
Abstract
Abstract
Background:
Migration from Latin American countries has increased the number of cases of chagasic megacolon in Western countries. Megacolon is a late complication of Chagas disease, resulting from irreversible destruction of the intramural intestinal nervous system with extensive loss of neurons, ganglionitis, and myositis at the sites of the myenteric and submucosal plexuses. Several surgical procedures involving partial or total resection of the dilated colon have been proposed for treating chagasic megacolon, but intra-operative evaluation of neuronal degeneration in the residual colon has not been commonly done.
Methods:
Case report and literature review.
Case Report:
We describe a case of chagasic megacolon treated successfully with a modified Habr-Gama technique, with the intra-operative examination of frozen sections of the residual segments of the colon for the presence of neurons.
Conclusions:
The recurrence of constipation after surgical treatment can result from the progression of chagasic neuronal degeneration in the preserved colon, and may be preventable by intra-operative evaluation of whether signs of neuronal degeneration or inflammation are absent in the anastomosed colonic tract.
C
The clinical picture of the chronic form of Chagas disease is dominated by cardiologic and gastrointestinal manifestations [4]. Even though it may involve the entire gut, Chagas disease affects primarily the esophagus and the colon, leading to megaesophagus and megacolon [5,6].
Chagasic megacolon results from irreversible damage to the intrinsic and extrinsic autonomic nervous system [7,8], characterized by degeneration and a decrease in the number of myenteric neurons and interstitial cells of Cajal, and impairments in glial cells caused by inflammatory infiltration [9]. The rectum and the sigmoid colon are the regions of the large intestine affected most frequently in chagasic megacolon. The denervation of the myenteric plexus gives leads to loss of motility and dilation of the distal colon, and presents clinically as progressive and frequently severe constipation, complicated by sigmoid volvulus and fecal impaction. This stage of Chagas disease is resistant to drug therapy, and surgery is the only possible treatment for it.
With the aim of relieving constipation and preventing complications, several techniques have been reported for the surgical treatment of chagasic megacolon, the most widely used of which is abdominal rectosigmoidectomy with immediate posterior colorectal end-to-side stapled anastomosis (the modified Duhamel–Haddad or Habr-Gama technique) [10]. We report here a case of chagasic megacolon treated surgically with the modified Habr-Gama technique and discuss whether the tactic used for treating Hirschsprung megacolon is also appropriate for chagasic megacolon.
Case Report
A 56-year-old Bolivian female had a 22-year history of Chagas disease, diagnosed at a Bolivian center on the basis of standard serologic tests for T. cruzi (detection of parasites in blood smears and IgM antibody tests). Routine laboratory tests based on hemoculture, immunologic assays for immunoglobulin G (IgG), and findings in cardiologic examinations and abdominal imaging studies were normal for 20 y, after which the patient began to experience chronic constipation. For 2 y her gastrointestinal disorder was managed with the use of laxatives and rectal enemas, but in July 2008 her symptoms worsened and she was referred to our department for surgical treatment.
Plain abdominal radiographs showed gross dilation of the colon, and particularly of the sigmoid colon, which was confirmed by barium enema studies (Fig. 1). Anorectal manometry showed impairment of the sphincteric response to rectal distension, with absence of the rectoanal inhibitory reflex (RAIR) at a volume of 200 mL of air. A prolonged colonic transit time was demonstrated, with radiopaque markers halting in the left quadrant at day 5 (Fig. 2). No cardiovascular manifestations of the patient's colonic pathology were seen with specific tests.
