
Abstract
Abstract
Background:
Peritoneal dialysis (PD)–related peritonitis is the most common complication and the leading cause of technique failure for patients on PD therapy. The aim of this study was to review the episodes and outcomes of PD-related peritonitis, with special reference to the effects of age and diabetes status.
Methods:
The study comprised 204 consecutive peritonitis episodes between January 2001 and June 2011 from our registry database. Factors associated with treatment failure and mortality were analyzed with multi-variable logistic regression modeling.
Results:
The overall peritonitis rate was one episode per 65 patient-months or 0.187 episodes/patient-year. Older patients had lower probability of remaining free of peritonitis (log rank, p<0.001). Elderly patients and diabetic subjects had a higher risk of peritonitis-related dropout. Age (odds ratio [OR], 1.37; p=0.041), diabetes mellitus (OR, 3.64; p=0.005), and gram-negative peritonitis (OR, 3.55; p=0.011) were independent determinants of catheter removal. Age (OR, 1.93; p=0.026) and diabetes (OR, 5.98; p=0.015) were the only predictors of death from peritonitis.
Conclusions:
Old age and diabetes mellitus are two major risk factors for adverse outcomes of PD-related peritonitis. Although they are not contraindications to PD, our results suggest that these patients need meticulous care when peritonitis occurs.
P
The elderly patient population is the fastest-growing demographic of end-stage renal disease (ESRD) in developed countries [5]. A recent study demonstrated that, in contrast to young patients, PD was not associated with longer survival than hemodialysis in elderly or diabetic patients [6]. However, quality of life might be similar (if not better) in elderly patients on PD therapy [7]. Therefore, dialysis modality choice for the older patient with ESRD should be individualized based on the benefits and risks of the modality, patient co-morbidities, and family resources. In this regard, there have been conflicting data on the risk and outcomes of peritonitis in elderly patients.
Previously we have shown that PD is a feasible and safe option for elderly patients [8]. Despite a longer hospital stay, elderly patients had similar overall complication rates and catheter survival to those of the younger group in the short term. However, the impact of age on PD-related peritonitis was not addressed specifically in our previous study. The purpose of the present study was to review the episodes and outcomes of PD-related peritonitis in our patient cohort, with special reference to the effects of age and diabetes status.
Patients and Methods
This cohort study included consecutive adult patients who were receiving PD in our hospital between January 2001 and April 2011. Data were retrieved from individual clinical records and our computerized renal registry. In all cases, prophylactic cefazolin was administered prior to surgical placement of a double-cuffed, straight Tenckhoff catheter [8]. After catheter placement, intravenous cefazolin was administered routinely for one day. Peritoneal dialysis was initiated after a break-in period of two weeks. All patients were provided with a glucose-based dialysate and twin-bag connection system.
All episodes of PD-related peritonitis from January 2001 to June 2011 were reviewed. Patients were asked to contact us as soon as possible if they experienced cloudy effluent or abdominal symptoms. Peritonitis was defined as clinical features of peritonitis (abdominal pain or cloudy effluent) and dialysate leukocytosis (white blood cell count >100/mcL with ≥50% neutrophils) [4]. Recurrent peritonitis was defined as an episode occurring within four weeks of completion of therapy of a prior episode but with a different organism. Relapsing peritonitis was defined as an episode occurring within four weeks of completion of therapy of a prior episode with the same organism or one sterile episode. Repeat peritonitis was defined as an episode occurring more than four weeks after completion of therapy of a prior episode with the same organism. Relapsing episodes were not counted when calculating peritonitis rates; whereas recurrent and repeat episodes were counted.
Peritonitis episodes were treated with a standard antibiotic protocol at our hospital. Initial antibiotics for peritonitis were ceftazidime with cefazolin administered intra-peritoneally. Intravenous antibiotics were used when the patient appeared to have sepsis clinically. Peritoneal dialysis effluent were sent for bacterial and fungal culture by inoculation into blood culture media, and observed for at least 72 h to document pathogens. Anti-microbial susceptibility was determined by standard disk-diffusion methods. Antibiotics were changed subsequently according to the culture and sensitivity results of the dialysis fluid. Tenckhoff catheters were removed and patients were put on temporary hemodialysis therapy when peritonitis failed to resolve with antibiotics.
