
Abstract
Abstract
Background:
We report our experience with the surgical closure of late post-pneumonectomy bronchopleural fistula (PBF) using our own method of coverage of the bronchial stump: Pedicled pericardial flap in combination with fibrin glue.
Methods:
We reviewed the surgical results of 33 patients who underwent surgical closure of PBF by thoracotomy access using three methods: Myoplasty (MYO)—12, omentoplasty (OMT)—10, and pedicled pericardial flap (PPF) with fibrin glue—11. Post-operative follow up was six months.
Results:
The patients' demography was comparable among the groups. The diameter of the fistulas ranged from 5 mm to total dehiscence. The mean time of the fistula manifestation (in weeks) was 21.5 in the MYO group, 19.50 in the OMT, and 20.1 in the PPF group. The shortest period of hospital drainage of the pleural space was noted in the PPF group. Healing of the fistula was obtained in 66.67% in the MYO group, 80% in the OMT, and 100% in the PPF group. The number of complications was similar in all groups. The hospitalization time was significantly shorter in the PPF group (13.00 d) versus the MYO group (19.58 d) and the OMT (20.01 d). Overall mortality rate was 18.18%; 33.33% of the patients in the MYO group and 20% in the OMT group died. There were no hospital deaths in the PPF group.
Conclusion:
Pericardial flap supported by fibrin glue can be an effective method adjunctive to the treatment of postpneumonectomy PBF in selected patients. Compared with other methods of bronchial stump coverage (omentopasty and myoplasty), this one showed a higher percentage of healing of the fistulas and shorter duration of hospital drainage and hospitalization.
P
The surgical treatment of late PBF (>30 d after pneumonectomy) remains one of the most difficult challenges for thoracic surgeons, and its results are still unsatisfactory. Recurrence of PBF after surgical repair results in high mortality of 30% to 70%, largely because of respiratory insufficiency and uncontrolled sepsis [9,10]. Standard treatment for persistent PBF involves re-thoracotomy or sternotomy access with primary closure of the fistula with transposition of vascularized autologous flaps to cover the defect and then sterilization of the pleural space. To reinforce the BS, different types of pedicled, well-vascularized flaps (muscular, pleural, pericardial fat, diaphragm, omentum, or vena azygos) are used [11].
Increasingly better treatment effect is obtained in some patients using endoscopic intrabronchial stenting procedures in combination with pleural space drainage [12,13]. In case of the failure of PBF surgical treatment and ineffective chest tube drainage, open window thoracostomy remains the only therapeutic option. Pleural packing for many weeks followed by obliteration of the empyema space with vascularized tissue enables healing of the fistula. Although this approach has been successful in up to 92% of cases, it results in prolonged hospitalization, repeated operative procedures, and substantial morbidity [14].
The objective of this study was to investigate the efficacy of the surgical closure of the late PBF using three various pedicled autologous grafts: Intercostal muscle flap, omental flap, and pericardial flap. We especially recommend our own modification of the earlier known method of the BS coverage by means of pedicled pericardial flap. In our method, we additionally apply fibrin glue on the margins of the fistula before performing the suture to the BS. Postoperative follow-up comprised the period of six months.
Patients and Methods
In the years 1999–2012, 33 patients with late PBF were treated at the Department of Thoracic Surgery, General and Oncological Surgery, Medical University in Lodz. The time criterion suggested by Algar et al. (fistula occurrence >30 d after pneumonectomy) was accepted for the diagnosis of late PBF [15]. The patients treated by bronchoscopic methods and open window thoracostomy and those with early fistula were excluded from the study. Twenty-two of these patients underwent lung resection in our institution. Eleven patients were referred from three other thoracicsurgical institutions. In patients with BF, indications for primary pneumonectomy were the following: Lung cancer (25), abscesses (four), tuberculosis (two), bronchiectasis (one), and aspergilloma (one).
During primary pneumonectomy, the BS closure was made in all of the patients with commercial mechanical thoracoabdominal staplers 35–45 mm (Ethicon, Inc., Johnson & Johnson, Somerville, NJ; and Auto Suture, Covidien, Mansfield, MA). No routine coverage of the BS was performed with autologous tissues to prevent PBF. Only in two patients during primary thoracotomy was the BS covered by a pleural flap. Resection margins were free of carcinoma in all patients.
