
Abstract
Abstract
Background:
Many case reports describe tuberculosis (TB) co-existent with a malignant neoplasm. However, the neoplasm in most of these reports is lung or breast cancer, with only two cases of liver cancer concomitant with TB reported in the literature. Although both TB and cancer are very common diseases, little attention has been given to the pathophysiologic and practical implications of their co-existence.
Methods:
Case report and literature review.
Case Report:
A 73-year–old female patient with a history of hypertension and hepatitis C presented with abdominal pain of 2 mos duration. Laboratory findings showed an elevated serum concentration of α-fetoprotein. A computed tomography scan demonstrated a solitary hypodense tumor in the right lobe of the liver (segment VIII). A pre-operative chest radiograph was within normal limits. The patient underwent an uneventful tumor resection. Histologic examination of a surgical specimen of the tumor demonstrated a moderately differentiated hepatocellular carcinoma co-existent with caseating granulomas.
Conclusion:
Through this case report, the authors discuss the pathogenesis of the rare association of TB and malignant neoplasm of the liver, and present a review of the current literature on the association of TB and cancer. Further research is required to determine whether a TB infection resembles other chronic infections and inflammatory conditions in having a potential to facilitate oncogenesis.
T
F=female; HCC=hepatocellular carcinoma; NA=not available.
Case Report
A 73-year-old female with a history of hypertension and hepatitis C presented with right upper abdominal pain of approximately 2 mos duration. Upon admission the patient was well and her vital signs were normal. Physical examination revealed no signs of ascites, malnutrition, or hepatomegaly. The patient's spleen was palpable about 1 cm below the left costal margin. A tuberculin skin test was not performed. Laboratory findings showed an elevated serum concentration of α-fetoprotein (42.48 mcg/L). The patient's liver transaminase activities were mildly elevated, in the presence of a normal total bilirubin concentration. Her albumin and coagulation factors were within normal limits. Serology for hepatitis C was positive, with negative results for hepatitis B virus. A chest radiograph was normal. Abdominal ultrasonography revealed a hyperechoic heterogeneous lesion in the right lobe of the liver. A computed tomography (CT) scan demonstrated a solitary hypodense tumor measuring 2 cm in diameter in the right lobe of the liver (segment VIII) (Fig. 1).