Patients were followed up until death, stopping PD, or August 2011, at which point data were censored. Treatment failure included death and catheter removal/switch to hemodialysis required for the resolution of peritonitis. Mortality related to peritonitis was defined as death of a patient with active peritonitis or within two weeks of a peritonitis episode.
Continuous variables are expressed as medians with inter-quartile ranges. Categorical variables are expressed as frequencies and percentages. Continuous variables were compared using the Mann-Whitney U test. Proportions were compared by the Fisher exact test. Multivariable analyses with forward stepwise logistic regression modeling were used to test for factors associated with treatment failure and mortality. Baseline variables that achieved a p value of <0.1 in uni-variate analyses were included in multi-variable analyses. Odds ratios (ORs) and 95% confidence intervals were calculated. Time to first peritonitis episode and peritonitis-specific technique survival were examined using Kaplan-Meier plots with the log rank test [9]. Throughout the analyses, p values less than 0.05 (two-sided hypotheses) were considered to be statistically significant.
Results
During the study period, there were 204 peritonitis episodes diagnosed in 128 of 349 patients undergoing regular PD over a cumulative follow up period of 12,113 patient-months, including 17 episodes of relapsing peritonitis. Therefore, the overall peritonitis rate was one episode per 65 patient-months or 0.187 episodes/patient-year. Of the cohort patients, 80 had one peritonitis episode; 36 had two peritonitis episodes; five had three peritonitis episodes; three had four peritonitis episodes; and four had five or more episodes.