A PBF was suspected in the presence of fever, cough, or putrid or hemorrhagic expectoration, in combination with increased white blood cell (WBC), C-reactive protein (CRP), and procalcitonin (PCT). Fistula diagnosis was achieved by bronchoscopy in combination with fistulography and radiologic imaging (computed tomography) in all cases.
In 33 patients with late PBF, the following three surgical methods were used via rethoracotomy access to close the fistula: 11 pedicled pericardial flap (PPF) with fibrin glue, 12 myoplasty (MYO), and 10 omentoplasty (OMT). The technique for the fistula closure was chosen randomly in the investigated group. After hospital discharge, the patients were followed up on an outpatient basis for six months.
Surgical Technique
The initial step in the management of patients with postpneumonectomy empyema was chest tube drainage to achieve local source control. After confirmation of the PBF diagnosis, the patients were qualified for surgical treatment by re-thoracotomy access. Mechanical debridement of the pleural cavity was made intraoperatively with the exposure of the edges of the BS.
In the OMT group, omental flap transposition performed through a thoracotomy access for BS coverage was performed in 10 patients according to a standard technique described by Yokomise et al. [16]. In the MYO group, myoplasty technique, similar to that described by Hollaus et al. [10] and Garcia-Yuste et al. [17], was used in 12 patients to close the fistula. The bronchial stump was covered with intercostal muscle bundle (nine cases) and pedicled latissimus dorsi flap (three cases).
In the remaining 11 patients from the PPF group, to repair the fistula, our modified method was applied using a pedicled pericardial flap glued with fibrin on the BS margins. In detail, during PPF procedure, the patients were intubated with a double-lumen endotracheal tube to protect the contralateral lung until the PBF was ruled out definitively. After debridement of the pleural space and irrigation with 0.1% chloramine, the fistula margins were sutured with four nonabsorbable single deep mattress sutures of 3–0 or 4–0 PDS (polydioxanone, Ethicon, Somerville, NJ) monofilament absorbable suture inserted “en mass” through the bronchial wall and the surrounding mediastinal tissues (opposing each other). Then, fibrin glue (Tissucol, Baxter Healthcare Corporation, Deerfield, IL) was applied on bronchial edges around the fistula, which was closed immediately with surgical sutures (Fig. 1). The sealant transforms into a stable fibrin clot within three to five minutes. The incision of the pericardial sac and preparation of the pedicled flap from the anterior pericardium (without phrenic vessels) was the next stage of the procedure. The flap should be long enough (about 2 cm) to cover the fistula with no tension at the free margin. The flap was attached cap-like over the closed fistula and sutured tightly with continuous sutures (4–0 PDS) (Fig. 2). The BS was then checked for air leakage with 30 cm H2O sustained airway pressure. At the end of the procedure, special attention was paid to the restoration of the pericardium to prevent cardiac herniation. We routinely applied Vicryl® mesh for that purpose (Ethicon Johnson & Johnson, Somerville, NJ). Continuous pleural irrigation was performed post-operatively in all patients until pleural lavage was clear.

Visible application of fibrin glue on internal edges of the bronchial fistula, earlier interrupted surgical sutures were performed.
