
Abstract
Abstract
Background:
Diagnosing infection efficiently is integral to managing critically ill patients. Knowing if and how trauma and general surgery patients differ in their presentation of new infectious complications could be useful. We hypothesized these populations would differ in presentation in the intensive care unit (ICU).
Methods:
We analyzed data collected prospectively from all 1,657 trauma and general surgery patients admitted to the surgical and trauma ICU (STICU) over a 21-month period. Clinical data from the first day of a newly diagnosed infection were compared for trauma (82% of the series) and general surgery (18%) patients.
Results:
A total of 10,424 STICU days were included, and 267 nosocomial infections were diagnosed. Trauma patients were younger (50 vs. 62 years; p<0.001) and more likely to be male (78% vs. 46%; p<0.001) than were general surgery patients. Similar percentages of the two groups were infected (11% and 13%, respectively), and infections occurred after a similar number of days in the STICU. The mean maximum temperature on the day prior to diagnosis was higher in trauma patients (38.4°C vs. 37.7°C; p<0.001), and the mean leukocyte count was lower (13,500 vs. 15,800 106/L; p=0.013). General surgery patients were more likely to be hypotensive (13% vs. 2%; p=0.002) and to have a positive fluid balance >2 L on the first day of infection (27% vs. 13%; p=0.02). Respiratory infections were more common in trauma patients (40% vs. 7%; p<0.001), and urinary tract infections were less common (19% vs. 36%; p=0.011).
Conclusion:
Differences exist in how new infections manifest in trauma and general surgery patients in the ICU. General surgery patients appeared sicker on their first day of infection, as evidenced by a higher leukocyte count, lower blood pressure, and substantial positive fluid balance. Intensivists may need differing thresholds for triggering infection workups when employed in a mixed unit.
H
Critically ill patients are at particular risk for nosocomial infections because of the number of devices used in their care [3]. Studies have shown critically ill surgical and trauma patients have higher rates of nosocomial infection than their medical intensive care unit (ICU) counterparts [4,5]. Therefore, prevention, early identification, and effective treatment of nosocomial infection is a goal for improving patient care in the surgical and trauma intensive care unit (STICU).
Diagnosing infection in a timely manner is often difficult in the STICU. Classically, fever and leukocytosis are considered to be heralds of infection. Yet, previous work looking into the sensitivity of fever and leukocytosis as predictors of blood, urine, or respiratory infection in the trauma population has questioned these relations [6–8]. This finding has been rationalized by attributing a patient's higher temperature and white blood cell (WBC) count to a robust non-infectious systemic inflammatory response syndrome (SIRS) secondary to traumatic injury, which can mask or mimic the presence of infection. Intensivists continue to struggle to define a reliable and efficient way to differentiate non-infectious from infectious SIRS.
At our institution, STICU attending physicians see both trauma and general surgery patients. We believe that a similar mixed rounding practice occurs at many institutions, although the exact number of combined STICUs in this country is unknown. There are currently 291 trauma centers (105 Adult Level 1) verified by the American College of Surgeons, and only 74 centers reported themselves as trauma ICUs in the latest National Healthcare Safety Network (NHSN) update [3,9]. Furthermore, the increasing prevalence of the acute care surgery (ACS) model of practice means that more surgeons will be caring for mixed populations of patients, especially at trauma centers. Studies by both Magret et al. and Hedrick et al. have shown differences in the outcomes of ventilator-associated pneumonia (VAP) in trauma and non-trauma surgical patients [10,11]. However, we are unaware of any studies that have looked specifically at differences if any in how a new infection presents in critically ill trauma and general surgery patients. For intensivists and other specialty surgeons charged with the care of both of these populations, it would be useful to know if and how trauma and general surgery patients differ in their presentations of a new infectious complication. We hypothesized that these two populations would show significant differences in clinical features collected on the first day of a new nosocomial infection in the ICU.
