
Abstract
Abstract
Background:
Anastomotic leak after rectal resection carries substantial morbidity and mortality. A diverting ileostomy is beneficial for high-risk anastomoses, but its creation and reversal carry a surgical risk in addition to that of resection itself. We sought an alternative method for managing complications of rectal anastomosis.
Methods:
We developed an endoluminal negative-pressure technology with a diverting proximal sump, and hypothesized that it would close anastomotic disruptions in pigs. We performed rectal resections on pigs, with primary anastomoses and the creation of an anastomotic defect. In animals in the treatment group we inserted an endoluminal negative-pressure device and kept it at a low level of continuous suction for 5 d. No device was inserted in a control group of animals. After the 5-d period of treatment we evaluated the anastomoses in both the treatment and control groups of animals for leakage, using contrast enemas. Specimens of anastomosed rectum were evaluated histologically for mucosal integrity and for the location and density of inflammatory responses.
Results:
Fourteen pigs were assigned to either the treatment (n=10) or control (n=4) group. Of the pigs in the treatment group, 90% had complete closure of their rectal defect, as compared with 25% of the animals in the control group (χ2 test, p=0.04). The animals in the treatment group had only minimal mucosal and serosal inflammation, whereas those in the control group had extensive mucosal damage with associated serositis.
Conclusions:
Endoluminal negative-pressure therapy was well-tolerated and led to successful closure of 90% of the anastomic rectal defects in the treatment group of animals in the present study. Additional evaluation of this therapy is warranted.
C
Anastomotic disruption is a dreaded complication of colorectal surgery, leading to increases in re-operation rates, hospital lengths of stay, cancer recurrence rates, morbidity, and mortality [4–6]. Anastomotic leaks may result in abscesses, enterocutaneous fistulae, severe sepsis, and peritonitis. Although the reported overall rate of leaks in colorectal anastomoses ranges from 2.4%–12%, a markedly higher rate of anastomotic disruption, of 8%–24%, occurs in lower rectal anastomoses [5,7–10]. Proximal diversion through loop ileostomy or transverse colostomy does not prevent anastomotic leaks and is therefore not commonly used other than for high-risk anastomoses [7,9]. Classic management of an anastomotic leak requires laparotomy and resection or reinforcement of the anastomosis, with proximal diversion or creation of a Hartmann pouch [5]. A proximal diversion without resection of the leaking anastomosis may be a safe alternative [9,11]
Regardless of the technique used for its management, an anastomotic leak requires additional surgical procedures in both the short-term and remotely to restore bowel continuity, with each surgical procedure incurring additional morbidity and surgical risk. Morbidity is also associated with enterostomies, and loop ileostomies carry among the highest rates of stomal morbidity [12]. We therefore sought an alternative to the surgical management of anastomotic leaks in the rectum.
Morykwas et al. introduced negative-pressure therapy in 1997 as a method to expedite healing by secondary intention [13]. They conducted multiple animal experiments involving the introduction of their vacuum-assisted closure (VAC) device with a foam dressing, adhesive drape, and controlled subatmospheric pressure to accelerate wound healing. They found that the VAC technique increased local blood perfusion, accelerated granulation-tissue formation, decreased tissue bacterial loads, and increased nutrient blood flow [13,14]. Additionally, VAC therapy decreases local inflammation [15].
Vacuum-assisted closure devices now have numerous clinical applications and have recently been used in treating pre-sacral and para-anastomotic rectal abscesses. The Endo-SPONGE (B. Braun Medical, Melsungen, Germany), a VAC device commercially available in Europe, is effective in closing abscess cavities resulting from anastomotic leakage without the need for re-operation [16–21]. The technique for this uses an endoscope to reach the abscess cavity, a plastic introducer tube, and pushing probe to deploy the Endo-SPONGE into the abscess cavity while the plastic tube is retracted [16]. The technique requires exchange of the device every 3 –4 d and approximately one month for full resolution of the cavity.
Our study proposed a novel technique in which a negative-pressure closure device placed within the bowel lumen is used to heal anastomotic leaks in the rectum following a low anterior resection. This endoluminal technique also provides a proximal sump port to eliminate waste. We conducted a non-randomized, controlled trial in a pig survival model to test the use of endoluminal negative-pressure therapy for the healing of anastomotic leaks following rectal resection and for reducing leak-related morbidity by reducing rates of intra-abdominal sepsis. Our secondary endpoint was to evaluate mucosal integrity and inflammation at the leak site.
Materials and Methods
The Institutional Animal Care and Use Committee (IACUC) at the University of Virginia approved the study. Our protocol ensured the appropriate care, use, and humane treatment of the animals being used for research in accordance to the Animal Welfare Act of 1966 (as amended in 1990) and the Guide for the Care and Use of Laboratory Animals [22, 23].