In all, the median age of starting PD was 53 y (range, 18–91). The median time to first peritonitis was 15 mo (range, 1–96 mo). As shown in Figure 1, older PD patients had lower probability of remaining free of peritonitis. At 1 y of starting PD, the probability of experiencing a first peritonitis episode was 13% in the younger group and 24% in the elderly group. After 5 y, the probability of experiencing a first peritonitis episode was 47% in the younger group and 64% in the elderly group.
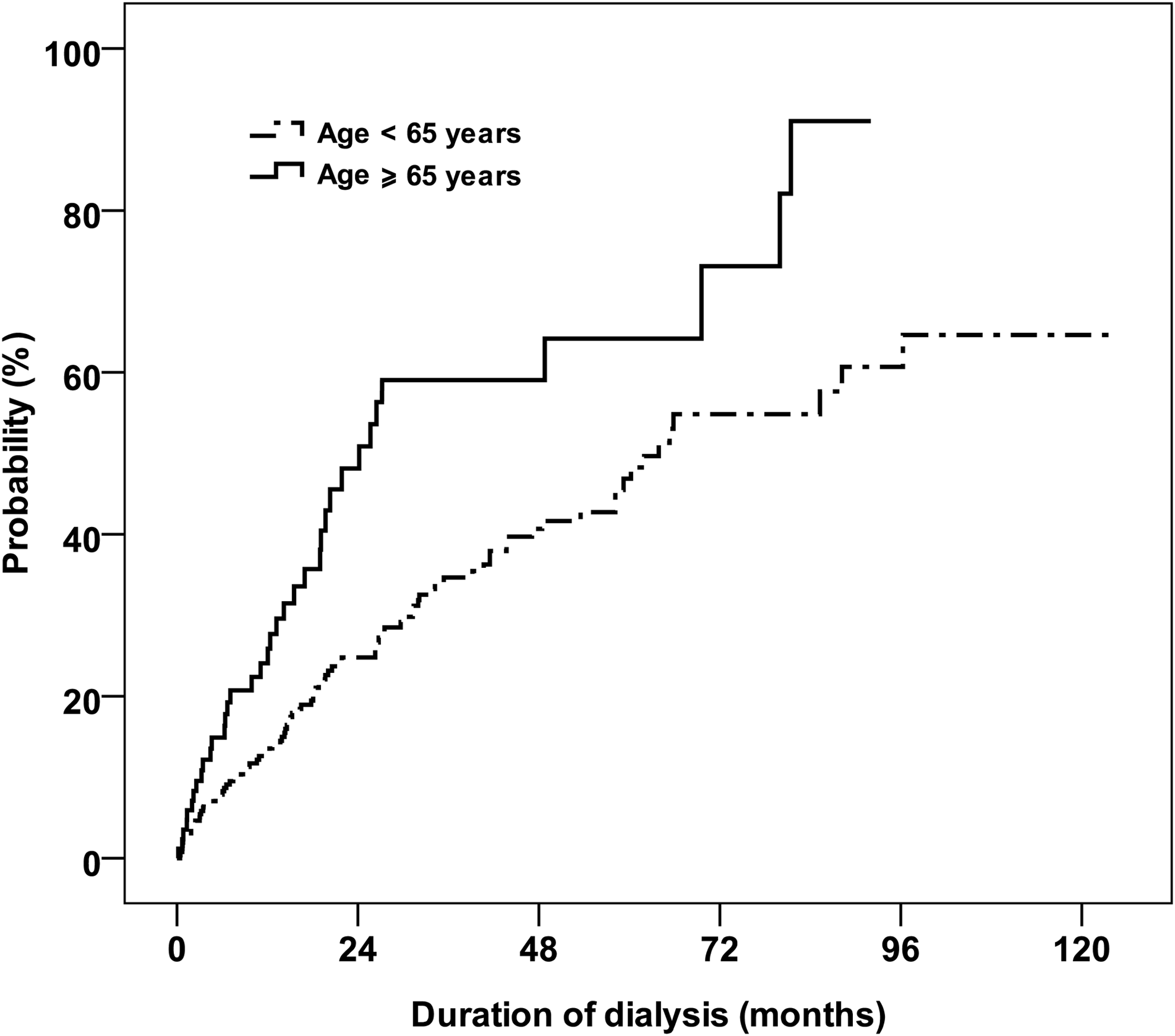
Cumulative incidence curves for the first episode of peritonitis calculated by the Kaplan-Meier methods. Old age (≥65 years) was associated with a significantly increased likelihood of developing first peritonitis (log rank p<0.001).
Of the 349 subjects, 30% had diabetes mellitus. Diabetes was associated with an older age of starting PD (59 vs. 47 y; p<0.001). At 1 y of starting PD, the probability of experiencing a first peritonitis episode was 13% in the non-diabetic patients and 26% in the diabetic patients. However, the Kaplan-Meier curve showed that there was no difference in the cumulative incidence of first peritonitis episode among patients with and without diabetes mellitus (Fig. 2).

Cumulative incidence curves for the first episode of peritonitis according to diabetes mellitus status, calculated by the Kaplan-Meier methods. No significant difference was seen by log rank test (p=0.113).
In 204 peritonitis episodes, 57 (28%) were culture-negative. More than one organism was isolated from the dialysis fluid in 11 (5%) episodes. Among 147 episodes with organism cultures, a total of 161 organisms were identified. The most frequent organism was Escherichia coli and Streptococcus species. The detailed categories of organisms are shown in Table 1. Diabetes mellitus status did not influence the microbial profile. The elderly had lower prevalence of gram-positive organisms (31% versus 46%, p=0.046). The prevalence of gram-negative organisms was 35% in patients 65 y or older and 28% in patients younger than 65 y (P=0.323). There was no difference in the microbial profile between initial and subsequent peritonitis episodes.