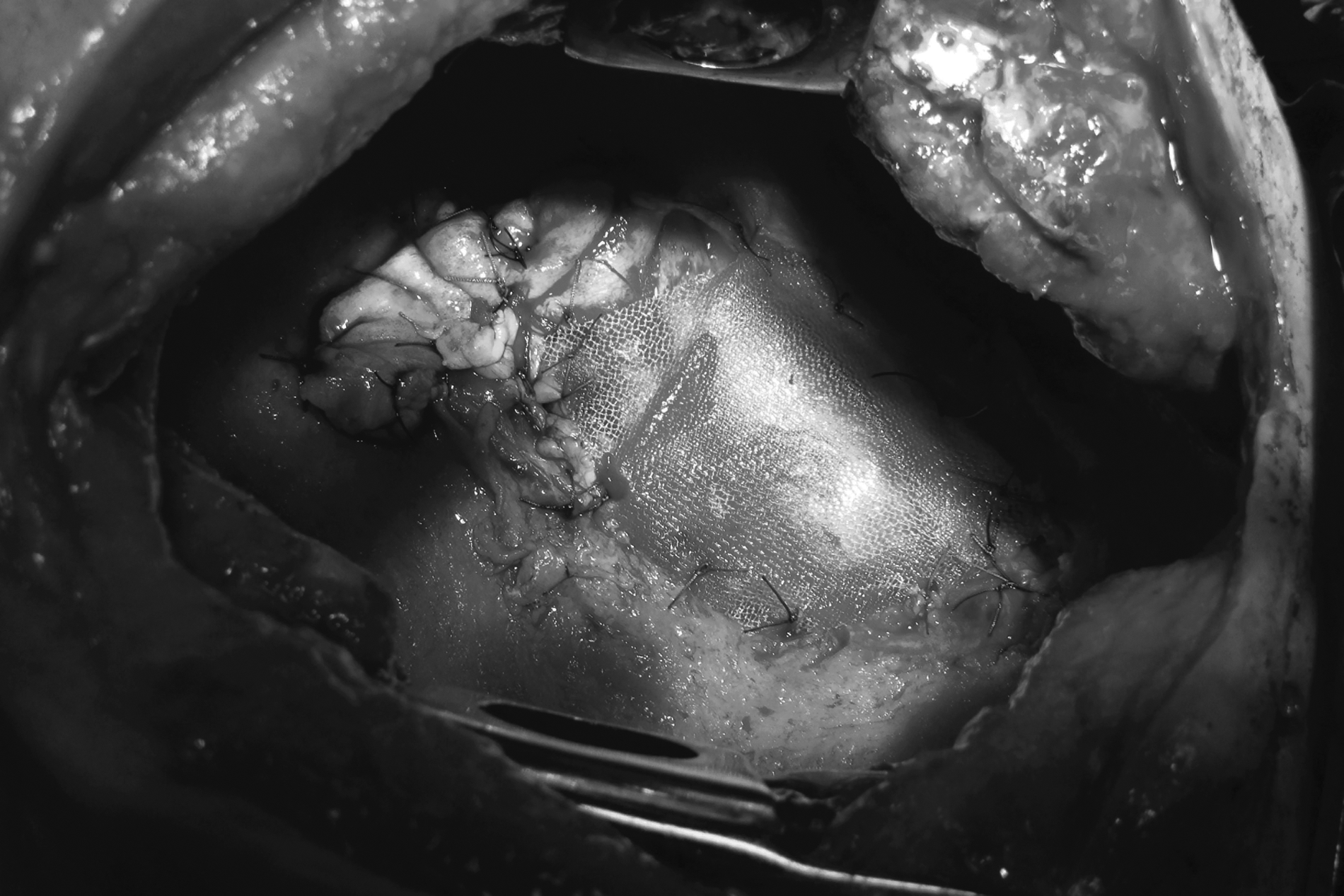
Final stage – the bronchial fistula covered with pericardial flap fixed to the surrounding tissues with single sutures, pericardial sack reconstructed with polypropylene meshwork.
In patients with severe local inflammatory process and coexisting sepsis, three repetitive re-thoracotomies were performed with surgical debridement and antiseptic packages of the pleural cavity according to the technique described by Shneiter et al. [18]. Three patients from the PPF, two from the MYO, and one from the OMT group underwent these procedures to sterilize the pleural space and create better conditions for PBF healing.
Statistical Analysis
The Student t test was used for comparison of means and the Mann-Whitney U test was used if abnormal distribution was detected in continuous data. For categorical data comparison, the independent Chi-square test was applied. The level of significance was established as p<0.05. ANOVA or Kruskal-Wallis test (when variance differed significantly among the subgroups) was applied to investigate the effect of the treatment method on therapy results. Likelihood ratio test for independence was used for categorical data comparison, that is, the influence of three methods of treatment on the therapy results. Significance level was established as p<0.05.
Results
Demography
The MYO group included 10 men and two women, with a mean age of 57.83 y (median: 57.5). The OMT group consisted of nine men and one woman, with a mean age of 59.9 y (median: 59.5). In the PPF group, there were nine men and two women, with a mean age of 55.27 y (median: 55.00). The groups did not differ statistically regarding demographic features (ANOVA p=0.52041).
