
Abstract
Abstract
Background:
Post-operative sepsis remains a substantial cause of morbidity and mortality. In injured patients, that a polymorphism of the gene for tumor necrosis factor-β (TNF-β) has been related to the development of sepsis. Genetic factors may also have a role in etio-pathogenesis of sepsis following surgery. We investigated the relationship of the polymorphism of the gene for TNF-β and the serum concentration of TNF-α to the development of sepsis after elective major surgery.
Methods:
The study population consisted of 211 patients undergoing major elective surgery. The NcoI polymorphism of TNF-β was studied in genomic DNA through the analysis of restriction fragments of Nco1-digested DNA with the polymerase chain reaction (PCR). All patients were followed for 1 mo after surgery for any evidence of sepsis. Serum concentrations of TNF-α were measured pre- and post-operatively by enzyme linked immunosorbent assay (ELISA). Genotypes of TNF-β and the production of TNF-α were related to the occurrence of sepsis.
Results:
Post-operative sepsis developed in 21.8% (n=46) of the patients. The overall mortality was 4.2% (n=9). The overall allele frequency of the TNF-β genotype was 0.32 for TNFB1 and 0.68 for TNFB2. Within the TNF-β genotype, 11.84% (n=25) of the patients were homozygous recessive for TNFB1, 41.23% (n=87) were heterozygous, with TNFB1/TNFB2, and 46.91% (n=99) were homozygous dominant for TNFB2. The incidence of post-operative sepsis was significantly (p=0.01) higher in patients homozygous for the TNFB2 allele. When compared with patients carrying at least one TNFB1 allele (TNFB1 homozygous and heterozygous genotype), the TNFB2 homozygous genotype was associated with an odds ratio (OR) of 2.60 (p=0.005; 95% CI 1.32–5.15) for the development of sepsis. As compared with that for the heterozygous genotype, the OR for the homozygous TNFB2 genotype was 3.00 (p=0.003; 95% CI 1.39–6.44). In patients with post-operative sepsis, serum concentrations of TNF-α were significantly higher (p=0.02) in TNFB2 homozygous individuals than in those of individuals of the other TNF-β genotypes.
Conclusion:
The development of sepsis was associated with a greater capacity to produce TNF-α after surgery. The Nco1 polymorphism of the TNF-β gene was associated with the development of post-operative sepsis with an increased serum concentration of TNF-α. In patients without post-operative sepsis, polymorphism of the TNF-β gene was not related to different levels of TNF-α production. This indicates an association between polymorphism of the TNF-β gene and post-operative sepsis, suggesting the TNFB2/B2 genotype as a high-risk factor for the development of sepsis after elective surgery.
T
Cytokine networks are believed to be of major importance in the pathogenesis of infectious diseases, and tumor necrosis factor (TNF) in particular appears to play a crucial role in this [6,7]. The pro-inflammatory cytokine TNF-α is an essential component of the host immune response to infection [8], and is responsible for the release of other inflammatory mediators. Tumor necrosis factor-α also plays a major role in the clinical manifestations of septic shock [9], and its serum concentrations correlate inversely with survival in severe sepsis [10,11]. With regard to this, an inherited variability in cytokine production, including that of TNF-α, and a genetic predisposition to fatal infectious diseases have been suggested [12]. The variability in TNF-α synthesis was initially correlated with genotypes of class II human leukocyte antigens (HLA) [13,14]. However, the location of the gene that encodes TNF-α and TNF-β within the major histocompatibility complex (MHC) raised the possibility that genetic alterations in the loci for these cytokines may be involved directly in a high level of production of TNF-α. A restriction fragment length polymorphism (RFLP) present in the TNF-β gene is correlated with increased concentrations of TNF-α in plasma and a high mortality in patients with severe sepsis [15]. The mortality in severe sepsis was found to be statistically significantly greater in patients homozygous for the TNFB2 allele than in those heterozygous for the Nco1 poly-morphism. A statistically significant association was found for the genotype of biallelic Nco1 polymorphism of the TNF-β gene and the development of severe sepsis after major blunt trauma [15].
