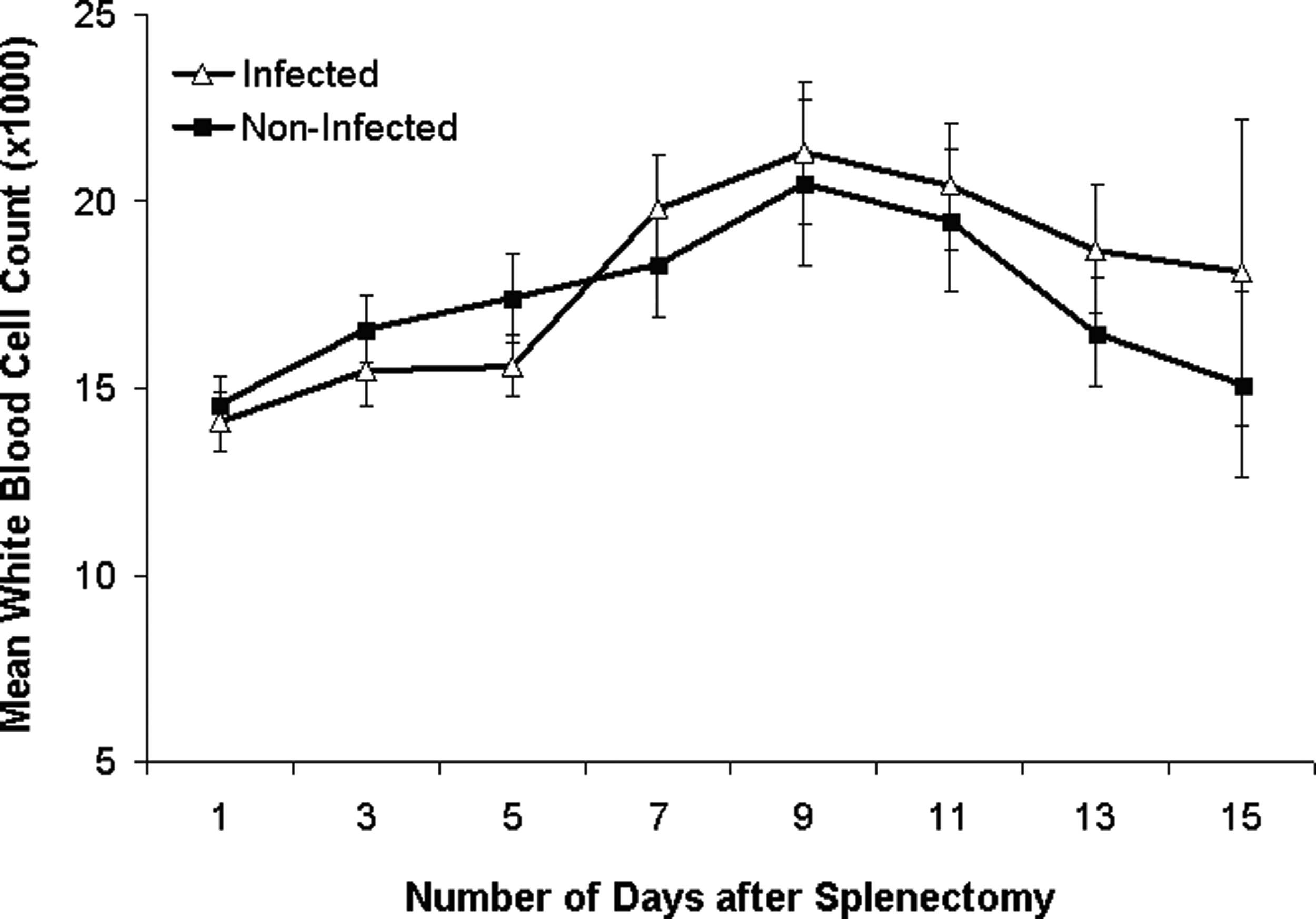
Mean daily maximal white blood cell counts of infected and non-infected trauma splenectomy patients during study period of post-operative days 1–15.
A platelet count was obtained from the same complete blood count result used to identify the maximal WBC. Mean platelet counts were higher in the non-infected group than in the infected group on every day of the study period, as seen in Figure 3. The platelet counts in the two groups showed a statistically significant difference with time (p<0.001). Contrasts of the two groups' platelet counts at specific time intervals after TS showed statistically significant differences from POD 5–7, 7–9, 9–11, and 11–13. There was no statistically significant difference in the two groups' platelet counts from POD 1–3 and POD 3–5.

Mean platelet counts of infected and non-infected trauma splenectomy patients during study period of post-operative days 1–15.
Additionally, a platelet count of 200×103/mm3 became a clinically relevant cutoff value for the infected as opposed to the non-infected patients. Patients whose platelet counts exceeded 200×103/mm3 on POD 3, 5, and 7 were significantly less likely to have a diagnosis of infection than those with a platelet count below this value on any of these same days (POD 3, 26% vs. 51%, p=0.03; POD 5, 47% vs. 81%, p=0.005; and POD 7, 71% vs. 96%, p=0.025, respectively).
Discussion
Our study demonstrates that values of clinical parameters show observable differences that can be used to identify infection in TS patients. Authors of previous papers have indicated that TS patients who develop an infection have higher and more persistently elevated maximal WBCs than those who do not develop an infection, and that a WBC above 20×103/mcL beyond 10 d after TS should prompt a search for infection [22]. In their study, Rutherford et al. compared the response of the WBC to bacteremia in patients who had a splenectomy and those who had a splenorrhaphy. They found a higher peak WBC in post-splenectomy than in post-splenorrhapy patients with bacteremia, but that the WBC could not be used to predict bacteremia in individual patients. Rutherford et al. found no statistical difference in maximal WBC counts in post-splenectomy patients who had bacteremia and those for whom either no blood culture was done or who had a negative blood culture result. They attributed this finding to an error caused by a small sample size. They also concluded that greater injury severity, as measured by the ISS, increased the risk of bacteremia. Our study sampled patients with a broader range of infections that included urinary tract infection, pneumonia, intra-abdominal abscesses, and surgical site infections, in addition to bacteremia. Additionally, all of the patients in our study were status post-splenectomy, which controlled for the immunogenic contribution of the spleen. We were unable to demonstrate a difference in maximal WBC in infected and non-infected patients following TS.
A separate recent retrospective study identified three factors as predictive of sepsis in TS patients: An injury severity score (ISS) >16, a WBC of 15×103/mcL, and a platelet count-to-WBC ratio (PC/WBC) of <20 on POD 5 [23]. This study that found this demonstrated that when all three factors were present, the probability of sepsis was 96%, and that when the WBC exceeded 15×103/mcL and the PC/WBC was less than 20, the probability of sepsis was 80%. When all three criteria were absent, the probability of sepsis was 2.5%. Our findings correspond with the observation in the study in which these findings were made that platelet counts are higher and rise faster in non-infected than in infected TS patients. A finding in our study was that by POD 5, the platelet count was an independent predictor of infection. Additionally we found statistically significant differences in body temperature in infected and non-infected TS patients. Infected TS patients had significantly higher maximal daily body temperatures than non-infected patients. We also found that the WBC count is not a reliable indicator of infection in patients who have had TS, as there was no observed statistically significant difference in the WBCs of the infected and non-infected patients in our study.
Validation of these cut-off values in a prospective series found that when two of the three risk factors described above were present, patients had an associated rate of infection of 79% [24]. However, the investigators who made this finding noted that non-infected patients who had undergone TS had WBCs above 15×103/mcL both before and after POD 5 and 6. Our study supports the limited effectiveness of the WBC in predicting infection in TS patients. Additionally, use of the specific cut-off values to identify infection in the study just described had a narrow clinical window, limited to the first post-operative week.
Our study showed a more rapid rate of thrombocytosis in non-infected TS patients, which persisted throughout the study period. Use of this information may allow the earlier diagnosis and treatment of infectious complications in the TS patient population. In our study the mean day of diagnosis of infection was POD 7; however, clinical predictors of infection were present on POD 5. Infected TS patients had an average total hospital LOS that was 15 d longer than that of non-infected patients, and an average LOS in the ICU that was 16 d longer than that of non-infected patients. Earlier diagnosis and treatment of infectious complications of splenectomy may contribute to a reduction in the use and cost of ICU or total hospital resources.
We found additional differences in several clinical parameters in infected and non-infected TS patients. Peak heart rate was significantly higher in the infected group on every day of the study period. This difference was most apparent on POD 7.
Our study had several limitations. The data were from a single institution, and the retrospective nature of the study may have introduced bias. We were unable to determine the rationale behind the decision to obtain cultures to rule out infection. We sought to minimize any selection bias by allocating patients to the infected group only if they had a positive culture. Owing to the small sample size of the study, all infectious complications were consolidated into a single group, without regard to severity or type of infection. Furthermore, the relatively small sample size of the study prevented sub-group analysis of each type of infection. The method we selected for day of infection was based on the day of the first positive culture. A prospective study is needed to validate these findings.
In conclusion, this study demonstrates that several clinical parameters can be used to identify post-operative TS patients at higher than average risk for infection. Analysis of specific clinical and laboratory trends, such as in maximal body temperature and platelet count, may allow the earlier identification and potential treatment of infection in patients who have undergone TS. Patients whose platelet counts fail to rise above 200×103/mm3 in the first week after TS should be suspected of having an occult infection and should undergo further diagnostic investigation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.