
Abstract
Abstract
Background
: In 2010, the Ventral Hernia Working Group (VHWG) published a grading system to assess the risk of surgical site complications in patients undergoing ventral hernia repair. This study evaluated the predictive value of the VHWG classification for the surgical outcomes of laparoscopic ventral hernia repair (LVHR) and identified independent factors associated with surgical site infection (SSI) and surgical site occurrence (SSO).
Methods
: A retrospective review was performed of all patients who underwent LVHR over a 10-year period at two institutions. The U.S. Centers for Disease Control and Prevention definition of SSI and the VHWG definition of SSO were used. Univariable analysis was performed using the Student t-test, analysis of variance, chi-square test, or Fisher exact test, as appropriate. Multivariable analysis was used to identify independent factors associated with SSI and SSO.
Results
: Differences in American Society of Anesthesiologists class, body mass index, diabetes mellitus, chronic obstructive pulmonary disease, tobacco use, hernia type, prior abdominal surgery, prior ventral hernia repair, hernia size, and total infections were identified by grade. There was no difference in SSI or SSO by grade. Multivariable analysis revealed institution and number of prior abdominal operations to be associated with SSI. Institution, prostate disease, and prior ventral hernia repair were associated with SSO.
Conclusions
: The VHWG classification was unable to predict SSI and SSO and may not be applicable in LVHR. This study identified independent factors associated with SSI and SSO in LVHR. Although further study is warranted to validate these results, the factors presented may be a useful tool to stratify patient risk of SSI and SSO with LVHR.
V
In 2010, the Ventral Hernia Working Group (VHWG) published a grading system to stratify patients for assessment of the risk of surgical site complications. The paper also outlined a generalized approach and technical considerations for the repair of incisional ventral hernias, including the growing role of biologic repair materials [5]. Along with SSI, the VHWG defined surgical site occurrence (SSO) as an endpoint. Surgical site occurrence includes SSI, seroma, wound dehiscence, and enterocutaneous fistulae at the site of the hernia repair. Patients are risk stratified on the basis of previous surgery, infections, and co-morbidities. Patients rated grade I have a low risk of complications and no history of wound infection. Patients rated grade II are considered to have co-morbidity and include current smokers, those with diabetes mellitus, obese patients, immunosuppressed patients, and patients with chronic obstructive pulmonary disease (COPD). Patients rated grade III are classified as potentially contaminated and have a history of surgical site infection, current ostomy, or violation of the gastrointestinal tract. Patients rated grade IV are classified as infected and have an infected mesh or dehiscence.
The VHWG authors note that the classification “focuses primarily on the open repair of incisional ventral hernia. However, the growing popularity of laparoscopic techniques deserves discussion with relation to the grading system and recommendations of the VHWG” [5]. The purpose of this study was to evaluate the predictive value of the VHWG grade for early and late outcomes of LVHR. In addition, we identified independent predictors of SSI and SSO. We hypothesized that the VHWG grading system is predictive of SSI and SSO after LVHR.
Patients and Methods
The Institutional Review Board approved the experimental protocol through Baylor College of Medicine and affiliated hospitals. This study was exempt from the need for patient informed consent.
We retrospectively reviewed 201 consecutive patients who underwent elective LVHR with prosthetic mesh placement at two institutions from January 2000 to December 2010. The institutions were a Veterans Affairs Medical Center (VAMC) and a community hospital.
All patients received appropriate preoperative antibiotics. The LVHR was performed in a manner similar to the method described by the American College of Surgeons [6]. A mesh prosthesis was placed intraperitoneally behind the abdominal wall, with 3–6 cm of overlap of the abdominal wall from the borders of the hernia defect. The mesh was secured circumferentially with transfascial sutures and with tacks applied every centimeter along the mesh border. The type of mesh was chosen by the attending surgeon. There were no procedures done concomitantly with the LVHR in any of the cases. Any case in which bowel injury was incurred was converted to an open procedure and thus was not included in our analysis.