Among the 204 peritonitis episodes, resolution was observed in 160 (78%). A total of 44 patients experienced treatment failure of PD-related peritonitis (25 at the first episode; 14 at second; three at the third episode; one at the fourth episode; and one at the sixth episode), including 13 peritonitis-related mortality. Patients age ≥65 y or with diabetes mellitus had a significantly higher risk of catheter removal/transfer to hemodialysis following peritonitis (Figs. 3 and 4). Table 2 shows that catheters were likely to be removed in patients with older age, diabetes mellitus, the presence of gram-negative organisms, and fungal or mycobacterial peritonitis. Catheters were more likely to be retained in gram-positive peritonitis episodes. In a 55-year-old non-diabetic male, peritonitis was confirmed with dialysate leukocytosis (white blood cell count 120/mcL with 76% neutrophils). Five days after peritonitis, dialysate culture yielded Ochrobactrum anthropi. Although fungal culture positive for Candida haemulonii and Acremonium species were noted one month after the presentation of peritonitis, the catheter was not removed because of clinical resolution of peritonitis. It is the only exception to the general trend that fungal peritonitis was associated with catheter loss.

Kaplan-Meier curves for peritonitis-specific technique survival of peritoneal dialysis (PD) patients, censored for stopping PD and for death. Differences between the groups were statistically significant (log rank p<0.001).
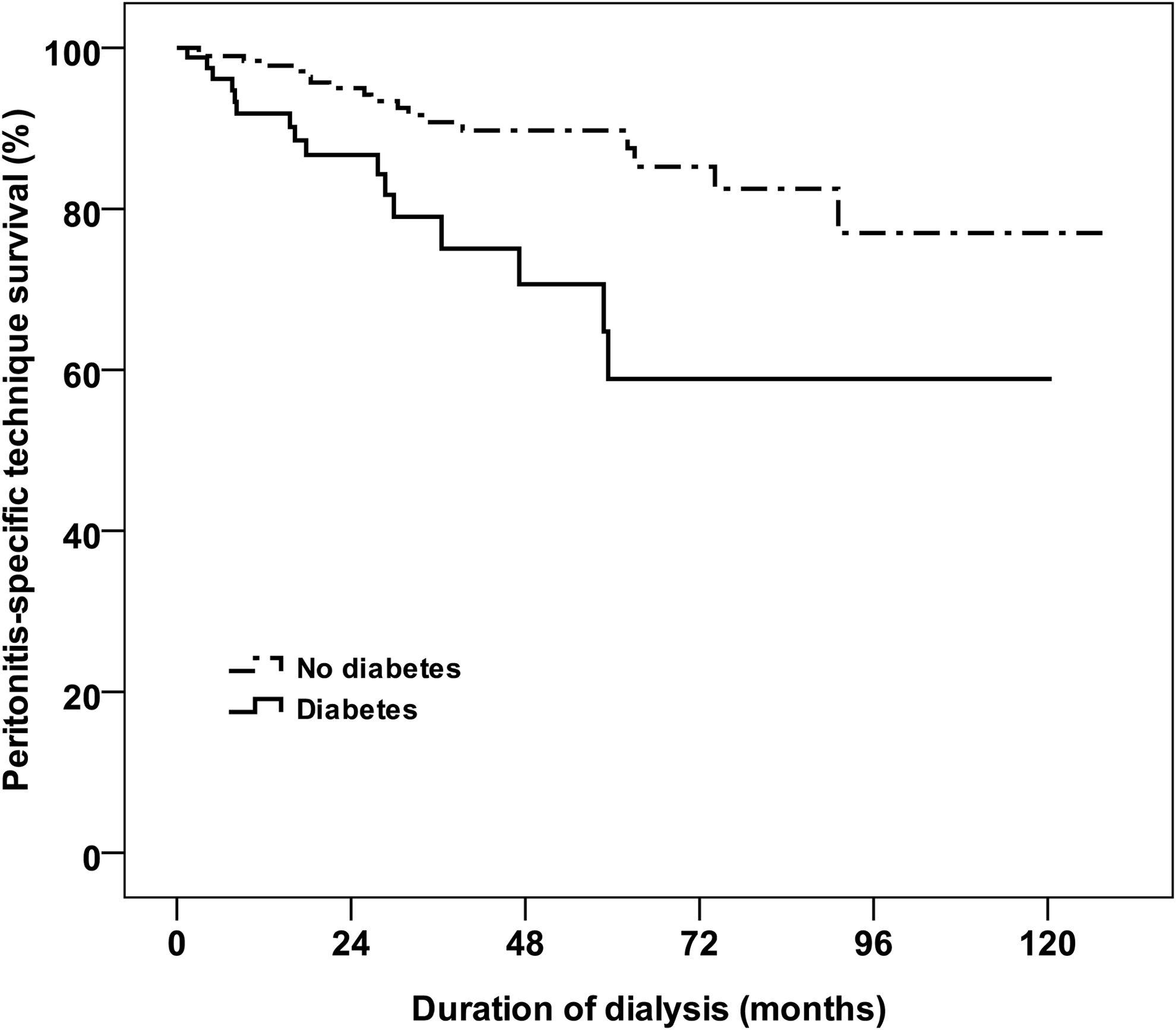
Kaplan-Meier curves for peritonitis-specific technique survival of peritoneal dialysis (PD) patients, censored for stopping PD and for death. Patients with diabetes mellitus had a significantly higher risk of catheter removal/transfer to hemodialysis following peritonitis (log rank p=0.001).