Indication for primary pneumonectomy
In the patients from the MYO group, the reasons for primary pneumonectomy were lung cancer (seven) [three after previous chemotherapy], lung abscess (two), aspergilloma (two), and tuberculosis (TBC) with empyema (one). In the OMT group, the indications for pneumonectomy were lung cancer (eight) [one after chemotherapy], abscess with empyema (one), and bronchiectasis (one).
In eleven patients from the PPF group, pneumonectomy was performed because of lung cancer (nine) [two after neoadjuvant chemotherapy] and TBC with multiple lung abscesses (two).
Fistulas location, time of the manifestation and size
The PBFs occurred on the right side in 30 patients (90.90%) and on the left side in three of them (9.09%). In the MYO group, the fistula manifested itself within the period of five to 49 weeks after pneumonectomy (mean: 21.50 wk). In the OMT group, the fistula was observed within the period of seven to 31 weeks (mean: 19.50 wk). The time of fistula manifestation in the PPF group was from seven to 49 wk (mean: 20.09 wk). The time of PBF manifestation did not differ among the investigated groups (ANOVA, p=0.9358).
The fistula diameter ranged from 5 mm to total dehiscence (15 mm). Mean fistula diameter was 11.33 mm (median: 12.50 mm) in the MYO group, 9.8 mm (median: 10.00 mm) in the OMT group, and 11.09 mm (median: 11.00 mm) in the PPF group. No statistically significant differences were confirmed in relation to the fistula size among the groups (p=0.4485).
Drainage duration
In the MYO group, the duration of the hospital drainage of the pleural cavity was from five to 24 d (mean: 10.92 d). The prolonged air leak or infected fluid was observed in three patients, and they were discharged from hospital with a passive compact drainage system for the ambulatory management. The chest tube was finally removed five, eight, and 10 days after the surgery.
In the OMT group, the time of hospital drainage was from four to 19 d (mean: 9.20 d). The compact drainage was continued in three patients after hospital discharge. It was finally removed six, eight, and 10 days after surgery.
In the PPF group, the length of hospital drainage was from three to 12 d (mean: 7.72 d). In four patients, the drainage was continued on an outpatient basis. When the pleural space was sterilized and air leak stopped, the drainage was removed in all patients (six to 15 d). In PPF patients, the length of hospital drainage was shorter than in the remaining two groups, but it was not statistically significant (p=0.2741).
However, the total drainage duration (including that on the outpatient basis) was similar in these three groups (mean value: MYO, 12.17 d; OMT, 9.2 d; and PPF, 11.45 d). The length of the total drainage of the pleural cavity did not depend on the applied method of treatment (ANOVA, p=0.6484).
Hospitalization time
The time of hospitalization was from eight to 32 d (mean: 19.58 d) in the MYO group, 12 to 34 d (mean: 20.01 d) in the OMT group, and 10 to 19 d (mean: 13.63 d) in the PPF group. The shortest hospitalization time was observed when PPF treatment method was applied (Fig. 3) (Kruskal-Wallis test: p=0.05320, ANOVA: p=0.0531).
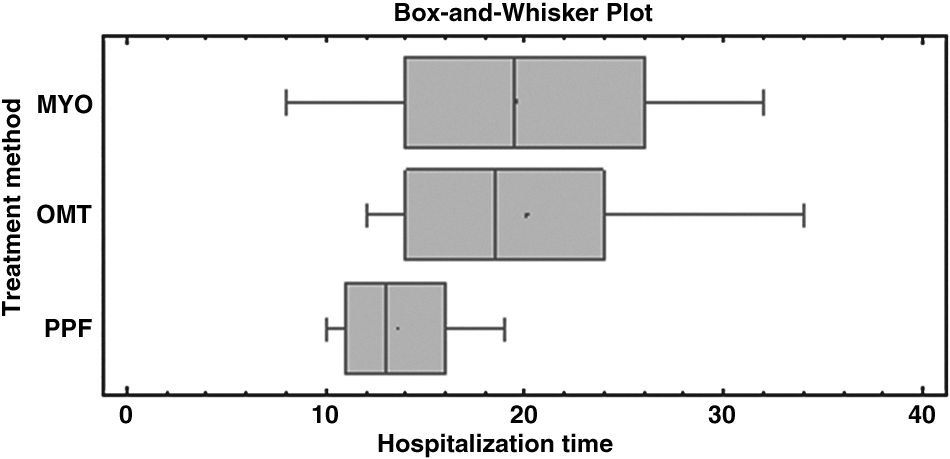
Comparison of the hospitalization time among the groups.