Patient data, including demographics, co-morbidities, clinical history, imaging data, and surgical outcomes, were reviewed. Each patient was then assigned a grade according to the VHWG system. Alcohol abuse was defined as >2 drinks per day. Surgical site infection was defined by the recommendations of the U.S. Centers for Disease Control and Prevention (CDC) and included infections as late as one year post-operatively [7]. Surgical site occurrence was defined by the VHWG as any surgical site complication, including “infection, seroma, wound dehiscence, and the formation of enterocutaneous fistulae” [5]. Seroma was defined as a clinical or radiographic bulge that was not a hernia recurrence or eventration by clinical examination or imaging. Eventration was defined as a patient complaint of a bulge without evidence of hernia recurrence or seroma and was assessed by computed tomography (CT) and clinical examination. Mesh eventration was the protrusion of the mesh beyond the anterior plane of the abdominal wall fascia. Tissue eventration was extension of retained preperitoneal fat or hernia sac beyond the boundaries of the anterior abdominal wall fascia. Ileus was defined as the absence of gastrointestinal function by post-operative day three or loss of gastrointestinal function not attributable to obstruction. Small bowel obstruction was defined as mechanical obstruction documented by clinical assessment or CT. Recurrence was assessed both clinically and via CT. Of our 201 patients, 125 (62%) had post-operative CT scans performed.
Patient characteristics were assessed using the Student t-test, analysis of variance, χ2 test, or Fisher exact test, depending on whether the variables were continuous or categorical. Any p value≤0.05 was considered to be statistically significant. Elements with missing data were omitted from the descriptive analysis. Univariable logistic regression models were built to estimate the odds of SSI, SSO, and VHWG grade when considering the effect of each variable separately [8]; however, we report only the univariable results of VHWG grade as the dependent variable.
Multivariable logistic regression models were built to assess the effect of a given predictor on both SSI and SSO while controlling for other predictors in the model. To identify the most significant predictors, VHWG grade and all variables with a p value<0.20 in the initial assessment of patient characteristics were put into the multivariable model and then reduced in a stepwise manner to identify the best fit according to the Akaike information criterion [9]. Diagnostics of the multivariable logistic regression model were assessed and validation was performed using a 10-fold cross-validation. All statistical analysis was performed on the software R (Vienna, Austria) [10].
Results
According to the VHWG grading system, 28 patients (14%) were grade I, 146 (72%) were grade II, and 27 (13%) were grade III. None of our patients was classified as grade IV. By univariable analysis, patient demographics were similar for the three groups. Because of the nature of the VHWG grading system, there were statistically significant differences in body mass index (BMI), COPD, diabetes mellitus, and current tobacco use among the three groups. The American Society of Anesthesiologists (ASA) stratification was significantly different among the grades. There was no difference in the prevalence of coronary disease, prostate disease, or alcohol abuse among the groups. We noted significant differences in the number of primary hernias, prior ventral hernia repairs, and previous abdominal operations among grades. Hernia size (overall area) was significantly different in the three groups, with greater dimensions being associated with higher grade. The type of mesh used was not significantly different among groups (Tables 1 and 2).
ASA=American Society of Anesthesiologists; VAMC=Veterans Affairs Medical Center.
Material in boldface indicates complications showing statistically significant differences between groups.
Tables 3 and 4 report the early and late outcomes, respectively. There was no significant difference in follow-up for the three groups (grade I, 24 mos; grade II, 24 mos; grade III, 20 mos). There was a significant difference in the prevalence of total infections in the 30-day post-operative period. However, there were no significant differences among the three groups regarding post-operative SSI or SSO, and there were no significant differences in any other outcomes for the three groups.
Material in boldface indicates complications showing statistically significant differences between groups.
LOS=length of stay; SSI=surgical site infection; SSO=surgical site occurrence.
SBO=small bowel obstruction.
By multivariable analysis, we noted that the only predictors of SSI were the institution where the operation was performed and the number of prior abdominal operations (Table 5). Institution, prostate disease, and a history of ventral hernia repair were predictors of SSO (Table 6). Other patient and operative factors, including mesh type, were not significant in predicting SSI and SSO. Interestingly, VHWG grade was not found to be a predictor of SSI or SSO. After the model was fully reduced, VHWG grade was returned to the model; however, there was no correlation between grade and SSI/SSO.
Material in boldface indicates complications showing statistically significant differences between groups.
Material in boldface indicates complications showing statistically significant differences between groups. K-fold cross validation 0.18.