Multi-variable logistic regression analysis was performed to assess the risk factors of treatment failure. As shown in Table 3, age at the time of peritonitis (per 10-y increase: OR, 1.37; p=0.041), diabetes (OR, 3.64; p=0.005), and gram-negative peritonitis (OR, 3.55; p=0.011) were identified as significant determinants of treatment failure.
CI=confidence interval.
Peritonitis-related death was observed in 13 patients. Characteristics of patients with a fatal outcome are listed in Table 4. Mortality was positively associated with age at the time of peritonitis, diabetes mellitus, the presence of gram-negative organisms, and fungal or mycobacterial peritonitis, and negatively associated with gram-positive peritonitis. The duration of dialysis and previous peritonitis episodes were not significantly different between the groups. In multi-variable logistic regression analysis (Table 5), age at the time of peritonitis (per 10-y increase: OR, 1.93; p=0.026) and diabetes mellitus (OR, 5.98; p=0.015) are independent predictors of death from PD-related peritonitis.
CI=confidence interval.
Discussion
The results of the present study clearly showed that old patients had lower possibilities of remaining peritonitis-free, higher rates of catheter removal and hemodialysis therapy transfer, and higher risks of dying from PD-related peritonitis. Chronological age is not necessarily associated with biological and functional declines [10]. However, experimental data suggested that aging is invariably accompanied by the presence of an inflammatory state in peritoneal mesothelial cells [11]. It is controversial whether older patients have a higher peritonitis rate. Some studies indicate that old age is an independent risk factor for peritonitis [12–15], whereas others failed to confirm such findings [16–19]. An era effect has been proposed in this regard [20]. It is also debatable whether older patients have worse clinical outcomes following peritonitis. Older age was associated with an increased risk for treatment failure in some studies [17,21,22]. Nonetheless, in other reports, age did not affect the outcome of peritonitis [16,23–25].
Nutritional status may be an important confounding factor that was not included in our study. Impairment of masticatory ability in the elderly correlates to lower serum concentrations of albumin [26]. In addition, plasma protein loss from the peritoneum was significantly greater in elderly PD patients, resulting to lower serum albumin levels [27]. Low serum albumin concentrations are associated with a shorter time to first peritonitis episode [28] and more complicated course of PD-related peritonitis or catheter loss [24,25]. Interestingly, the observation that old age increases the risk of peritonitis-related death seems consistent across the studies [17,19,29,30]. Although it is likely a consequence of a greater prevalence of comorbidities in the elderly, malnutrition may independently compromise patient survival during peritonitis episodes [29].
In this study, we also highlight that diabetes mellitus heightens the risk of treatment failure and mortality. Chronic hyperglycemia is associated with functional and structural peritoneal changes, which are prevented by insulin treatment [31]. Furthermore, diabetes mellitus may alter immunity of peritoneal defense, decrease bowel transit time, and increase formation of advanced glycation end products and glucose degradation products [32], leading to undue susceptibility to infection. Some previous studies support the notion that diabetes increases peritonitis risk [13,14,28,33], but others do not [12,15,18]. Contrary to our present findings, most series suggest that outcomes were not different between diabetic and non-diabetic patients [21,23–25,34], although decreased survival in diabetic patients was similarly reported in Japan [15]. The reason for this discrepancy is not clear. One limitation of our study is that the information of residual renal function and degree of glycemic control was not available in our peritonitis registry. Degree of glycemic control may influence considerably the integrity of the peritoneal membrane and treatment response to peritonitis.