Pig characteristics and operative preparation
Our study used 14 female Yorkshire pigs (60 lb–80 lb each). Upon arrival in our vivarium, pigs were kept under standard husbandry conditions, fed a Teklad 7037 Miniswine diet (Harlan Laboratories, Indianapolis, IN) and allowed to acclimate for 72 h. Food was withheld for 48 h before surgery and pigs were provided ad libitum access to drinking water containing sucrose at 50 g/L. At 24 h before surgery pigs were given 24 fluid ounces of magnesium citrate either in their drinking water or via gastric intubation under brief anesthesia for preoperative bowel preparation and washout.
Anesthesia and surgical approach
On the day of surgery anesthesia was induced in the study animals with intramuscular (IM) xylazine 2 mg/kg and telazol 6 mg/kg. When the animals were in the recumbent position for surgery, they were given glycopyrrolate IM at 0.01 mg/kg, long-acting tetracycline (LA-200, Pfizer, New York, NY) IM at 9 mg/kg, and enrofloxacin (Baytril 100, Bayer, Morristown, NJ) IM at 7.5 mg/kg. The animals were intubated, maintained under anesthesia with 2.5% isoflurane in oxygen, and monitored with standard cardiopulmonary monitoring. Warm lactated Ringer's solution (LRS) was administered intravenously (IV) during surgery at 5 mL/kg/h and animals were placed on a circulating-warm–water blanket to prevent hypothermia. The neck, back, and abdomen of each animal were shaved and the skin prepared for aseptic surgery. A transdermal fentanyl patch (75 mcg/h) was placed on the thoracic skin and 0.3 mg buprenorphine IV was administered once. The pigs were prepped and draped in the usual sterile fashion and an indwelling silastic catheter (0.062” ID x 0.125” OD) was implanted in the internal jugular vein and tunneled subcutaneously to exit caudal to the ipsilateral scapula. A midline lower abdominal incision was then made and the peritoneal cavity was entered sharply. The rectosigmoid colon was mobilized and approximately 5 cm of rectum was resected in the standard fashion. The distal colon was primarily re-anastomosed to the rectum using a curved 21-mm ENDOPATH endoscopic intraluminal circular stapler (Ethicon Endo-Surgery, Inc, Cincinnati, OH). A 2-cm defect was then made sharply in the staple line in each pig, leaving a visible gap in the colorectal anastomosis (Fig. 1).
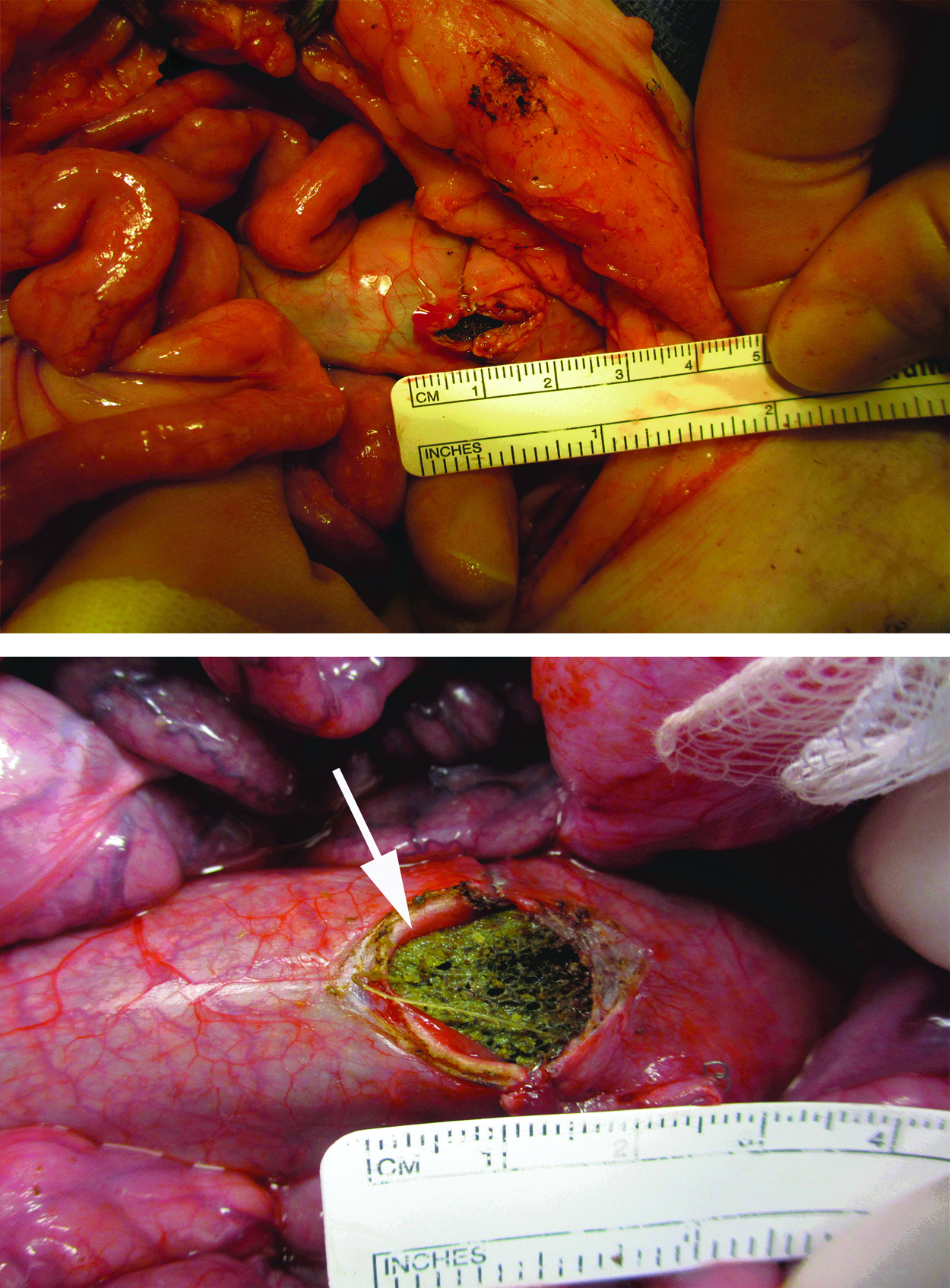
After rectal resection and stapled anastomosis, a 2-cm enterotomy was made in the staple line in all of the pigs in the study. In the treatment group of pigs, the negative-pressure device was placed across the defect. A portion of the device can be seen through the defect (arrow). Color image is available online at www.liebertpub.com/sur