Discussion
Ventral hernias are a common source of morbidity in the United States. In recent years, laparoscopy has emerged as a potentially less morbid approach to repair; however, although the risk is lower than that of open repair, SSI and SSO continue to be significant complications. The VHWG classification was proposed as a tool to predict SSI and SSO in ventral hernias, regardless of the type of repair. Although the VHWG focused primarily on open incisional repairs, the authors noted that laparoscopic repairs “deserve discussion in relation to the grading system”5 [5].
Our study found an overwhelming majority of patients were classified as grade II (72%), with an equal distribution between grades I (14%) and III (13%). Demographic and historic differences among the grades noted on univariable analysis were not surprising. Patients undergoing ventral hernia repair are more likely to have a co-morbidity, making VHWG grade I patients inherently less common. Grade III patients have an ostomy (n=1 in our population; this patient underwent laparoscopic parastomal hernia repair), prior SSI (n=26 in our population), or a violation of the gastrointestinal tract. In all patients with violation of the gastrointestinal tract, the operation was converted to an open procedure, and the patient was excluded from our analysis. Grade IV patients (dehiscence related to infection, or infected mesh) are not suitable for laparoscopic repair. The significant differences in BMI, diabetes mellitus, COPD, and tobacco use were expected, as those factors are inclusion criteria for grade II. The ASA class, which takes into account patient co-morbidities and functional status, also showed the expected significant difference among the grades. The difference among the groups regarding hernia size mirror the existing literature; patients with prior abdominal operations, including prior ventral hernia repairs or incisional hernias, are more likely to have recurrent and larger hernias [3,11,12,].
Surgical site infection is a commonly studied outcome in ventral hernia repairs. Although the prevalence of SSI after LVHR differs widely in various reports, most studies comparing LVHR with open repair demonstrate a decrease in SSI [2,4,13–21]. The differences in the reported prevalence of SSI after LVHR may be related to different risks of the patient populations studied, the number of primary hernias within the cohort, study methodology, the post-operative period used to describe SSI, and the definitions applied. Many studies fail to utilize the CDC definition of SSI and instead use various other definitions [2–4,22,23]. Additionally, much of the literature on this subject addresses only open repairs or combines open repair and LVHR into one group [24,25]. Obesity [26], COPD [22,27,28], diabetes mellitus [29], tobacco use [22,24], and incision class [22] are independent risk factors for SSI in open hernia repair. Despite their risk factors for SSI, patients rated grades II and III do not have strict contraindications to LVHR; the decision to perform open or laparoscopic repair is weighed against the individual risk for infection and other co-morbidities. Patients rated grade IV (active mesh infection or dehiscence) are not suitable for laparoscopic repair, excluding them from any studies concerning the VHWG classification and LVHR [5].
We noted that the institution and the number of prior abdominal operations were independent predictors of SSI after LVHR (Fig. 1). Our VAMC population was at higher risk of SSI, a finding supported by other recent studies [30]. Compared with our community hospital, the patients at the VAMC were more likely to be male, older, have more co-morbidities, and to be classified in a higher VHWG grade (p=0.04). This difference in patient population, particularly the greater prevalence of co-morbidities, likely contributed to the predictive value of institution as a variable for SSI. As such, institution may function as a surrogate marker. However, patient population is only one factor when looking at institutional differences. Such differences affect surgical outcomes in multiple ways, including operative personnel and protocols, staffing patterns, the presence of trainees, and microbiology patterns [31,32]. Thus, differences between institutions may not be explained by differences in patient population alone. Further study is needed to elucidate the importance and contribution of these differences to SSI.