Patients and Methods
This study was reviewed and approved by the Metro Health Medical Center Institutional Review Board. A secondary analysis was performed on data collected prospectively on all trauma and general surgery patients consecutively admitted to a Level 1 urban trauma center's mixed STICU over a 21-month period (March 2007–November 2008). General demographic and clinical data, along with specific clinical features from the 24 h prior to a newly diagnosed nosocomial infection, were compared for the two groups. The first day of infection was defined as the date on which a positive culture was obtained from a patient. Therefore, all infections included were culture-confirmed. Additionally, all infections were confirmed clinically by an STICU attending physician and met the CDC guideline definitions for nosocomial urinary (UTI), respiratory, and blood stream infections [12]. Specifically, respiratory infections were diagnosed using cultures from tracheal aspirates or bronchoalveolar lavage. “Other” infection sites included wounds, incisions, intra-abdominal, sinus, and meninges. Infections contracted outside the STICU or on ICU day 1 were excluded.
The STICU attending physician caring for the patient at the time of culture made the decision whether to start or withhold empiric antibiotics on the day of culture. The details of this clinical decision were not the focus of this study and are not discussed here.
Data were collected from an internal clinical research database, SIC-IR®. The SIC-IR® database has been validated as an accurate clinical documentation tool and robust research database [12,13]. All patients admitted to the STICU are entered prospectively in this database. The database is updated daily with clinical data. The temperature is the maximum temperature recorded in the previous 24 h. Vital signs, including heart rate (HR), respiratory rate (RR), blood pressure (BP), oxygen saturation (SpO2), and central venous pressure (CVP), are collected by the resident on morning rounds (typically 6–7
Data were analyzed using SPSS, version 19 (SPSS Inc, Chicago, IL). A p value ≤0.05 was considered statistically significant. Numeric data are expressed as mean±standard error of the mean and compared using the Student t-test after evaluation with a Levene test for equal or unequal variance. Categorical data were described as a percentage and compared using either a χ2 or Fisher exact test as appropriate.
Results
Our analysis included 1,657 critically ill trauma and general surgery patients, who accounted for 10,242 total STICU days. Eighty-two percent of the patients (n=1,359) were trauma admissions. One hundred seventy-five patients were found to have 267 nosocomial infections. There was no difference in the rate of new infections in trauma vs. general surgery patients: New STICU infections occurred in 11% of trauma patients and 13% of general surgery patients. Patient demographics are shown in Table 1, which demonstrates significant differences between the two cohorts. Trauma patients were younger than the surgery patients and more likely to be male.