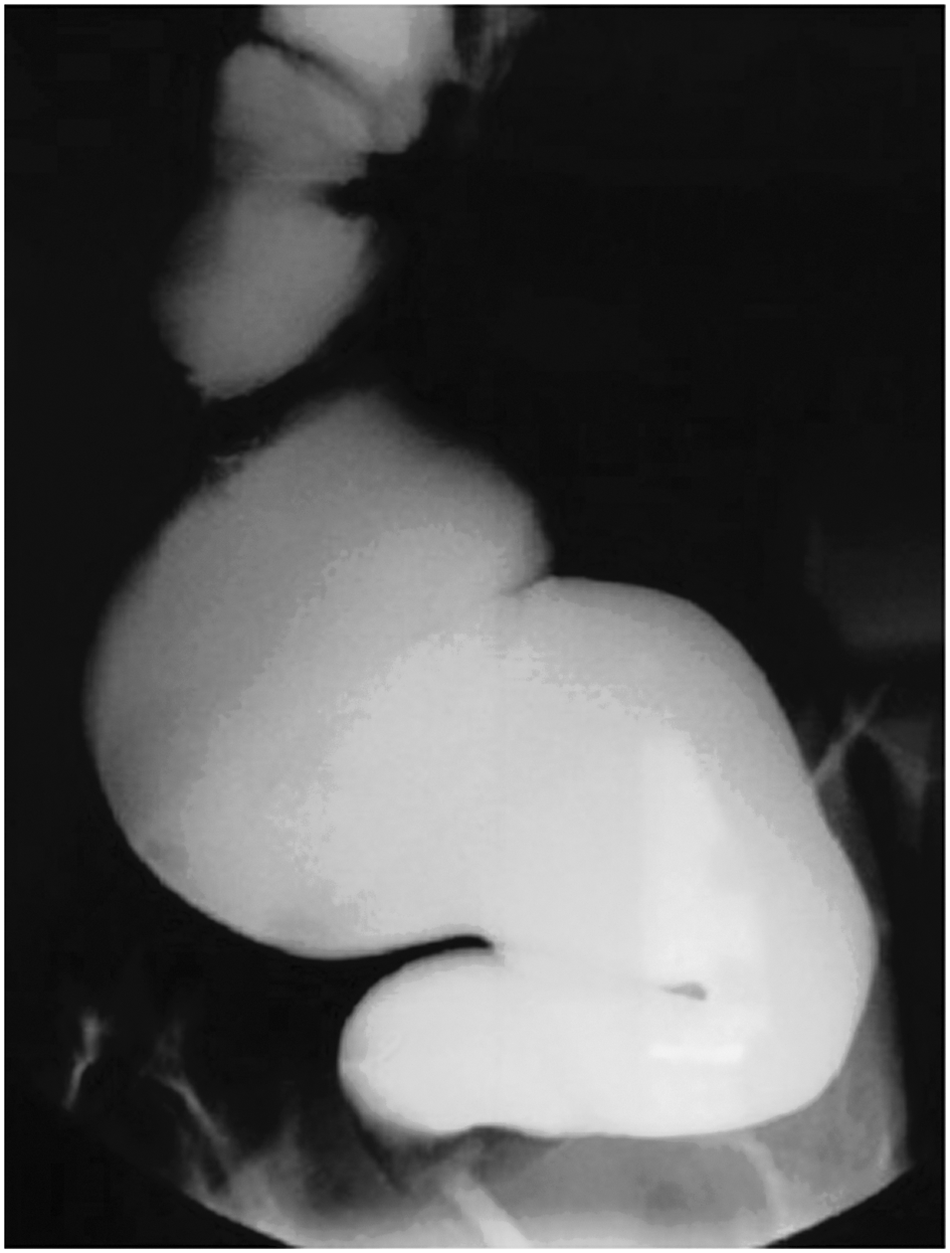
Barium enema showing grossly increased diameter of the entire sigmoid colon.