Compared with hemodialysis, PD offers cardiovascular, retinal, and renal benefits in diabetic patients [35]. However, diabetes remains a poor prognostic factor for survival of elderly patients on PD therapy [36]. The plausible hypothesis is, as aforementioned, impaired immunity against infection in diabetic subjects. An alternative explanation is that diabetic patients may have a more indolent presentation of peritonitis, which theoretically may result in delayed treatment and a dismal prognosis. Wang et al. showed that in dialysis patients, older age and diabetes mellitus are both risk factors for bacteremia, whereas diabetes mellitus and lower serum albumin are risk factors for bacteremia-associated mortality [37]. In line with their observation, our results underscore the importance of timely and aggressive management of peritonitis to prevent death in diabetic patients.
The International Society for Peritoneal Dialysis has published guidelines that provide comprehensive recommendations for managing PD-related peritonitis based on the best currently available evidence [4,38]. Catheter removal is indicated to prevent morbidity and mortality from refractory peritonitis and to protect the peritoneal membrane for future use. It should be emphasized that prolonged attempts to treat refractory peritonitis and to "save the catheter" are associated with an increased risk of fungal peritonitis and poor patient outcome [39]. In our experience, relapsing peritonitis is a controversial indication for catheter removal. Twelve (71%) of 17 episodes of relapsing peritonitis in this study showed considerable clinical improvement within 72 h of initiating therapy. These successfully treated episodes were either culture-negative or due to gram-positive organisms. Moreover, seven (58%) patients had no subsequent episodes of peritonitis. This is in keeping with the experience of others [40,41]. Our algorithm for the management of PD-related peritonitis is illustrated in Figure 5.
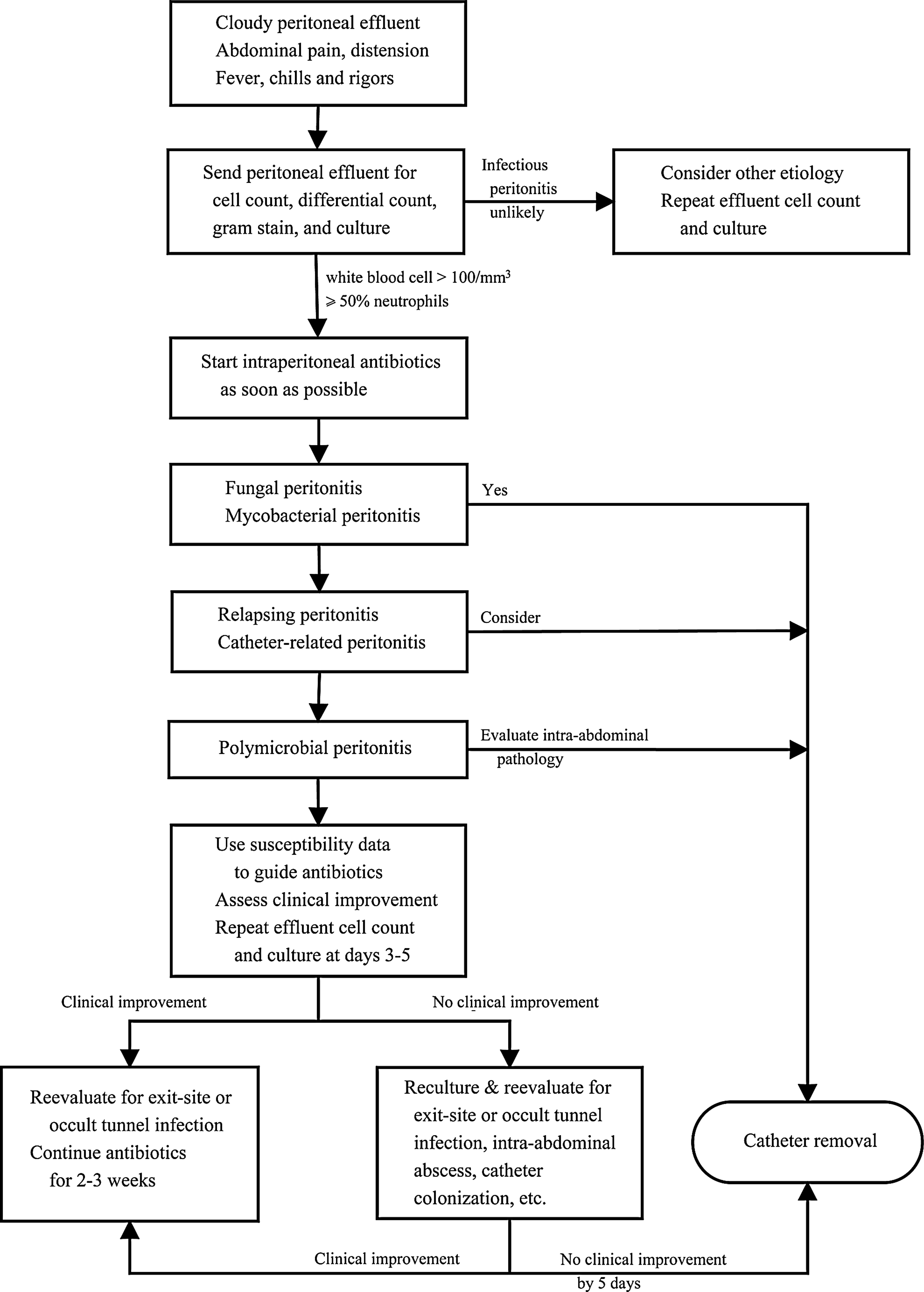
Algorithm for the management of peritoneal dialysis-related peritonitis. Relapsing peritonitis, an episode that occurs within four weeks of completion of therapy of a prior episode with the same organism or one sterile episode. Catheter-related peritonitis, peritonitis in conjunction with an exit-site or tunnel infection with the same organism or one site sterile (especially Staphylococcus aureus and Pseudomonas aeruginosa; except coagulase-negative staphylococci).