The pigs were assigned to either the study or the control group. Before surgery on each pig was begun, it was scheduled to facilitate the availability of necessary equipment, including suction and fluoroscopy equipment. Pigs in the study group underwent placement of a negative-pressure system with a dual-chamber sump (Fig. 2). This was made with black GranuFoam (Kinetic Concepts, Inc, San Antonio, TX) arranged cylindrically around 16-French sump tubes (Bard Medical, Covington, GA). The negative-pressure system was placed manually into the rectum of each animal in the study group, across the site of anastomosis. The proximal sump port terminated in the colon proximal to the site of anastomosis, and was connected to a suction unit at negative pressures of 5–140 mm Hg. The distal vacuum port terminated within the GranuFoam sponge and was connected to a separate vacuum system with negative pressures of 5–140 mm Hg. The tubing exited into the perirectal tissues and was tunneled subcutaneously and exteriorized posterior to the scapula. This was done to facilitate minimal restraint of the animals. The anus was sewed shut with silk suture. The abdomen of each pig was closed with running sutures of #1 polydiaxinone and the skin was closed with staples.
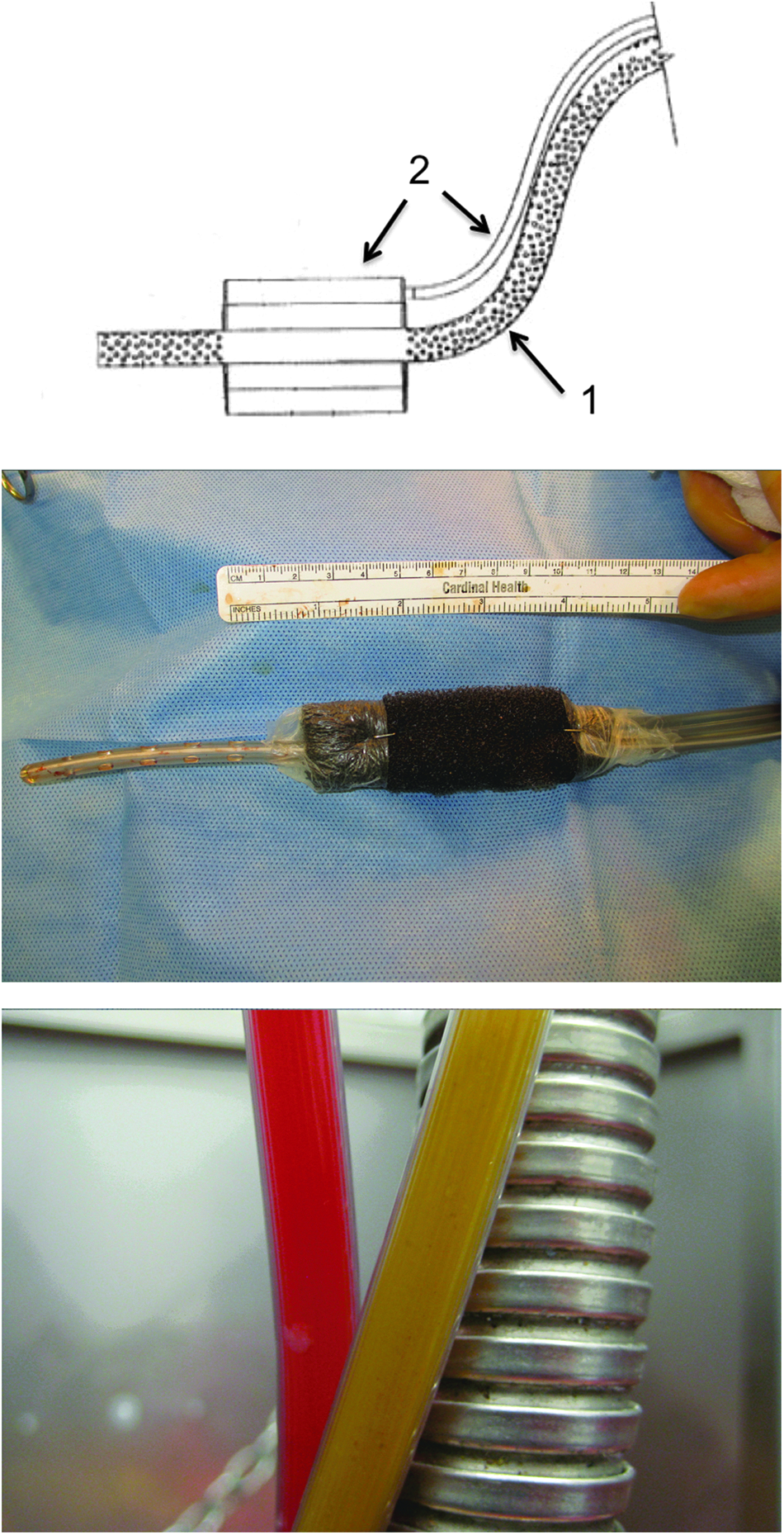
Top: Schematic diagram of the endoluminal negative-pressure device, illustrating the proximal sump (arrow 1) and the vacuum device with its separate vacuum tubing (arrow 2). Middle: Photograph of the negative-pressure device ex vivo, showing black Granufoam, adhesive moisture barrier, and sump and vacuum tubing. Bottom: Photograph of the external portion of the tubing system of the device, showing fluid drained by the vacuum sponge (red) and fluid from the proximal fecal sump (yellow-brown). Color image is available online at www.liebertpub.com/sur
Postoperative care
Postoperative continuous total parenteral nutrition (TPN) and LRS was given to the study animals via a central line. The animals' resting energy requirement (RER) was calculated as 35 kcal/kg/day, with 80% of their calories provided by fat (Liposyn II, Hospira, Lake Forest, IL) and 20% by glucose (50% glucose, Butler-Schein, Melville, NY). Amino acids were supplemented at 4 g/100 kcal/d (10% amino acid, Aminosyn-sulfite free, Hospira) and the potassium concentration of the infusate was adjusted to 30 mEq/L. Total parenteral nutrition was given at a rate calculated to deliver the animals' RER over a period of 24 h and LRS was provided at 1 mL/kg/h. Serum biochemistry analyses was done on post-operative days 1 and 5 to assess hepatic and renal function and to determine whether the animals were hydrated adequately. During the period between surgery and euthanasia, the study animals were placed in a harness (Lomir Biomedical, Malone, NY) with a conduit to protect IV and vacuum lines, and their motion was restrained partly with a harness that prevented them from turning but allowed them to stand and move with restriction in an 18 ft2 elevated run. The pigs were tranquilized twice daily with a combination of 5 mg diazepam/10 mg acetylpromazine IV to facilitate measurement of their temperature, pulse, and respiration, and their physical examination by members of the veterinary staff. Pigs exhibiting signs of peritonitis, which included tachycardia (heart rate [HR]>150 beats/min), peritoneal signs, fever (>103.5 °F), or discomfort that was not relieved with fentanyl or buprenorphine, were removed from the study and euthanized.
Macroscopic evaluation
Pigs were weighed pre-operatively and after euthanasia. On post-operative day 5 pigs were euthanized with Euthasol (Virbac, Fort Worth, TX), the endoluminal negative-pressure system was removed in the study group, and post-mortem lower GI fluoroscopy with contrast (50% Hypaque, diluted 1:5; Amersham Health, Princeton, NJ) was done and recorded on an OEC 8800 C-arm fluoroscope (GE Medical Systems, Salt Late City, UT). At necropsy, the animals' exploratory laparotomies were re-opened and the peritoneal cavity examined for evidence of peritonitis, abscess, anastomotic fistulae, and adhesions.
Histopathology
The sites of rectal anastomosis in each animal were excised and fixed in formalin. The specimens were dissected, and sections of the enterotomy site, uninvolved rectum, and any areas of atypical appearance were taken for examination. The sections were embedded in paraffin, cut at 5-mm intervals with a standard microtome, mounted on slides, and stained with hematoxylin and eosin (H&E). The slides were evaluated by a pathologist (M.M.) for mucosal integrity, overall inflammatory response, and the presence of serositis, mucosal necrosis, and fibrinous adhesions. Inflammatory response was evaluated adjacent to the enterotomy site and graded as mild, moderate, or severe, with mild representing increased mucosal inflammation, moderate representing increased inflammation with loss of mucosal crypts, and severe representing complete absence of crypts. Serositis was scored as mild if minimal serosal inflammation was present and as moderate if inflammation and fibrinous adhesions were seen. Adhesions to any adjacent abdominal organs were recorded. The pathologist was blinded as to which specimens came from pigs in the control and which from pigs in the treatment group of the study.
Statistical analysis
The study was a feasibility study and its original intent was not to provide statistical significance but to evaluate the feasibility of using the endoluminal negative-pressure device investigated in the study. The study was not statistically powered a priori. The Fisher exact test was used to calculate statistical differences in the frequency of leaks in the control and treatment groups in the study.
Results
Gross evaluation and fluoroscopy
Ten pigs had an endoluminal negative-pressure device placed colorectally and were part of the experimental group. All 10 tolerated 5 d of therapy. Nine of these animals had complete closure on post-mortem fluoroscopy (Fig. 3). One had a contained leak near the site of anastomosis, with a 5-cm abscess on necropsy. We did not see any leak on gross necropsy in the nine pigs with complete healing (Fig. 4). In seven pigs, a scar was seen at the anastomosis, with complete apposition of rectal mucosa. No physiologic narrowing of the lumen was seen on fluoroscopy. In two cases, adjacent structures (bladder, fallopian tube, ovary) had formed a flap over the anastomotic site to create the seal (Fig. 5).
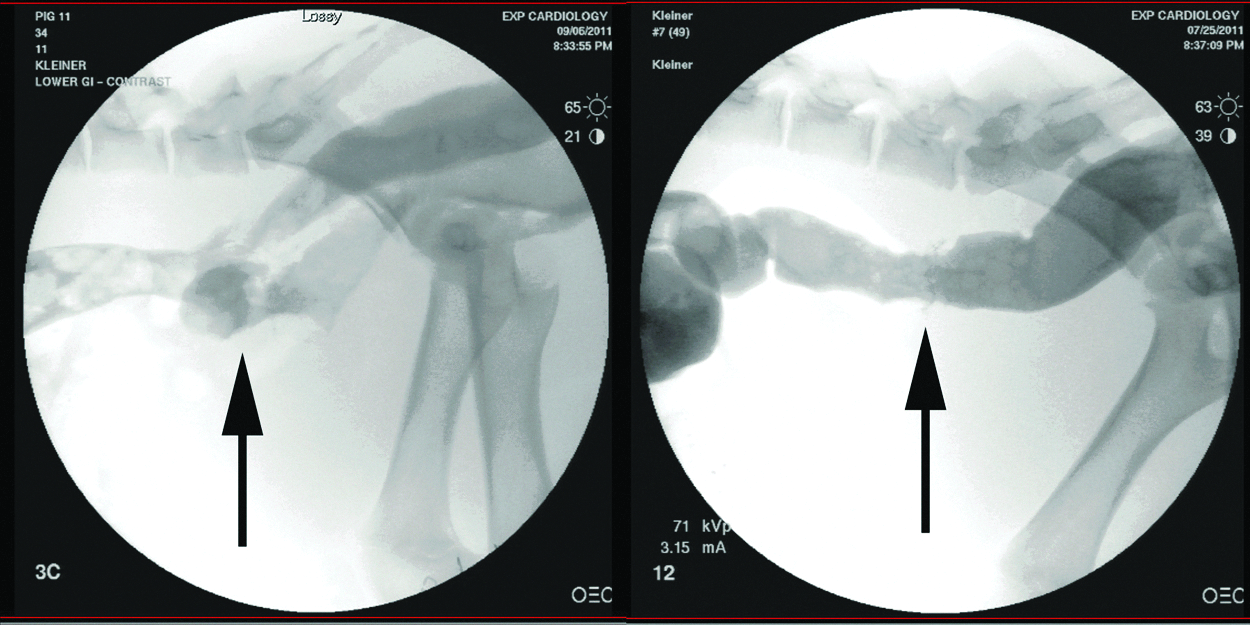
Left: Representative fluoroscopic image of rectal anatomosis in a control pig. Contrast medium flows freely from the site of anastomosis (arrow) into the pelvis. Right: Contrast-enhanced fluoroscopic image of anastomosis in a pig in the group treated with the endoluminal negative-pressure device, showing an intact rectal anastomosis.
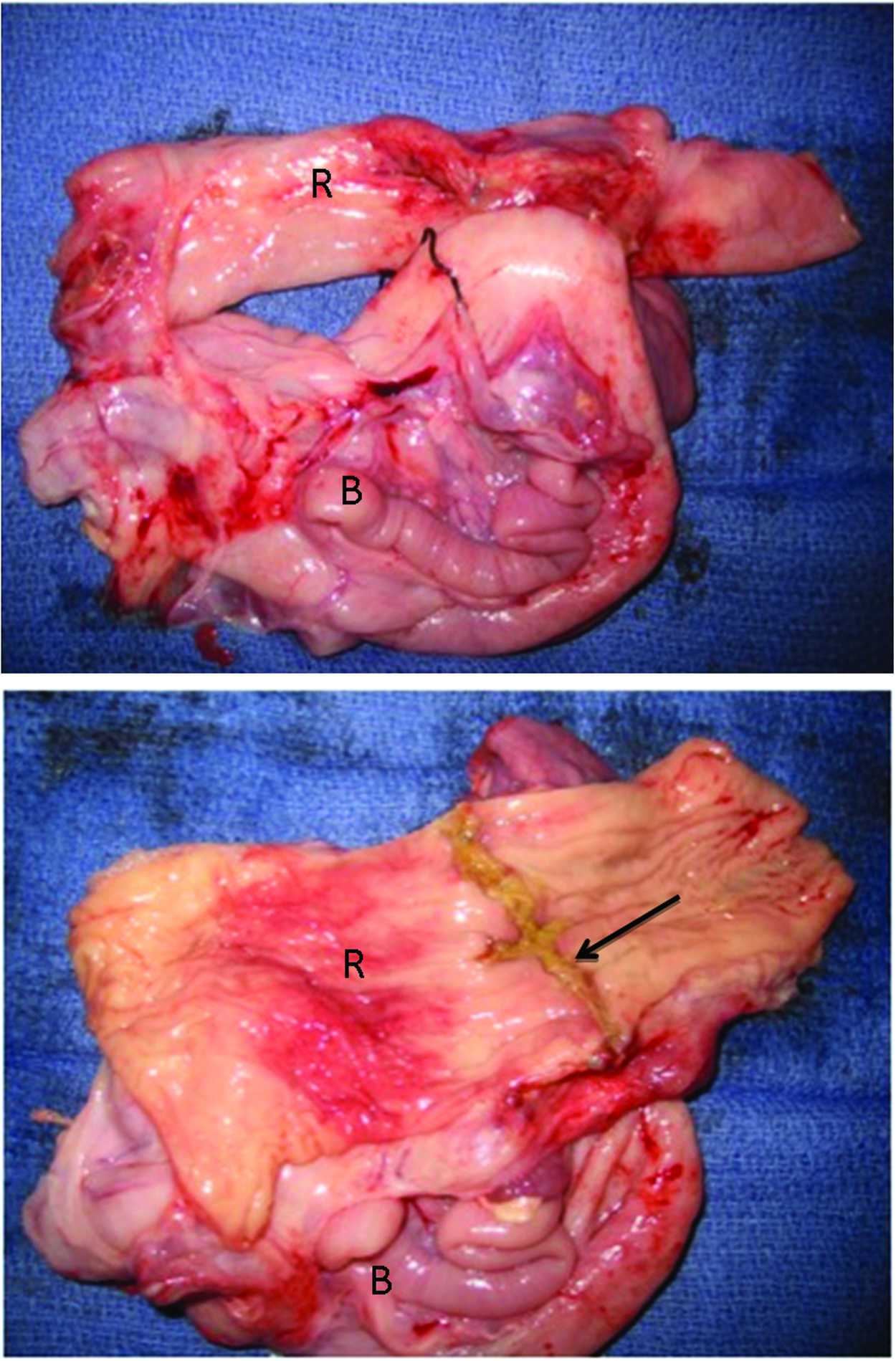
Top: Gross necropsy of specimen of rectum (R) with adjacent bladder (B). Bottom: The specimen is shown after lengthwise opening, revealing an intact anastomosis (arrow). Color image is available online at www.liebertpub.com/sur

Top row: Gross histology demonstrating the rectum with adjacent, adherent fallopian tube (on left). On the right, the rectum is opened lengthwise to reveal an intact anastomosis, with a flap of adjacent serosa as a patch. Bottom row: Adhesion of rectum to surrounding abdominal organs (H&E, 20× magnification). Fibrinous adhesion of the enterotomy site and surrounding rectum to various abdominal organs was observed in both control and experimental pigs, including bladder
The four pigs in the control group did not undergo endoluminal negative-pressure therapy. Three of these pigs had a leak at the site of anastomosis on fluoroscopy and turbid fluid in the abdomen on necropsy (Fig. 3). Two of these three pigs contained leaks with abscesses adjacent to the anastomoses. One pig had an uncontained leak, with free enteric contents in the abdomen. Three of the four pigs had to be removed from the study due to signs of sepsis. Thus, the p value for post-operative leak in this pilot study is 0.04.
Weight and laboratory tests
Control pigs weighed an average of 27 kg at the beginning of the study and 28 kg at its conclusion. The mean weight of the pigs in the treatment group was 30 kg at both the beginning and the end of the study. The white blood cell (WBC) count in the control group averaged 10.9 k/mm3 at the beginning, and increased to 19.1 by the end of the study. WBC count in the experimental group averaged 18.8 k/mm3 at the beginning and 26.7 k/mm3 at the end of the study. Serum biochemical analysis found no significant difference between the control and treatment groups during the study.
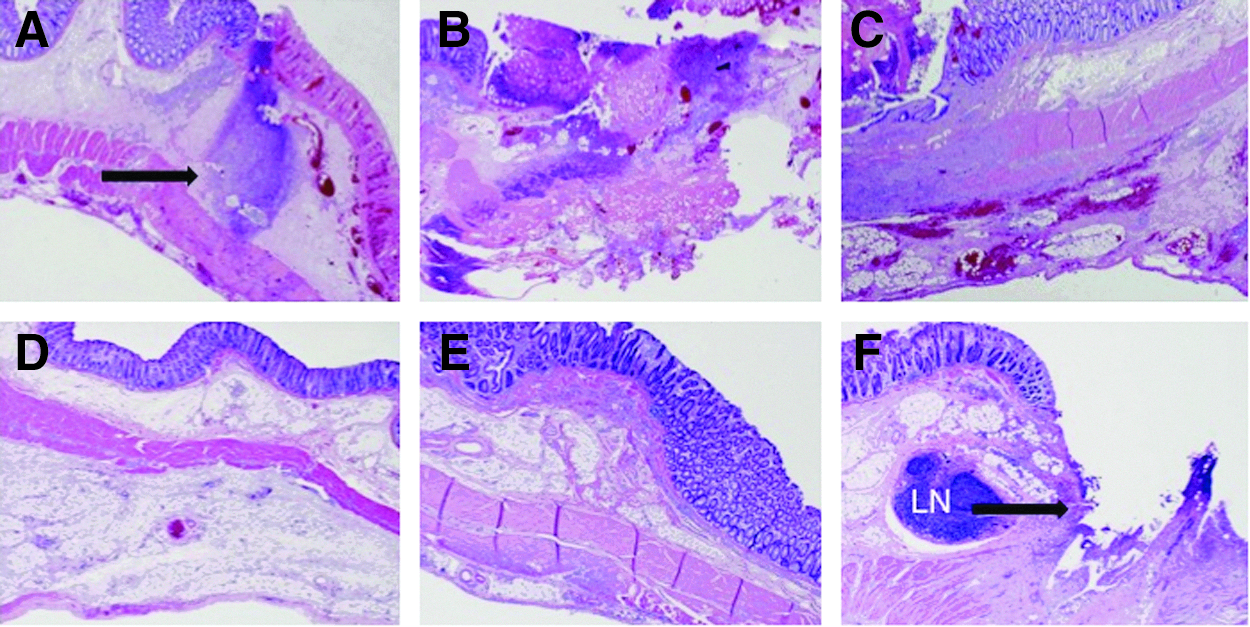
Histopathology
Representative histology specimens from both the treatment and the control groups are shown in Figure 6. All enterotomy sites showed standard microscopic reparative changes, including increased acute and chronic inflammation and granulation tissue with early scar formation. Use of the endoluminal device was associated with decreased rates of mucosal inflammation and crypt dropout in the treatment as compared with the control group (26% vs. 75%, respectively), decreased rates of prominent serositis (46% vs. 75%, respectively), and decreased ischemia/mucosal necrosis adjacent to the enterotomy site (27% vs. 100%, respectively) (Table 1). Fibrinous adhesions with involvement of surrounding abdominal organs (bladder, ovary, and fallopian tubes) were seen frequently in both the treatment and control groups (64% vs. 75%, respectively ). One pig in the control group that was found to have a leak showed extensive microscopic damage to the rectum, including extensive necrosis and prominent submucosal hemorrhage.
VAC=vacuum-assisted closure device.
Discussion
The study described here examined in a prospective manner the ability of endoluminal negative-pressure therapy to close leaks in colorectal anastomoses. Endoluminal negative-pressure therapy was well tolerated in the pigs in which it was examined in the study, and successfully closed 90% of colorectal anastomoses in the study subgroup of animals in which it was used. The leaks created in these animals ranged in size from one-third to one-half of the bowel lumen, and were found to have healed fully on fluoroscopic examination and necropsy. None of the animals undergoing negative-pressure wound therapy had signs of intra-abdominal infection. Animals in the control group did not do as well, as we expected in view of their large untreated enterotomies. The frequency of leaks in the treatment group as determined fluoroscopically was significantly lower than that in the control group, even in this small pilot study.
We propose the use of a negative-pressure device to assist the healing of colorectal anastomoses expected to carry a high risk of post-operative leakage. A diverting proximal stoma, although protective against morbidity after rectal surgery, also creates issues of morbidity, cost, and quality of life for the patient. As is a diverting ileostomy, a negative-pressure device would be used to prevent a potential leak from becoming clinically important. We believe that use of a post-operative endoluminal negative-pressure device may serve as a prophylactic measure in high-risk colorectal anastomoses, and could potentially replace diverting loop ileostomy in select cases. This could change the way in which rectal surgery is performed, and provide a means of preventing and managing the complications of anastomotic leaks without the need for a diverting ostomy.
In this study we chose to create artificially an incomplete staple line because we believed that closing a known leak would more reliably demonstrate, in a smaller group of animals, the success of the device examined in the study. An alternative study design, with the negative-pressure device examined in the study placed in an intact anastomosis, would find a probable leak rate of 15% (as estimated from the rates of leak after low anterior resection), and would thus require a larger study population. The small sample size and non-randomized design of the present study permit only preliminary conclusions to be drawn from the study data, and a larger scale study will be beneficial. The method in which the device was inserted in the pigs in the present study (tunneled subcutaneously, exiting through perianal tissue) was part of the study design largely because pigs scratch their perianal areas and would otherwise dislodge the device with their movement. We do not anticipate these issues with human studies, in which we intend to have the negative-pressure device examined in the present study exit just as would a rectal tube. With the vacuum suction applied to the device, it undergoes virtually no migration. This is similar to the case with commercially available negative-pressure systems for wound therapy. We also do not anticipate that human studies would include the need for TPN and NPO. We used TPN in the pigs in the present study because they were young and growing, and unable to tolerate being NPO for several days, in contrast to adult human beings following surgery.
Grossly and histologically, we saw adhesions between the rectum and adjacent structures after anastomosis in the animals in our study. Published data link negative-pressure therapy to the formation of enterocutaneous fistulas. This is of concern in view of the morbidity associated with rectovaginal and rectovesicular fistulas. The minimal inflammation seen on histology in our study animals is somewhat reassuring, indicating that use of the negative-pressure device examined in the study is a potentially inconsequential process. Additionally, there was no difference in the rate of formation of adhesions in the control and treatment groups in our study. This finding is reassuring, but this issue bears further investigation in follow-up studies.
Anastomotic leak continues to be a substantial cause of morbidity and mortality after rectal surgery. Risk factors for anastomotic complications include rectal operations, patients with several co-morbidities, radiation, immunosuppression, and emergency surgery [4,10]. Anastomotic leaks in cancer patients undergoing colorectal surgery are also associated with decreased cancer-specific survival as well as local recurrence of disease [6,22]. There are obvious differences between high-risk anastomoses in human beings, such as those in patients in whom irradiation of the pelvis is used in treating rectal cancer. This factor has not been addressed with our current model, and further evaluation of anastomoses created after irradiation is needed for examination of their histologic and other features.
The present study has shown that 5 d of endoluminal negative-pressure therapy assists the closure of anastomotic leaks. This pilot study did not evaluate the long-term durability of rectal anastomoses after endoluminal negative-pressure therapy. To begin assessing the durability of these anastomoses after removal of the negative-pressure device, we conducted a follow-up “survival” study of the anastomoses created in the study at 14 days after removal of the device. In this follow up we studied two pigs with the protocol described in the Methods section of this paper, but rather than performing euthanasia and necropsy on post-operative day 5, we allowed the pigs to resume eating for 14 d after removal of the negative-pressure device. We then performed repeat fluoroscopic evaluations at 14 d after removal of the pigs' devices and found that neither pig had a leak or narrowing of their anastomosis on fluoroscopy. The duration of application of the device needed for complete healing is not known, and may vary with the individual patient. In our study the device was placed transrectally with direct visualization. Conceivably, the device could also be placed endoscopically, allowing replacement if it became dislodged or dysfunctional during the course of treatment. This was not attempted in the present study.
Previous studies have evaluated use of negative-pressure wound therapy in the healing of anastomotic leaks. Several studies have evaluated the Endo-SPONGE system [20,21], and another study, by Mees et al., examined an endovacuum assisted-closure device that significantly accelerated wound healing after colorectal surgery [17]. Patients treated with the devices described in these studies required diverting ostomies before the devices were placed. In contrast, our study evaluated the use of endoluminal therapy rather than diversion with the use of a proximal stoma.
We conclude that endoluminal negative-pressure therapy is feasible and safe in an animal model. This therapy was successful in closing anastomotic defects in 90% of the animals in which it was used in our study. Even in this small population, the rate of anastomotic leak was significantly lower with use of the endoluminal device. Additional evaluation of endoluminal negative-pressure therapy is warranted in a larger study, and examination in human clinical trials of the device described in the present study is warranted.
Footnotes
Acknowledgments
Dr. Rosenberger is supported by National Institutes of Health (NIH) Grant 5-T32-AI-078875-02 from the National Institutes of Health. The remaining authors declare no grant funding. Additional support for this study was provided by a grant from Hunter Surgical Corporation. We thank Gina Wimer, Jeremy Gatesman, and the rest of the University of Virginia Center for Comparative Medicine staff for their help executing this project.
Author Disclosure Statement
Drs. Shada, Rosenberger, Mentrikoski, Silva, and Feldman have no financial disclosures or conflicts of interest. Dr. Kleiner is the inventor of the technology examined in the study and may have the potential for future financial benefit from it.