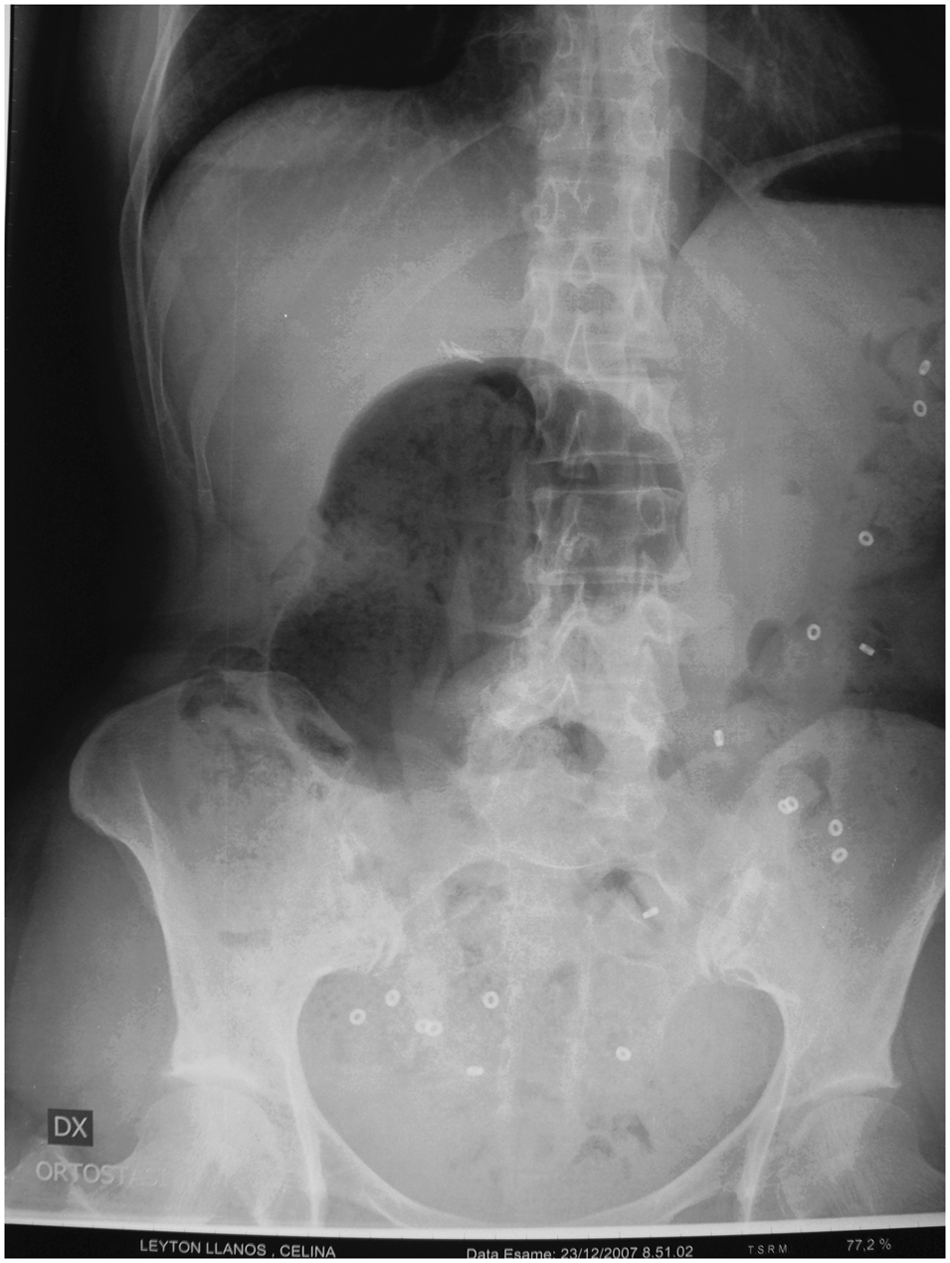
Radiograph of bowel during study of intestinal transit time, in which markers had stopped in the left quadrant at day 3.
At surgery, the patient's sigmoid colon and rectum appeared dilated. For investigation of the enteric nervous system, seromuscular biopsy specimens from the ascending, transverse, and descending colon and the rectum were stained with hematoxylin-eosin (H&E) and acetylcholinesterase (AChE) for frozen-section examination. The splenic flexure, left colon, and posterior rectal wall were mobilized as far as the level of the elevator muscles, with exposure of the anorectal junction. The rectal biopsy specimen was negative for ganglion cells, but the biopsy specimen from the descending colon revealed a normal number of ganglion cells between the muscular layers.