For this reason, it must also be considered possible that a genetically determined inflammatory response contributes to sepsis or other post-operative complications in elective surgeries. In view of this, it would be important to find a genetic marker that identifies surgical patients with an increased susceptibility to post-operative sepsis. Because of a strong association of TNF-β Nco1 polymorphism and the risk of severe sepsis after major trauma [15], we hypothesized that this polymorphism might have a role in the development of sepsis following major surgery. We therefore conducted a study to determine the relationship of the NcoI polymorphism of the gene for TNF-β and the occurrence of sepsis after major surgery.
Materials and Methods
Patient characteristics and study protocol
Ethical approval for the study was obtained from the institutional ethics committee, King George's Medical University (KGMU), Lucknow, India. Two hundred eleven patients who underwent major elective abdominal surgery during October 2010 to June 2012 in the surgical wing of the University Hospital (KGMU) were included in the study. Elective major surgery was defined as planned surgery requiring more than one hour of operating time and anesthesia or respiratory assistance. All patients enrolled in the study met the criteria of being 18–50 y of age and without pre-existing infection, rheumatoid arthritis or a seronegative inflammatory arthropathy, malignant disease, or diabetes mellitus; not taking a steroid medication; and having no acquired or inherited immunodeficiencies. Informed consent was obtained for the withdrawal of blood samples for determining patients' individual NcoI polymorphism for TNF-β and serum cytokine analysis, and prospective collection of the patients' data. All of the patients had surgery under conditions as similar as possible, as the first case of the day to undergo surgery in the operating room by the same operating team. The intra-operative blood loss and duration of surgery (incision to closure) for each patient were recorded. The patients; characteristics are shown in Table 1. All patients were given non-steroidal anti-inflammatory drugs for post-operative pain, and at the time of induction of anesthesia were given a single intravenous dose of a broad-spectrum antibiotic (a third-generation cephalosporin) for prophylaxis against surgical infection. All patients were followed for 1 mo after surgery for any evidence of sepsis. Sepsis was defined according to the criteria of Bone et al. [16] by a body temperature >38.5°C or <35.6°C, tachycardia >90 beats/min, tachypnea >20 breaths/min, leukocytosis >12,000/mcL, or leukopenia <4,000/mcL.
Values are given as numbers (%) or mean±SD.
Differences were tested with the χ2 test and the Fisher exact test for frequencies and with the Student t-test for mean ± SD.
A value of p<0.05 was considered statistically significant.
TNF-α=tumor necrosis factor-α.
Genotype analysis of the Nco1 restriction fragment length polymorphism within the locus of the gene for tumor necrosis factor-β
The genotype of the TNF β gene according to Nco1 RFLP was determined through amplification with polymerase chain reaction (PCR) and enzymatic digestion of the products with Nco1 (Fermentas, ThermoFisher Scientific, Waltham, MA). For this, 3 mL of venous blood were drawn into ethylenediamine-tetra-acetic acid (EDTA)-containing Vacutainer tubes (Becton–Dickinson, Franklin Lakes, NJ), and each patient's genomic DNA was extracted from EDTA-anti-coagulated whole blood with a commercially available deoxyribonucleic acid (DNA) isolation kit (QIAmp DNA Blood Mini Kit, Qiagen, Hilden, Germany) according to the manufacturer's instructions. A 782-bp PCR product of the TNF-β gene was amplified through PCR withthe following pair of primers: forward: 5′-CCGTGCTTCGTGCTTTGGACTA-3′ and reverse: 5′- AGAGGGGTGGATGCTTGGGTTC-3′ [17]. The amplification reaction was done with 10–100 ng of genomic DNA, 0.2 micromol of primers, 200 micromol of deoxynucleotide triphosphates (dNTPs), 1.5 mmol of MgCl2, and 1 unit of Taq polymerase in a total volume of 20 mcL. The PCR conditions consisted of initial denaturation at 95°C for 5 min followed by 35 cycles of denaturation at 94°C for 1 min, annealing at 58°C for 1 min, and extension at 72°C for 1.5 minutes. This was followed by final extension at 72°C for 10 min. A total of 10 mcL of the resulting PCR product was digested with NcoI for 10 min at 37°C, and the resulting fragments were analyzed on 1% agarose gel (Fig. 1).