Fistula healing
In the MYO group, closure of the fistula was achieved in eight patients (66.67%). The recurrence of PBF was observed in four patients (33.33%), two of whom died. In the first patient who survived the recurrence, the fistula was controlled with an endobronchial stent. In the second patient, open window thoracostomy was performed. After pleural cavity sterilization, the fistula was closed successfully in the second stage by omentoplasty.
In the OMT group, success in closing the fistula was achieved in eight patients (80.00%). In two patients, PBF recurrence was observed (20.00%), and one patient died. In one patient who survived, persistent drainage was applied as further treatment.
Healing of the fistula was obtained in all 11 patients in the PPF group. The highest rate of fistula healing was observed in patients treated by the PPF method (p<0.05) (Fig. 4).
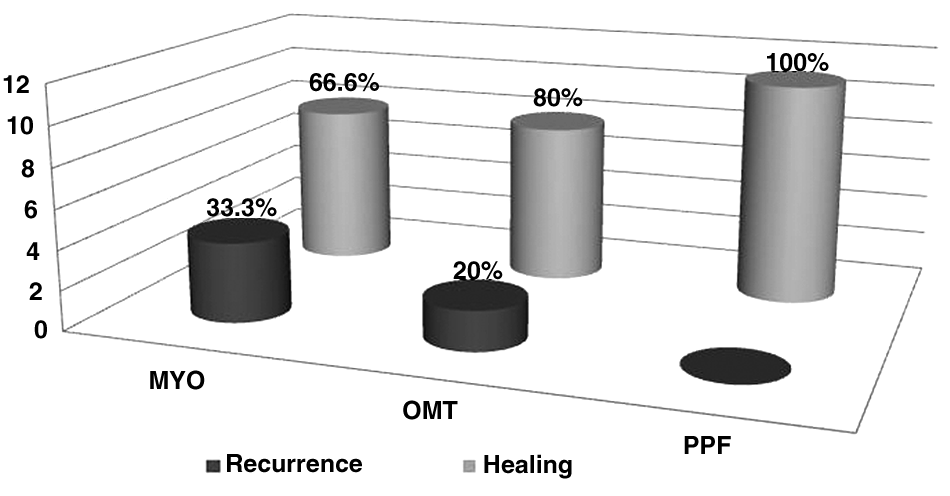
The effectiveness of the three methods for bronchial fistula closure.
Complication and mortality
Overall mortality rate for all 33 patients surgically treated for PBF was 18.18% in the perioperative period and 24.24% in the six month follow up period (deaths after discharge from hospital). The rate of hospital mortality in individual groups was: 33.33% in the MYO group, 20% in the OMT group, and no deaths in the PPF group. The mortality rate on follow-up completion differed insignificantly as it was 33% in the MYO group, 30% in the OMT group, and 9% in the PPF group.
In the MYO group, four patients died during hospitalization because of aspiration pneumonia with respiratory insufficiency (two), empyema with fistula recurrence (one), and massive gastric hemorrhage (one). The following minor complications were observed in the MYO group patients: prolonged air leak (two), surgical site infection (two), recurrence of empyema without fistula (one), pulmonary edema (one), atrial fibrillation (one), and arrhythmia (one).
In the OMT group, two patients died in the post-operative period for the following reasons: Aspiration pneumonia with respiratory insufficiency (one) and myocardial infarction with circulatory insufficiency (one). One patient died during the follow up period. Different minor complications were also observed, that is, subphrenic abscess (one), pneumonia (one), surgical site infection (two), abdominal distension (one), and arrhythmia (one).
In the PPF group, no hospital death was noted. Within six post-operative months, a recurrence of pleural empyema but without bronchial fistula was noted in three patients. In two patients, to sterilize the pleural cavity, continuous pleural lavage was used successfully. In the third of these patients, the empyema persisted despite drainage. Four weeks after surgery, heart failure was experienced caused probably by tight reconstruction of the pericardium, which required re-operation. After the next two weeks, the patient died because of cardiorespiratory failure. Arrhythmia (two) and infection of the thoracotomy incision (one) were observed among less severe complications. Statistical analysis showed that the incidence of complications was not related to the method of treatment (p=0.3756).