The Douglas pouch of the peritoneal reflections was incised and the anterior rectal wall was then mobilized for a few centimeters to transect the extraperitoneal rectum with a TA-55 stapler (United States Surgical, Norwalk, CT). An immediate posterior colorectal end-to-side stapled anastomosis between the rectum and descending colon, near the left colonic corner, was then done with a CEEA 31 stapler (United States Surgical). The anastomosis was located at the lower third of the posterior wall of the rectum, just above the anorectal ring. No diverting stoma was created. The patient's post-operative hospital stay was 10 d, during which no complications occurred. Oral feeding was resumed on day five and immediate relief of the patient's obstructive symptoms was achieved.
Histologic examination of formalin-fixed, paraffin-embedded sections of the sigmoid colon and rectum showed marked reductions in the numbers of ganglion cells and an intense inflammatory infiltrate in the myenteric plexus, with a predominance of mononuclear cells (Fig. 3). Adequate numbers of ganglion cells were observed in the ascending, transverse, and descending colon (Fig. 4). One year after surgery, the patient was in good health, with one daily bowel discharge. Four years after surgery the patient remained asymptomatic, without having had any medical treatment or hospital admission. Anorectal manometry done 3 y after the patient's surgery found RAIR with an insufflated air volume of 60 mL.
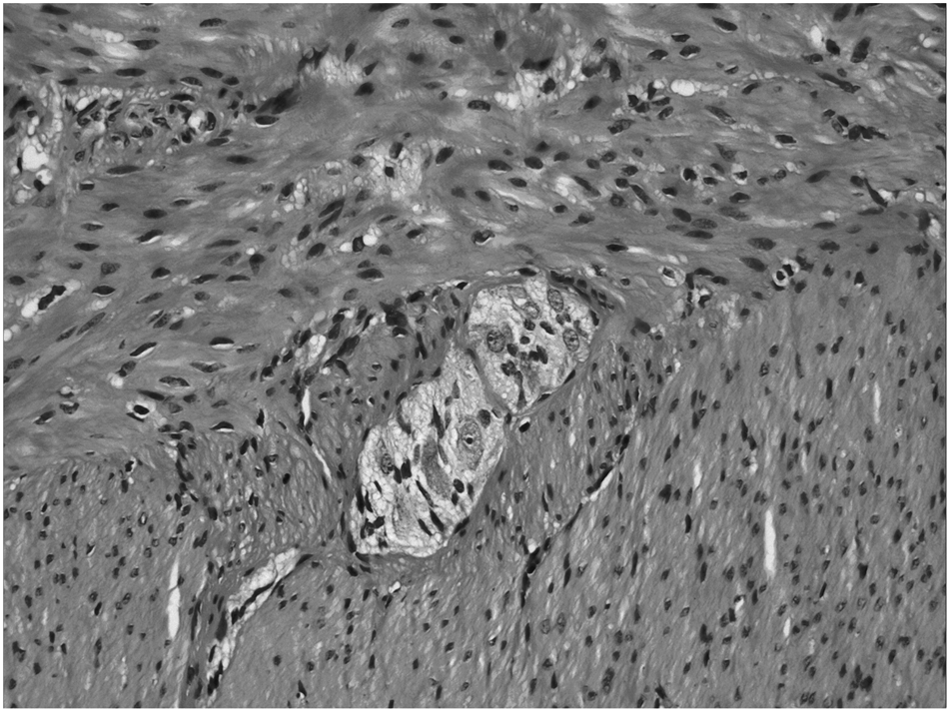
Photomicrograph of sigmoid colon showing inflammatory cells around degenerated neurons.

Photomicrograph of descending colon. Note the absence of myositis and presence of normal numbers of neurons in the myenteric plexus.