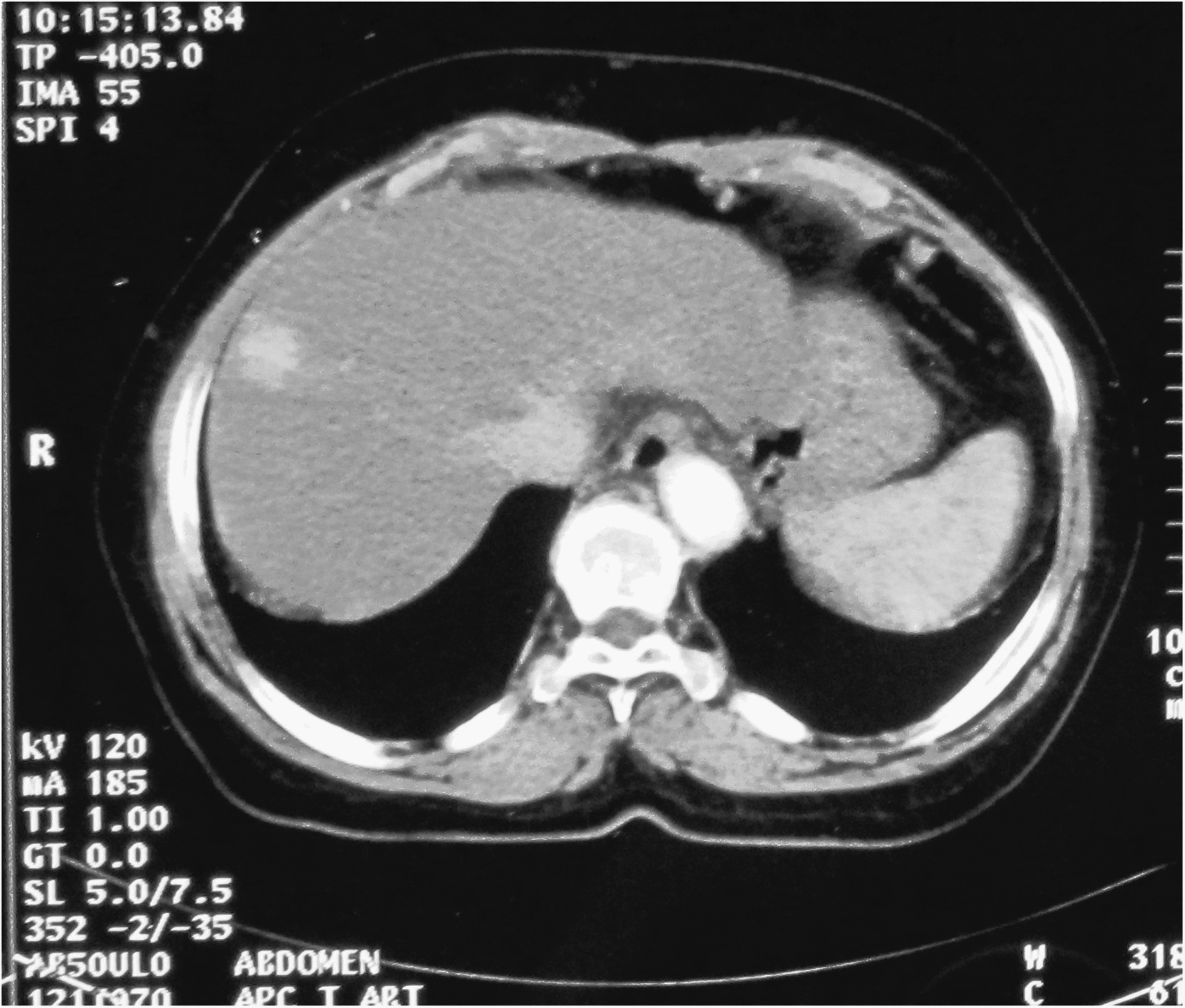
Computed tomography scan demonstrating a 2-cm nodular hypodense intra-hepatic lesion located in segment VIII of the right lobe.
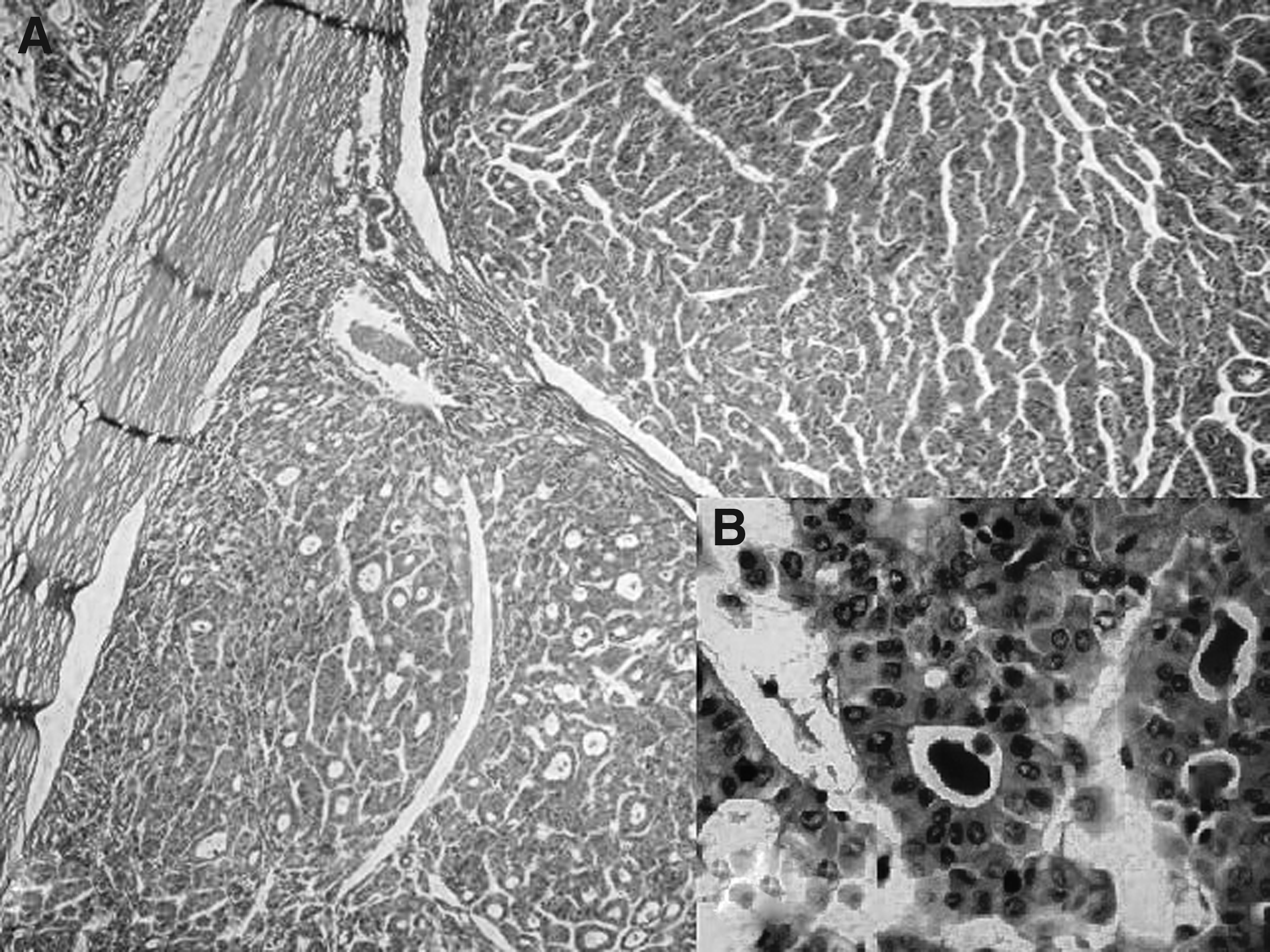
The patient underwent hepatic resection. Sectioning of the surgical specimen revealed a firm, grey-white lesion with irregular margins, measuring about 2.0×1.5 cm. Histologically, the lesion consisted of tumor cells simulating hepatocytes, that were arranged in plates and pseudoglandular structures (Fig. 2). The neoplastic cells had round nuclei and a mild variation in size, hyperchromasia, and an increased nuclear:cytoplasmic ratio. Focally, bile plugs were noticed in the pseudoglandular structures of the tumor (Fig. 2). The adjacent liver parenchyma was cirrhotic. Multiple epithelioid cell granulomas, some showing a central area of caseation necrosis (Fig. 3) as well as Langhans giant cells, were found in the surrounding liver tissue. Stains for acid-fast bacilli and fungi were not performed. The final pathologic diagnosis was moderately differentiated hepatocellular carcinoma concomitant with TB. The patient's post-operative course was uneventful. Following surgery, she underwent standard chemotherapy for TB but was unfortunately lost to follow-up.

Discussion
The association of TB with carcinoma was described initially by Bayle 204 years ago [1,2]. The potential association of TB with the subsequent development of cancer has been investigated since Bayle's description [2,3]. Although Cooper in 1932 reviewed 11 cases of apparent liver cancer with TB, nine were metastatic cancers and one was found subsequently to be a carcinoma of the gallbladder [4]. To date, only two cases of primary liver cancer concomitant with TB of the liver have been reported, by Wagner in 1861 and Yano et al. in 1994, respectively (Table 1) [1,4].
Research on carcinogenesis is expanding, and the possible correlation between chronic inflammation and the development of cancer is being discerned. In this context, a history of tuberculous infection has been examined as a risk factor for the development of cancer. Collation of the available evidence has led to the establishment of three different types of association of TB and malignant disease: (1) The development of cancer against a background of previous tuberculous infection; (2) the concurrent existence of TB and malignant disease in the same patient(s) or clinical specimen(s); and (3) the diagnostic challenges arising from the multi-faceted