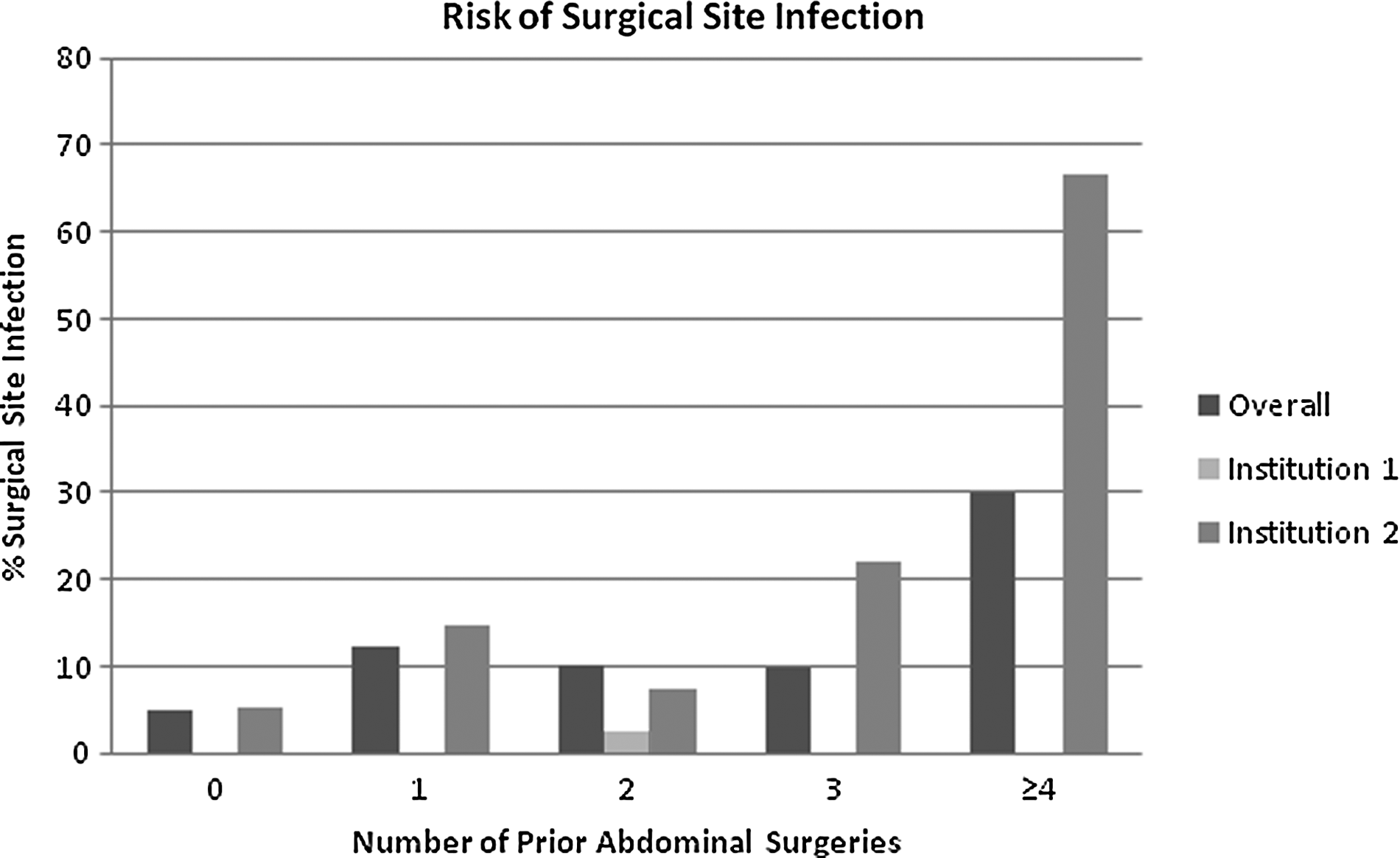
Prior abdominal operations and institutional differences increase the risk of surgical site infection.
In addition to institution, the number of prior abdominal operations was an independent predictor of SSI in our patients. Those with a history of such operations are likely to have incisional hernias that are larger and more complex and are associated more often with SSI in multiple studies [3,33–35]. The non-significant trend toward more SSIs by grade may be an indirect reflection of the number of prior abdominal operations.
Surgical site occurrence is a novel method to define site complications. There have been no studies of the prevalence and predictors of SSO with LVHR. Second to SSI, seroma is the most studied SSO with LVHR. However, seroma has not been well defined in this population, and a review of the literature shows a 0.5%–100% occurrence of post-operative seroma in patients undergoing LVHR [4,13–16,36–39]. We included all patients with documented seroma. A consensus definition and proper documentation/reporting of seroma would improve greatly the quality of data available in LVHR patients.