Discussion
Chagas disease is an infectious disease caused by T. cruzi, a protozoan parasite endemic in many rural areas of Brazil as well as in other Latin American countries. This protozoan pathogen chiefly affects the heart, esophagus, colon, and rectum, leading to cardiac damage, megaesophagus, and megacolon. However, although megacolon and megaesophagus are the most common gastrointestinal manifestations of infection with T. cruzi, other chronic localizations of such infection are described, such as the stomach, small intestine, gallbladder, and biliary tree [11], causing scialorrhea, megastomach, megaduodenum, megajejunum, megagallbladder, and megacholedochus [12].
Chagasic megacolon is the result of irreversible damage to the intrinsic and extrinsic intestinal nervous system resulting in an increased diameter and length of the large bowel, particularly of the sigmoid and descending colon. In recent years, the physiopathology of chagasic megacolon has been clarified. Extensive neuron loss with ganglionitis and myositis has been found in the myenteric and submucosal plexus in chagasic megacolon. Chronic, irreversible atonic dilation of the colon could result from the loss or malfunction of cholinergic neurons in the disease, whereas nitrergic neurons are less damaged and may appear to be increased in number relative to cholinergic neurons [13]. Because nitrergic neurons inhibit colonic contractility, they are responsible for colonic dilation.
In contrast to the megacolon of Hirschsprung disease, chagasic megacolon is not a consequence of distal aganglionosis. In fact, enteric neurons are present but extremely reduced in number in the dilated segment of colon, with the consequence that chagasic megacolon results from an acquired hypoganglionosis, usually in the recto-sigmoid tract, which should therefore be considered the segment of bowel primarily affected by the disease. The neuronal damage is also responsible for the absence of RAIR, which plays an important role in the mechanism of evacuation [14,15]. According to Cavenaghi et al., air volumes >250 mL are necessary to induce RAIR in chagasic megacolon [16]. In our patient RAIR was absent at a volume of 200 mL of insufflated air. The theory most endorsed is that rectal dyskinesia, with a lack of motor coordination of peristalsis, may result in a functional disorder between contractions of the rectum and relaxation of the internal sphincter of the anus, thus causing constipation [17].
Several procedures have been proposed for the surgical treatment of chagasic megacolon, including sigmoidectomy, abdominal rectosigmoidectomy, left colectomy, and subtotal colectomy. All of them consist of partial or total resection of the dilated region of colon [18,19], with differing morbidity and recurrence rates. Good functional results, with a low rate of recurrence of constipation at long-term follow-up [20,21], have been obtained with the Habr-Gama technique [11], which consists of abdominal rectosigmoidectomy with immediate posterior colorectal end-to-side anastomosis using a circular stapler, thereby eliminating the second stage of the Duhamel–Haddad technique [22,23].
To our knowledge, only one indexed publication described the recurrence of chagasic megacolon after surgery for its treatment [21]. This study examined 10 patients with a recurrence after surgery of severe stipsis (infrequent bowel movements, hard stools, or pain or straining with bowel movements), at a mean of 17.7 y. In all 10 patients dilation of the remaining left colon or of the entire colon was observed. In four of the patients the reason for the failure of surgical treatment was preservation of the rectum or a high colorectal anastomosis. Fecal impaction in the rectum was found in five patients. Considering this drawback, we decided, rather than choosing another technique, to staple the rectum below the peritoneal reflection, thereby reducing both the size of the rectum and the risk of fecal impaction.
The recurrence of stipsis after a long interval following surgery for chagasic megacolon could be a progression of chagasic neuronal degeneration in the preserved colon. We checked for the presence of neurons in the residual segments of the colon of our patient through the intra-operative examination of frozen sections. There are no reports in the literature in which the exact extension of lesions of the enteric nervous system in Chagas disease is estimated, and it is therefore not clear whether chagasic alterations are present in the colonic tract other than in the recto-sigmoid colon at the time of surgery.
Seromuscolar biopsy during surgery could be useful in verifying the site and extent of neuronal damage, glial cell alterations, and the inflammatory response in the enteric plexus in chagasic megacolon to permit tailoring of the extent of colonic resection to a point without signs of initial neuron degeneration.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest.