
Abstract
Background:
No conclusive results on the efficacy and timing of open abdomen (OA) are available, particularly in the setting of intra-abdominal infections. We analyzed outcomes and risk factors retrospectively in a large series of patients managed with an OA during the past 20 y in an effort to clarify this issue.
Methods:
We reviewed the records of 133 patients who underwent treatment with an OA, considering factors related to patient, disease, medical management, and surgical treatment. The end points of the bi-variable analysis were 1-y mortality, calculated from the time of an initial OA procedure, and definitive fascial closure.
Results:
Most patients (112/133) managed with an OA had one of several types of peritonitis. Many patients had severe clinical conditions (mean Acute Physiology and Chronic Health Evaluation [APACHE] II score was almost 9 points for the study population). With regard to surgical management, the mean (+SD) number of abdominal revisions was 5.9+9.3 during a mean duration of treatment with an OA of 14.3+11.6 d. The overall mortality in the study was 26% (35/133). Bi-variable analysis revealed factors associated with overall mortality to be age, renal and respiratory co-morbidities, edema on an initial chest radiograph, blood pressure, blood glucose and creatinine concentrations; and APACHE II score. The rate of definitive fascial closure was 75% (100/133). Factors associated negatively with fascial closure were respiratory co-morbidity, edema on a first chest radiograph, post-operative mesenteric ischemia as an indication for OA, blood glucose and creatinine concentrations, and duration of an OA.
Conclusions:
Patients' pre-operative clinical status influences strongly their response to surgical treatment. The management of OA does not affect adversely the survival of patients with intra-abdominal infections, but factors related to the management of OA (duration of OA) seem to affect the possibility of definitive fascial closure.
T
Use of the OA is indicated in patients with diffuse intra-abdominal infection or severe abdominal trauma (requiring surgery for damage control), massive intestinal distention, and defects in the abdominal wall, as well as those with acute mesenteric ischemia or necrotizing pancreatitis [1]. In practical terms, the OA might be useful in every situation in which a hostile abdomen requires extended treatment [2]. Additionally, the OA is the solution to the most dangerous of all conditions affecting the abdomen, abdominal compartment syndrome, in which it has been shown to decrease mortality markedly [3–10].
In the late nineteen sixties, after the introduction of the OA in the context of battlefield surgery [11], the decision to leave the abdomen in an open state was abandoned [12]. Yet the OA has occasionally been used in general surgery, and in this context the decision by several surgeons to persevere in its use contributed to the development and definition of the concept of “damage-control” surgery [13].
The approach suggested in damage control surgery, used originally in trauma surgery, was subsequently extended to general abdominal surgery in every setting in which a “second look” at the abdominal cavity was needed [14,15]. Lately, many efforts have been undertaken to define and outline recommendations for management of the OA [16–18], but definitive evidence for an optimal means of its management is still needed [1,19].
Currently, no conclusive results for this have been reached, because controlled randomized clinical trials of use of the OA are difficult to conduct [20], and today, more than a decade after the OA technique began to be used widely [19], its value is still difficult to assess and uncertainty remains about its efficacy. Despite progress following the introduction of vacuum-assisted temporary closure of the abdominal wall [1,22,23], the mortality associated with OA remains high, with many co-morbidities related apparently to the management and timing of delayed fascial closure [24]. At present, the literature contains varying proposals for whether or not to close the abdominal cavity after a laparotomy, with some preferring the use of an OA technique and others preferring repeat laparotomy if circumstances demand this [21].
Given these realities, two well-founded questions remain to be answered [20]: 1) Is management with an OA beneficial (or even harmful)?; and 2) when should an OA be discontinued? In the study reported here we analyzed retrospectively the outcomes and risk factors for a large series of patients treated with an OA during the past 20 y, with the goal of helping to answer these two questions, particularly in the setting of intra-abdominal infections [25].
Patients and Methods
We reviewed the records of 133 patients who underwent treatment with an OA between January 1990 and February 2012, considering the following factors:
1. Patient-related factors, consisting of age, gender, weight, height, co-morbidities (hepatic, renal, respiratory, and cardiovascular, and diabetic dysfunction); and prior abdominal surgery. 2. Disease-related factors (evaluated at admission or immediately before the first OA procedure), and comprising the indication for use of the OA technique, heart rate, heart rhythm, blood pressure, temperature, blood-test results (pH and hemoglobin in g/dL), hematocrit, white blood cell and platelet counts (per mm3), international normalized ratio (INR), activated partial thromboplastin time (aPTT), glucose, electrolytes (Na+, K+, Cl-, and Ca2+, in mEq/L), creatinine, aspartate aminotransferase (AST) (in IU/L), alanine aminotransferase (ALT) (in IU/L), bilirubin, findings on first chest radiographs (pleural effusion or edema), findings on first computed tomographic and ultrasound scans of the abdomen (abscess or fluid collection), and Acute Physiology and Chronic Health Evaluation (APACHE II) score. 3. Medical treatment-related factors (evaluated at admission or immediately before the first OA procedure), comprising use of a nasogastric tube, oxygen support, red blood cell (RBC) transfusion, medical treatment with opioids or antibiotics, and medical inotropic support. 4. Surgical treatment-related factors consistying of duration of surgery, intra-operative details (findings, resections, anastomoses, stomas), intra-operative RBC transfusion, duration of OA, number of abdominal revisions, and time interval between consecutive revisions.