Trauma patients were five times more likely to have a respiratory infection, and general surgery patients were twice as likely to have UTIs (Fig. 1). Rates of UTI were significantly higher in male general surgery patients than in male trauma patients (31% vs. 13%; p=0.04). The UTI rates were similar in female general surgery and trauma patients.
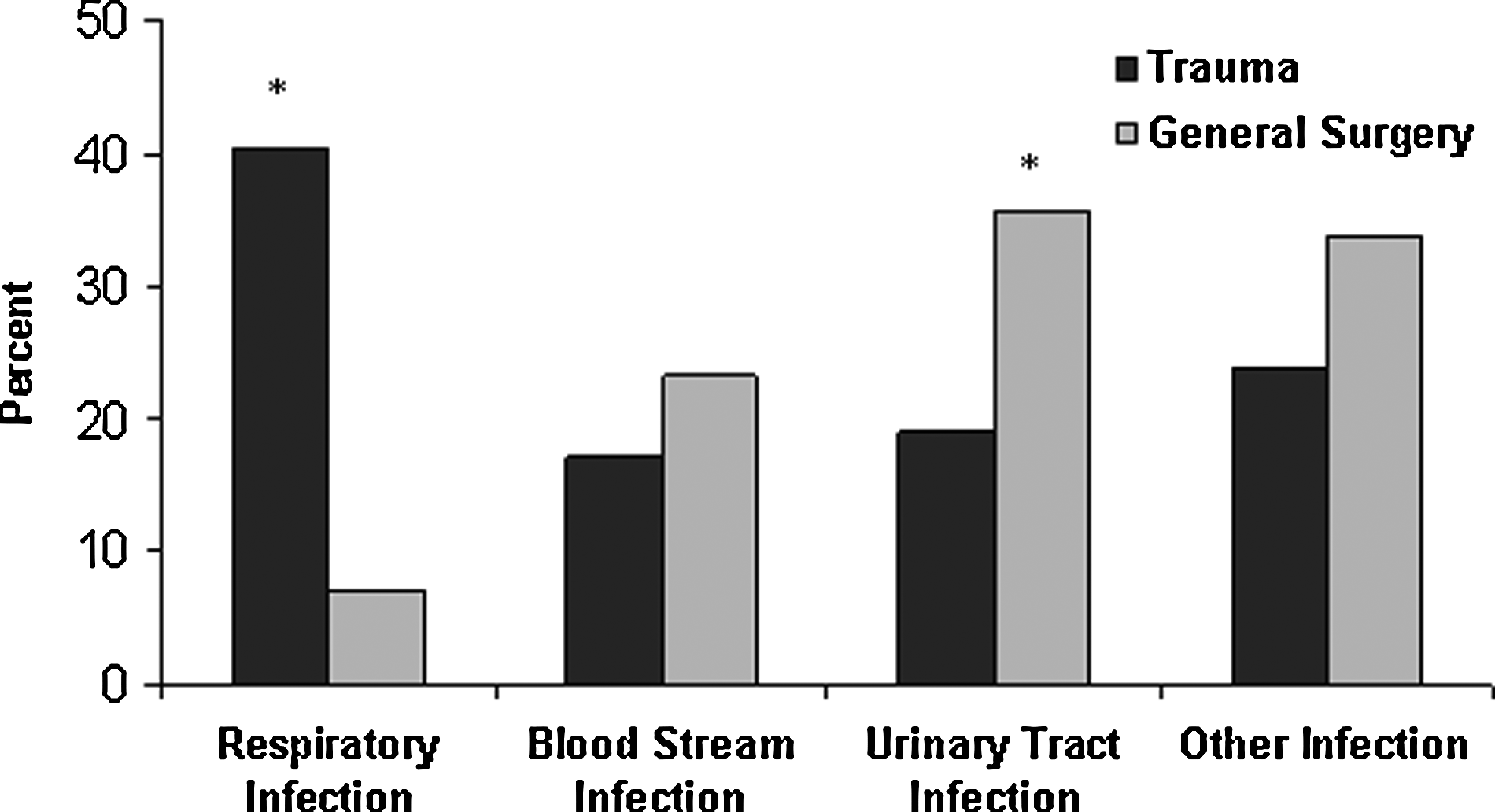
Prevalence of respiratory, blood stream, urinary, and other infections among critically ill trauma and general surgery patients in the surgery and trauma intensive care unit found to have a new nosocomial infection. Note that the Y axis goes only to 50%. *P≤0.5.
Table 2 illustrates the usage of invasive devices, corticosteroids, and blood products on the first day of a newly diagnosed infection. The majority of both populations were on a ventilator, and the mean number of ventilator days at the time of infection diagnosis was similar. Urinary catheters were present in every infected trauma patient and most general surgery patients. Again, the number of urinary catheter days was similar. More general surgery patients had a central venous catheter in place and a greater number of central venous catheter days at the time of diagnosed infection. A significant increase in corticosteroid use was observed in the general surgery patients. Similar percentages of patients in the two groups received blood products on the first day of infection.
Mean±standard deviation.
Trauma and general surgery patients spent similar amounts of time in the STICU before being found to have an infection, 13 days vs. 15 days, respectively (p=0.266). Table 3 shows the measured clinical features during the 24-h period before a newly diagnosed infection. Trauma patients had a significantly higher maximum temperature (38.4°C vs. 37.7°C; p<0.001). When temperature was considered as a categorical variable based on the SIRS criterion of 38.0°C, significantly more trauma patients met this criterion. The absolute fluid volumes were similar in the trauma and general surgery patients. However, fluid balance was significantly different, with more general surgery patients having a balance of >2 L in the 24 h prior to the diagnosis of an infection. General surgery patients had a higher mean WBC count on the first day of infection (p=0.013). When the SIRS criterion WBC >12,000×109/L was considered as a categorical variable, there was no difference between the two populations.
Mean±standard deviation.
On the first day of diagnosed infection, antibiotics were being given to 50.2% of trauma patients and 60.7% of general surgery patients (p=0.178). The STICU length of stay was similar for trauma and general surgery patients who developed infections, at 28 and 30 days, respectively (p=0.719).