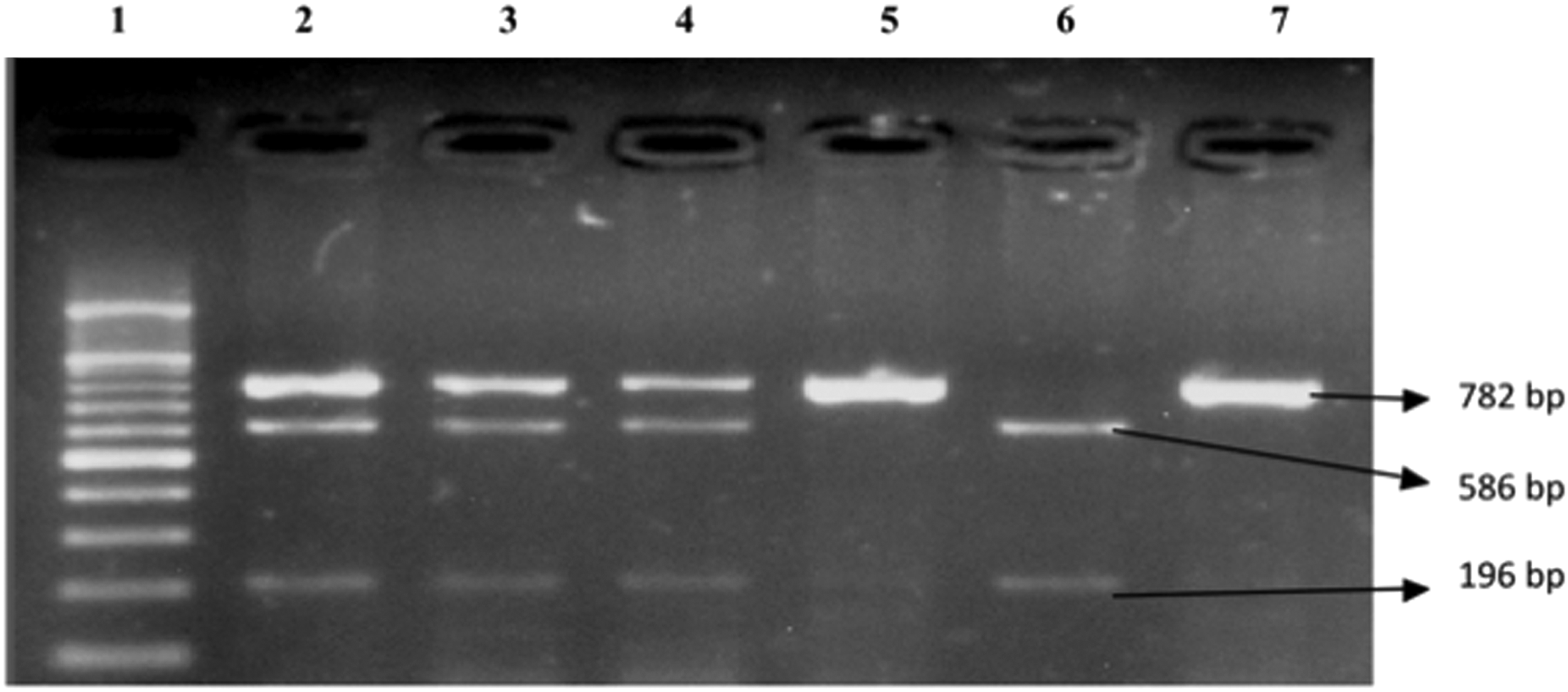
Genotypic analysis of the tumor necrosis factor (TNF)-β gene. The polymerase chain reaction product of 782 bp was digested with the endonuclease Nco1. Lane 1: 100 bp ladder; lanes 2–4: heterozygous genotype (TNFB1/B2); lanes 5 and 7: TNFB2 homozygous genotype (TNFB2/B2); lane 6: TNFB1 homozygous genotype (TNFB1/B1).