Discussion
The initial management of patients with late PBF includes effective drainage of the infected pleural space, antibiotics to treat the infection, and adequate clearance of secretions from the remaining lung. Definitive surgical repair should be delayed until the patient is in optimal condition and the cavity is clean [6]. The drainage of the empyema cavity is essential to control sepsis. Closed drainage often fails to drain the cavity completely with subsequent unsatisfactory control of the infection; in these cases, open drainage is performed [17,19]. Currently, three main types of the management of late PBF can be distinguished: Surgical repair, intrabronchial techniques, and open window thoracostomy.
The recommended surgical treatment for persistent PBF involves thoracotomy or sternotomy with primary closure and transposition of well-vascularized autologous flaps to cover the bronchial leak site and occupy the empty post-pneumonectomy space.
These surgical procedures are usually complicated and dangerous, and often, the treatment results are unsatisfactory. The success rate of PBF surgical closure has been reported in the range of 30% to 85%, with a mortality rate of 19.5% to 71% [9,10,20,21]. Endobronchial management of PBF is an attractive therapeutic option with no need for re-thoracotomy [12,13]. However, this technique can be applied only in selected patients, and most of them require another operation. The best results of endoscopic treatment are obtained in patients with fistulas smaller than 3 mm and with no co-existing life-threatening sepsis [22]. Hollaus et al. reported successful endoscopic fistula closure in 35.6% of patients, but at the same time, 35.6% of them required surgical intervention [22]. Open window thoracostomy is a method designed for patients after earlier unsuccessful treatment of PBF or as preparation for the next stage of treatment. The Clagett procedure and its modifications control the infection locally and improve the general condition. Combined with intrathoracic flap transposition, they contribute to the successful treatment of about 50%–75% of PBFs [17,23]. However, despite its positive effects, this method causes serious deformation of the chest, it is long-lasting, and tolerated poorly by patients. Pleural cavity wet dressings cannot control air leaks, which leads to severe respiratory insufficiency associated with high mortality.
As mentioned previously, the basis for surgical therapy of an open BS is its closure and reinforcement with well-vascularized tissue and sterilization of the pleural space [11]. Various pedicled flaps are used to cover the fistula depending on local conditions, their availability, the length and quality of bronchial wall, fixation in the mediastinum, and preferences and experience of the surgeon. Because of ischemia at the bronchial edge and the infected environment, the choice of autologous tissue for PBF coverage seems to be of crucial importance for optimal results.
Each of the methods using autologous flaps in the treatment of PBF has its benefits and limitations. Pleural flap is quite thin, and it has poor blood supply. It is usually used only to prevent the incidence of fistula during pneumonectomy [24,25]. The use of greater omental flaps has proved to be effective in the management of several complex thoracic surgical problems [26]. The omentum has a rich vascular supply assuring adequate oxygen and antibiotic delivery. Additionally, the omentum delivers potent angiogenic factors. No such factors have been found in muscle [27,28]. The greater omentum also provides good coverage to the BS [16]. Morgan et al. [29] showed in a canine model that ischemic bronchial tissue may be revascularized within four days after omental wrapping. Despite these enthusiastic reports, omentoplasty has a number of limitations. First, omentoplasty requires a separate abdominal incision, which poses a risk of infection in an additional body cavity; the surgery takes an extra 50–70 min [30]. In such conditions, omentoplasty can be unsuccessful in about 50% of patients [30,31]. The most serious complications of omentoplasty include ileus, gastrointestinal bleeding, abdominal distension, diarrhea, and anorexia [32]. In our study, we obtained 80% efficacy in PBF closure, and the mortality rate was 20%.
The use of diaphragmatic pedicle flap for closure of the bronchial fistula is not popular. Its advantages include easy access, and it is large enough to cover the defect [30,31]. However, similar to omentoplasty, the opening of the abdominal cavity poses a potential risk of infection. We observed that the diaphragm in late PE is rigid and shortened, and its vascularization can be poor. In such conditions, the flap does not adhere tightly to the fistula, which leads to air leak and to the recurrence of the fistula. Mineo et al. [33] listed arrhythmia, respiratory insufficiency, empyema recurrence, and bleeding among complications associated with diaphragm plasty.