Discussion
To our knowledge, this is the first study to examine whether there are differences in the clinical presentation of a newly diagnosed nosocomial infection in critically ill trauma compared to general surgery patients. It is important to emphasize that the critically-ill trauma and general surgery patients in our study had many differences. The trauma population was younger and predominantly male. Furthermore, this study demonstrated that these two populations show significant differences in how they present when newly infected. This finding has not been noted in the literature previously.
The infected trauma patients had a higher mean maximum temperature (38.4°C vs. 37.7°C) and were more likely to meet the SIRS temperature criterion of >38.0°C than infected general surgery patients. Previous work has shown that between 50% and 69% of trauma patients meet SIRS criteria during their second and third weeks post-injury [14]. However, it was surprising that the mean temperature found in this study was not higher in these infected trauma and general surgery patients. Our STICU practice defines febrile as ≥38.5°C, so the majority of these infected patients did not present with fever. Although studies have examined the sensitivity and specificity of fever when looking for infection, there is no work looking specifically at the likelihood of fever in confirmed infection [6–8]. Many of the infections included in this study occurred after two weeks in the STICU. The infected general surgery patients seem even less able to mount a fever. Perhaps this is related to their greater age and their pre-hospitalization health status.
Infected general surgery patients appeared sicker on the first day of a newly diagnosed infection. First, they had a lower mean maximum temperature, and as reviewed by Barone, the absence of a fever actually may be a poor prognostic indicator [16]. They also had more significant leukocytosis than their trauma counterparts (15.8×109 vs. 13.5×109L, respectively). Finally, critically ill general surgery patients had lower blood pressure and were more likely to have a >2 L fluid balance over the previous 24 h. We were unable to find other literature commenting on these clinical differences.
In addition to presenting differently, trauma and general surgery patients contract different nosocomial infections while in the STICU. Thus, the trauma patients were five times more likely to develop a respiratory infection despite having spent a similar number of days on a ventilator. This finding correlates well with the increased risk of pneumonia secondary to aspiration, emergency airway management, and chest trauma described previously [16,17]. Male general surgery patients were more likely to get UTIs despite a lower percentage having catheters in place. The population's greater age and female predominance may account for this increase, as older patients and women have higher rates of bacteriuria [18]. The general surgery patients had significantly more central line days. However, they did not have a higher rate of blood stream infections.
Interesting similarities were found between our newly infected STICU trauma and general surgery patients. Although the predominant types of infection were different, the ICU day of infection was similar for the two groups. Additionally, the STICU lengths of stay were similar. Although we do not have Acute Physiology and Chronic Health Evaluation scores for these patients, the similarly long STICU stay highlights that both of these populations were very ill.
In our study, the morning blood glucose concentration was not significantly different in the two populations. Previous studies have identified glucose control and the use of blood products as important risk factors for infection [19,20]. However, we did not look at the use of insulin to control serum glucose. There was no difference in blood products transfused on the first day of infection. However, we did not specifically compare the volumes or types of products transfused. In a further study, it would be interesting to look at the particular types of blood products used and the total volumes of blood products received by both populations prior to infection.
This study is limited by its retrospective design and the corresponding inability to understand all of the clinical conditions and decisions that led to events, such as culturing and the use of steroids and blood products. However, the prospective data collection involved mitigates the selection bias often seen in retrospective studies. Our database does not provide information regarding the physician's decision-making process. Therefore, we are unable to infer why a physician chose to culture a patient. In future prospective studies, we hope to investigate the clinical reasoning involved in and the effectiveness of these decisions. Additionally, this study did not aim to identify which patients were infected, nor did it address the ability of individual factors to predict which patients are infected.
In conclusion, this study highlights differences in how new infectious complications present clinically in trauma and general surgery patients. Routinely collected clinical data demonstrated that the general surgery patients appeared sicker on their first day of infection, as evidenced by higher WBC count, lower blood pressure, and a significantly positive fluid balance. These findings demonstrate that an intensivist may need differing thresholds for triggering an infectious workup in a mixed patient unit. As we work to our ultimate goal of improving our efficiency of diagnosing infections in the ICU, this study demonstrates that the type of patient (trauma vs. general surgery) should be a key factor in our clinical reasoning.
Footnotes
Author Disclosure Statement
None of the authors has any financial conflicts of interest to disclose.