presentations of these two disorders [4]. In general, chronic inflammatory conditions are believed to create the appropriate microenvironment for the development of neoplasia through a number of mechanisms. Examples of this include the association of gastro-esophageal reflux disease with esophageal cancer, atrophic gastritis with stomach cancer, and inflammatory bowel diseases with colon cancer. In addition, chronic infectious diseases, such as hepatitis B and C, Helicobacter pylori infection, and schistosomiasis are well-recognized as pre-malignant conditions [5].
In this context, mycobacterial infections may escape the host's cellular response and thereby establish chronic inflammation [6]. There is ample experimental evidence that Mycobacterium tuberculosis is capable of inducing damage to deoxyribonucleic acid (DNA) [7–9]. Specifically, various mycobacterial cell-wall components may induce the production of nitric oxide and reactive oxygen species [10]. Moreover, both nitrative and oxidative damage to DNA have been implicated in inflammation-related carcinogenesis [11]. Recent data also show that M. tuberculosis may enhance the synthesis of Bcl-2, which could lead to increased anti-apoptotic activity [12,13]. The combination of direct damage to DNA, inhibition of apoptosis, and the perpetuation of chronic inflammation may enhance the mutagenesis of progeny cells, and these effects, coupled with enhanced angiogenesis, may lead to a microenvironment highly conducive to neoplasia [4]. However, some authors suggest that in most cases the coexistence of TB and malignant neoplasms may be explained by chance alone, because of the common occurrence of both disorders [4]. Furthermore, TB must be distinguished from a sarcoid-like reaction. In patients without any symptoms of systemic sarcoidosis, non-caseating epithelioid cell granulomas may occur in lymph nodes draining a region housing a malignant tumor, in the tumor itself and even in non-regional tissues. However, in contrast to TB, no caseating necrosis is found in sarcoid-like reactions.
In summary, we have here reported a case of hepatocellular carcinoma concomitant with hepatic TB, together with radiologic and pathologic findings in this case. It is possible that the association of hepatocellular carcinoma and TB in this case was merely a coincidence. Further research is required to determine whether a tuberculous infection, as with various other chronic infectious and inflammatory conditions, may facilitate carcinogenesis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.