Our analysis did not include measurements of intra-abdominal pressure or any parameter assessed during intensive care. The end points of the analysis were 1-y mortality calculated from the first OA procedure, and definitive fascial closure.
Treatment
The OA technique was done by several surgeons in our institution's surgical division in accord with our conventional approach to a hostile abdomen [26]. Selection of the methods used for temporary closure during the long period of the study was based on devices available for this (Bogotà bag until 2007; Bogotà bag or vacuum-assisted therapy from 2007 to the present) [26]. Surgical revision of the abdominal cavity was always done in the operating room (as recommended in the safety guidelines for our intensive care unit in case of intra-abdominal infection) at 24–48-h intervals according to the clinical condition of the patient. Surgical revision of the abdominal cavity included: 1) Extended cleaning and debridement of any peritoneal surface; and 2) all maneuvers useful for a complete recovery of organ function (including, when possible, anastomosis or, alternatively, ostomy). All patients remained on mechanical ventilation through an orotracheal tube or tracheostomy, in accord with the findings on evaluation by the anesthesiologist. At the end of the period of OA, definitive fascial closure was done only in patients with a preserved abdominal wall and after accurate source control was achieved. In patients who did not have a definitive fascial suture, closure was obtained by vacuum-assisted therapy and, before 2007, through the use of skin flaps alone.
Statistical analysis
Results were expressed as percentages, median (range), or mean±SD. Data were analyzed with non-parametric tests (Fisher exact test or the Mann–Whitney U test, as appropriate). The level of significance was set at p<0.05 (two-sided). Statistical analysis was done with SPSS software (SPSS, Chicago, IL) for Windows (Microsoft, Redmond, WA).
Results
Patient- and disease-related factors
The study data base consisted of 74 men and 59 women with a mean age of 58.5±16.4 y. The OA approach was indicated for 91 (68%) of the patients at the time of their first surgical procedure; in 42 (32%) cases, OA was chosen as an option for complications of surgery after surgery had been completed or after an unresolved abdominal emergency. The indications for management with an OA, together with the pre-operative clinical findings in the respective patients, are shown in Table 1.
ALT=alanine aminotransferase; APACHE=Acute Physiology and Chronic Health Evaluation; aPTT=activated partial thromboplastin time; AST=aspartate aminotransferase; CT=computed tomography; Hb=hemoglobin; Hct=hematocrit; INR=international normalized ratio; OA=open abdomen; US=ultrasound; WBC=white blood cell count.
Treatment-related factors
The details of the medical and surgical treatment of all of the patients in the study are shown in Table 2. The collection of clinical parameters revealed that many patients presents severe clinical conditions, as indicated by a mean APACHE II score of almost 9 points for the study population (Table 1). With regard to surgical management, the mean number of abdominal revisions was 5.9±9.3 (6.3±11.9 in the group with abdominal trauma), with a mean overall duration of management with an OA of 14.3±11.6 d (range 1–80 d), and of 11.8±21.2 d (range 1–57 d) in the trauma group.
OA=open abdomen.
End points
The overall mortality in the study population was 26% (35/133), and that in the trauma group was 19% (4/21) (p>0.05 vs. patients with intra-abdominal infections). Bi-variable analysis (Table 3) revealed that factors associated with overall mortality were age, renal and respiratory co-morbidities, edema on a first chest radiograph, blood pressure, blood glucose and creatinine levels, and APACHE II score. The percent rate of definitive fascial closure in the study population 75% (100/133), and that in the trauma group was 86% (18/21) (p>0.05 vs. patients with intra-abdominal infections). Factors associated negatively with fascial closure in the non-parametric statistical tests used in the study (Table 4) were respiratory co-morbidity, edema in a first chest radiograph, and post-operative mesenteric ischemia as indications for OA; blood glucose and creatinine concentrations; and duration of OA (Figure 1). Statistical comparison of the effects of the different temporary closure devices used on the study patients was unreliable because after 2007, most of the patients who had an OA were treated with both a Bogotà bag and vacuum-assisted therapy in different phases of the same treatment.