Although older age and diabetes mellitus are not modifiable patient-specific demographic characteristics, potentially modifiable risk factors for peritonitis have been identified [3]. The organism causing peritonitis provides an important clue to the etiology of the infection. Peritonitis episodes caused by Staphylococcus aureus and Pseudomonas aeruginosa are often secondary to exit-site and tunnel infections [3]. Skin organisms such as coagulase-negative Staphylococcus generally lead to peritonitis through contamination. Previously we found that patients developing Pseudomonas peritonitis have done poorly if the peritoneal catheter is not removed [42]. Gram stain may also indicate the presence of yeast, thus allowing for prompt initiation of antifungal therapy and permitting timely catheter removal. Based on our results, older age is associated with fewer gram-positive organisms, suggesting that the association between older age and poor outcomes is unlikely to be due to problems with exchange technique. Enterocolitis or constipation is associated with peritonitis caused by enteric organisms [3]. Elderly patients who have an impaired gastrointestinal barrier function may be more susceptible to translocation of enteric bacteria and peritonitis.
In conclusion, older age and diabetes mellitus are two major determinants of adverse outcomes of PD-related peritonitis. Older age is also associated with a higher risk of peritonitis. Although both factors are not contraindications to PD, our results suggest that these patients need more intensive and meticulous care when peritonitis occurs. Assessing for comorbidity and treating appropriately, and tight glycemic control are potential strategies to minimize the development and consequence of peritonitis.
Footnotes
Acknowledgments
We gratefully acknowledge the staff of the PD center at Mackay Memorial Hospital, whose careful management of the patients and great help with data registration allowed us to perform this study.
Author Disclosure Statement
No competing financial interests exist.