In our multivariable analysis, SSO was independently predicted by institution, prostate disease, and prior ventral hernia repair (Fig. 2). As discussed previously, institutional differences are multifaceted and extend beyond differences in patient populations. Prior ventral hernia repair implies that the current problem is a recurrent incisional hernia. The literature supports the view that recurrent ventral hernias tend to be larger and complex [3,11,12] and associated with more complications, including SSO [3,12,25,28,33–35]. Prostate disease has not been studied extensively as an independent predictor of complications. However, a randomized controlled trial showed that prostate disease is associated with hernia recurrence and incisional hernias [40]. In addition, prostate disease is a uniquely male problem, and this may be a further representation of highly male-dominated institutions such as the VAMC.

Prior ventral hernia repair and institutional differences increase the risk of surgical site occurrence.
We also evaluated the VHWG classification in relation to long-term outcomes. Many studies claim similar recurrence rates for LVHR and open repair [2,17], whereas others state that LVHR has a lower recurrence rate [18]. Although the VHWG system was not conceived to evaluate recurrence, we felt that it was an important secondary endpoint. We were unable to show any predictive value of the VHWG classification regarding recurrence.
On the basis of these findings, it is unclear whether the VHWG classification offers any further insight into patient outcomes after LVHR. Many of the inclusion criteria for grade II are risk factors for ventral hernias and postoperative complications. Thus, we predict that the application of the VHWG grading system to most patient populations studied for ventral hernia repair will result in a predominantly grade II grouping. Despite identifying risk factors for SSI and SSO in ventral hernia repair in the literature, the VHWG does not differentiate between the relative risks of each of the inclusion criteria. The grading system does not differentiate between an otherwise healthy patient who has a 0.5 pack-year smoking history and an obese patient with COPD, poorly controlled diabetes, and a 50+ pack-year smoking history. These patients are considered equally “co-morbid.” Better stratification of the relative risks of each of the grading inclusion criteria may be useful in predicting the risk of SSI and SSO.
There are a number of limitations to our study. First, it is limited by its retrospective nature. Selection bias, surgeon preferences, and identification of outcomes by a chart review are all confounding factors. Second, on univariable analysis, there was a trend toward more SSI and SSO with increasing VHWG grade. However, on multivariable analysis, the VHWG classification was not predictive of SSI or SSO. In our patient population, the effect size for the VHWG was 0.12 for SSI and 0.11 for SSO, assuming an α of 0.05 and a 1-β of 0.80. An effect size of ≥0.21 would have been necessary to demonstrate an association between VHWG grades on SSI or SSO in this study. Our sample size of 201 is among the larger LVHR cohorts in the literature, but an even larger patient population may be able to define better the role of the VHWG classification. Additionally, the majority of our patients were classified as grade II, with significantly smaller, but equal, cohorts in grades I and III. Although this may be a reflection of the VHWG stratification system, the lack of balanced cohorts is a limitation of our study. Given the prevalence of SSI and SSO, a 646-patient cohort would have been necessary to demonstrate a statistical correlation between the VHWG grade and SSI (or an 809-patient cohort for SSO) on univariable analysis. However, despite potential univariable significance, the VHWG classification still may not be significant on multivariable analysis. Third, the majority of our data came from VAMC patients, who tend to be older and male and to have multiple co-morbidities. Application of the results of this study to other patient populations should be done with caution.
Conclusion
The VHWG classification, proposed as a tool to predict SSI and SSO, may not be applicable in LVHR. Although the system appropriately identifies preoperative risk factors for SSI and SSO based on the literature, it does not further stratify the relative importance of those risk factors and therefore did not provide any predictive insight in our patient population. On both univariable and multivariable analysis, the VHWG grading system was not predictive of SSI or SSO. Instead, we noted that institution and the number of prior abdominal operations identified patients at greater risk for SSI. Institution, prostate disease, and a history of ventral hernia repair were found to be independent risk factors for SSO in our study population. Further study, with larger cohorts, is needed to validate these results.
Footnotes
Author Disclosure Statement
R.B., S.A.C., S.C.H., and D.H.B. declare no competing financial interests. M.K.L. has held research grants from Lifecell and unrestricted education grants from Lifecell, KCI, and Acell.