Muscle flaps were used to buttress bronchial fistulas and to fill out residual spaces; they do not require the opening of the abdomen and are more easily borne by patients, which is an advantage. From extrathoracic muscles, intercostal muscle flaps are used preferentially in the treatment of PBF in some institutions [34]. However, reports concerning the treatment with their use are frustrating. Fistula recurrence reaches 50–66%, with an overall mortality rate of 50% [35,36]. Because of poor blood supply and necrosis, they are not effective in PBF repair. In the later period, a rare complication of heterotopic ossification can be observed [37]. In our experience, intercostal muscle flaps are easy to prepare, but it happens that they are too narrow, which causes problems with fixing them around the fistula. They do not adhere well to the BS and have a tendency to contract and to lead to necrosis. From among other muscle flaps, latissimus dorsi, pectoralis major, and serratus anterior are used most frequently for bronchial fistula coverage. Easy access, large surface, and relatively good blood supply are the advantages of these flaps. When a single muscle is not sufficient, two or more muscles may be used. In current literature, muscle flaps are reserved for situations where omentum is not available or circumstances where the residual cavity is obliterated concomitantly [6]. Chest deformations, muscle dysfunction, seromas, chest wall complaints, and winged scapula, which sometimes requires additional scapulectomy, are serious complications associated with their use [20]. In our experience, myoplasty had the worst results; PBF closure was obtained in 66.67% of the patients; overall mortality was 33.33%.
As far as pericardium is concerned, in the current literature, the use of pericardial fat or pericardium itself is described to be used for bronchial coverage during pneumonectomy to prevent the incidence of a fistula but seldom as a separate method of late PBF closure [38]. The idea of use of the pericardial flap for the reinforcement of BS during pneumonectomy is not new; it was described for the first time by Brewer et al. as an alternative method to the pericardial fat graft [39].
Often, insufficient length, width, consistency, vascularization, and the risk for pericarditis are mentioned among the drawbacks of pleural and pericardial flaps [30,40]. In our experience, we have observed that the pericardial flap demonstrates favorable properties. Pericardial sac is in the direct neighborhood of the PBF; a well-prepared flap has proper diameter and consistency, and it demonstrates good adhesiveness to the BS. We have never observed cases of ischemia or necrosis. It should be remembered that, at the end of the operation, the pericardium must be reconstructed to prevent heart dislocation. To avoid pericardial restriction, it is important to sterilize the pleural cavity carefully and to close the pericardial defect loosely. In patients with acute empyema, a soft catheter is placed in the pericardial sac with an exit site on the skin. The catheter allows evacuation of the infected fluid and irrigation of the pericardium with antiseptics. When the effluent becomes clear, the catheter can be removed easily. In our patients, no purulent pericarditis was observed in the early postoperative period, despite the potential risk for this complication.
The use of biologic glue is an important element of the technique of PBF closure. The application of fibrin glue for reinforcement of the BS after pulmonary resection is well known [41]. In our opinion, the biologic glue improves the seal obtained after suturing the ends on the fistula edges. This technique is used relatively frequently during endoscopic procedures [12,13].
Comparing the results of PBF treatment in our patients, with the use of three methods, we can say that the described PPF technique is more effective in regard to the number of healed fistulas and hospitalization time. The use of the patient's own pericardium has been the preferred method for PBF coverage in our department during the last five years. The shortest overall hospitalization time was obtained in patients treated by the PPF method, followed by MYO, and the longest was obtained in those who underwent the OMT procedure. The mean time of pleural cavity drainage turned out to be similar to that in patients operated on by traditional methods. The lack of perioperative death should be emphasized as beneficial for this method. The general number of complications and death rate within the six month follow up were similar. Obviously, we realize that the efficacy of the method should be confirmed in by observation of larger cohort of patients.
Conclusion
Pericardial flap supported by fibrin glue can be an effective method adjunctive to the treatment of post-pneumonectomy bronchial fistula in selected patients. Compared with other methods of the BS reinforcement (omentopasty and myoplasty), this one showed a higher percentage of healing of the fistulas and shorter hospital drainage time and hospital stay.
Footnotes
Authors Disclosure Statement
No competing financial interests exist.