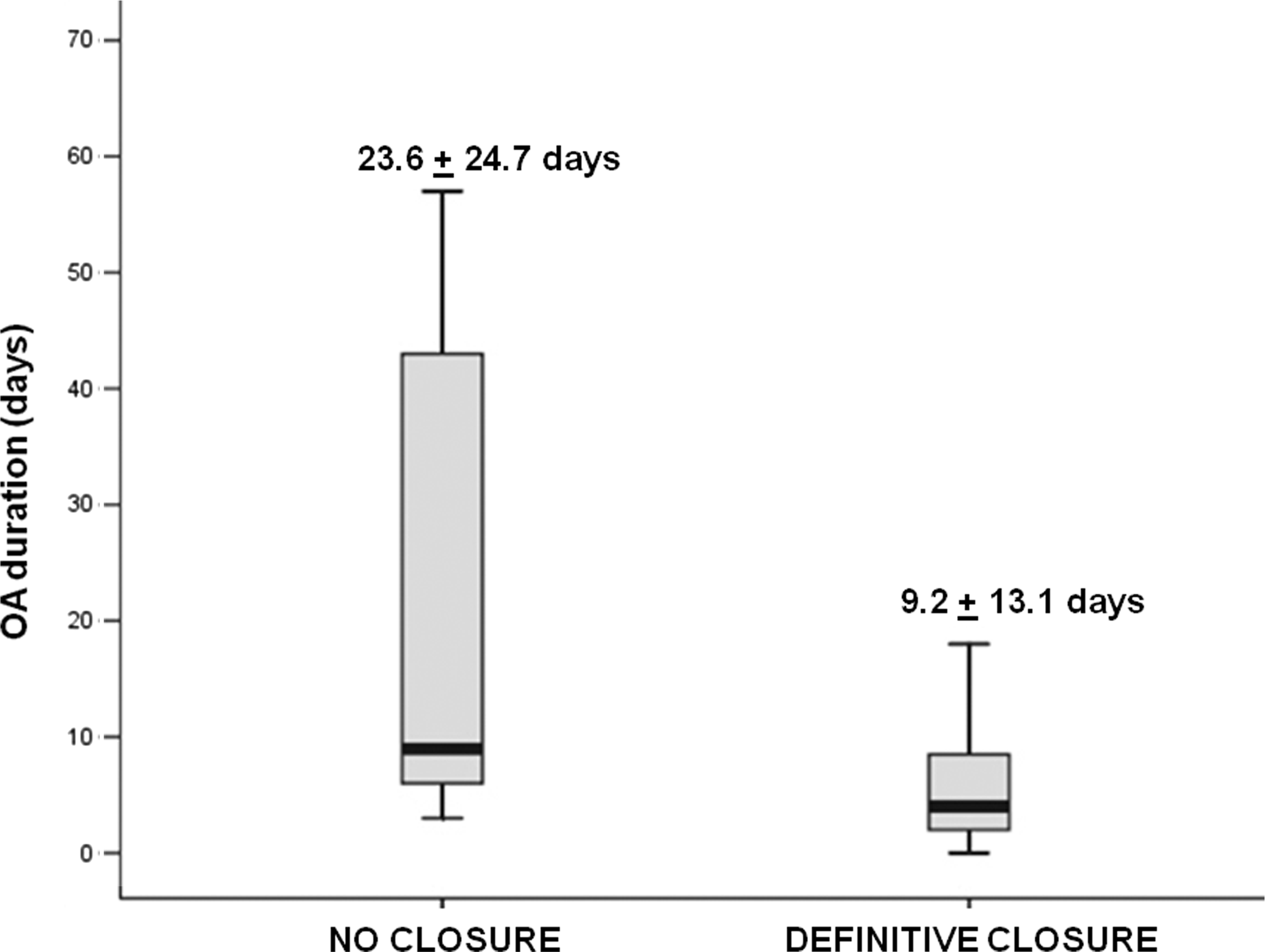
Box plots of the duration of an open abdomen in the study population according to the criterion of definitive fascial closure.
APACHE=Acute Physiology and Chronic Health Evaluation
OA=open abdomen.
Discussion
The focus of a discussion of OA should be the patient rather than the abdomen, including factors such as nutrition, ambulation, and control of infection and inflammation as relevant to the patient's prognosis. Accordingly, the patient's general clinical condition plays an important role in the evaluation of a patient [25].
Data in the literature refer largely to the use of OA after trauma. In our series, however, major trauma was the indication for OA in only 16% of the study population (21/133), with most instances of the use of OA being related to several types of peritonitis (Table 1). Although we found no statistically significant differences in the outcome rates for patients having OA because of trauma and those having it because of intra-abdominal infection, in order to attempt to clarify the real benefits and the ideal duration of OA management, a comparison of our outcome data with that in the literature is quite difficult, although still feasible, particularly with regard to mortality and time to fascial closure.
In our study, the overall 1-y mortality (calculated from the first OA procedure) was 26%. This figure refers to all cases in which an OA was used, independently of the specific indication for the patient's surgery. Schein et al. [27] prospectively studied a group of 52 patients who underwent “planned relaparotomies” to treat critical intra-abdominal infections. The overall mortality in their study reached 44%. Christou et al. [28] also conducted a prospective study, in which they analyzed 239 patients with abdominal sepsis in a non-randomized trial of management techniques and outcome in severe peritonitis. They observed an overall mortality of 32%, and through logistic regression analysis found that several criteria that were not strictly surgical (a high APACHE II score, low serum albumin concentration, and high New York Heart Association status for cardiac function) were significantly associated with postoperative death. Consistent with these results was the finding by Bosscha et al. [29] of an overall in-hospital mortality of 42% in a group of 67 patients who underwent open management of the abdomen and planned reoperation for severe peritonitis following perforation or disruption of the gastrointestinal tract. Koperna et al. [30], in a retrospective case-control study of 523 patients with severe peritonitis, in which they focused on 105 patients who underwent re-laparotomy for abdominal sepsis persisting after surgery, found a post-operative mortality of 54.5% after planned re-laparotomy as opposed to a mortality of 50.6% after re-laparotomy on demand. Estimation of these patients' risk was based on their pre-operative clinical conditions. Similar results and considerations with regard to mortality have been reported in more recent series [31,32] and in a Dutch randomized trial in which planned re-laparotomy was compared with re-laparotomy on demand in more than two hundred patients with severe peritonitis [33].
Therefore, both our results and the data reported in the literature strongly suggest that in the patient population for whom the OA technique is used (and particularly those with intra-abdominal infections), with its high mortality, clinical factors play an important role in predicting outcome. Co-morbidities and clinical status (evaluated at admission or in the immediate pre-operative period) strongly influence a patient's response to surgical treatment. Of interest was the finding in our study that keeping the abdomen open does not affect survival. In fact, treatment-related variables did not affect the 1-y mortality in our study, which was determined only by patient- and disease-related factors (Table 3).
On the other hand, factors related to the management of an OA appear to affect the possibility of definitive fascial closure (Table 4). Definitive closure is a crucial issue often discussed in the literature in the context of evaluation of the positive and negative factors in the decision to leave an abdomen open. Fascial retraction is a frequent complication of the OA technique that can necessitate complex and expensive solutions. The time for definitive closure of the abdomen is determined by the (changing) balance between the clinical judgement of the surgeon and the changes in the patient's clinical (and abdominal) condition. The literature does not permit the establishment of any clear rule for increasing the rate of definitive fascial closure beyond the use of a specific temporary closure device. It is known that the process of wound closure should begin at the first return to the operating room of a patient with an OA [1]; the goal of the first surgical revision of an OA (planned for 24–48 h after the patient's index operation) is to check the abdominal viscera, remove packing, and proceed to reconstruction (e.g., creation of anastomoses or stomae), as well as to begin abdominal closure or, more often, to perform a temporary closure with a view to definitive closure.
In our study, definitive fascial closure was achieved in 100 of 133 patients (75%). This result was achieved independently of the indication for use of an OA or the system used for temporary closure of an OA in a particular patient. Nevertheless, the time of closure (duration of OA) seemed to be the critical factor for the definitive closure of an OA. A shorter duration of OA was associated significantly with a high probability of definitive closure (p<0.032), and this probability increased when closure occurred within 9 d after an initial OA procedure (Fig. 1). The current literature indicates that both the mean time to closure of an OA and the patient's outcome extend over the wide range of 3–46 d) [34,35].
In our study (mean time to closure: 14 d), we observed two extreme cases in which an OA was continued for 80 d, both of which had a successful outcome. This finding does not have any scientific value, but indicates that as a technique, an OA is by itself inadequate for codification or classification.
Nonetheless, several authors have provided interesting contributions toward understanding when to stop treatment with an OA in cases intra-abdominal infection. Wittman et al. [36] stated that planned laparotomies have to be continued until the “abdomen is macroscopically clean.” Van Goor et al. [37] suggested microscopic bacterial cultural criteria for optimizing the timing of abdominal closure for patients with severe peritonitis, but these criteria are not easy to apply. If, therefore, a consistent set of criteria for the closure of an OA cannot be derived from surgical criteria alone [25], an established maximum duration of OA may be a simpler criterion for use in clinical practice.
According to the criteria set forth by Schein [20], our study was limited by its retrospective nature. Additionally, the study population was inhomogeneous and its data were difficult to analyze. Furthermore, we did not consider in our patient series any intensive care parameter (including intra-abdominal pressure). However, notwithstanding these potential limitations of our study, our decision to evaluate only simple clinical details improves the external validity of our conclusions.
Footnotes
Author Disclosure Statement
The authors report no conflicts of interest.