Assay of tumor necrosis factor-α
Serum was collected pre- and post-operatively from each of the patients in the study on post-operative days (POD) 2 and 4. Commercially available, highly sensitive enzyme-linked immunosolvent assay (ELISA) kits for human TNF-α (Orgenium AviBion, Vantaa, Finland) were used to measure serum concentrations of TNF-α according to the manufacturer's instructions.
Statistical analysis
Data were expressed as proportion or mean±standard deviation (SD), as appropriate. Testing for intergroup differences in proportions was done with the χ2 test or Fisher exact test. Odds ratios (OR) for the estimation of relative risk were calculated with 95% confidence intervals (CI). For intergroup comparisons, unpaired or paired Student t-test and one-way analysis of variance (ANOVA) was used. A value of p<0.05 was considered as statistically significant.
Results
Of the 211 patients enrolled in the study, 128 (60.66%) were female and 83 (39.33%) were male. The mean age of the patients was 35.97±11.22 y. Post-operative sepsis was diagnosed in 46 (21.80%) of the patients. The patients with and without post-operative sepsis were comparable in terms of parameters including age, gender, duration of surgery, blood loss, and mortality (Table 1). The duration of surgery (p=0.04) and intraoperative blood loss (p<0.001) were observed to be statistically significantly associated with the development of post-operative sepsis. Significantly increased white blood cell counts (WBC) (p<0.001) and mortality (p<0.001) were observed in patients with post-operative sepsis as compared with those without sepsis. The most common post-operative complication found in the study was surgical site infection (n=24; 11.37%), followed by the other complications listed in Table 3. The site of each type of surgery included in the study and the relevant incidences of post-operative sepsis and mortality are shown in Table 4. Sepsis was diagnosed in three patients 2 d after surgery, in five patients at 4 d after surgery, in two patients at 5 d after surgery, and in the remaining 36 patients at 8 d or more after surgery. The relevant microbiologic findings on blood culture for each case of post-operative sepsis are shown in Table 5. In all surgical site infections, the organism observed was Staphylococcus aureus.
Values are given as number (%).
Allele frequency and genotype distribution
With regard to TNF-β genotype, 11.84% (n=25) patients were homozygous recessive for TNFB1, 41.23% (n=87) were heterozygous, with TNFB1/TNFB2, and 46.91% (n=99) were homozygous dominant for TNFB2. The distribution of the TNF-β genotype subgroups among the patients was compared in terms of parameters including age, gender, duration of surgery, blood loss, and mortality (Table 2). Post-operative sepsis was observed in 5/25 (20%), 11/87 (12.64%), and 30/99 (30.30%) patients of the TNFB1 homozygous, TNFB1/B2 heterozygous, and TNFB2 homozygous genotypes, respectively. The overall allele frequency was 0.32 for TNFB1 and 0.68 for TNFB2. The allele frequencies of TNFB1 and TNFB2 were 0.22 and 0.78 in patients with post-operative sepsis and 0.35 and 0.65 in patients without post-operative sepsis.
Values are given as frequency (%) or mean±SD.
Differences were tested with the χ2 test for frequencies and ANOVA for mean±SD. *A value of p<0.05 was considered statistically significant.
TNF=tumor necrosis factor.
The genotype distribution in patients with an uncomplicated clinical course was statistically significantly (p<0.01) different from that in patients with post-operative sepsis. The development of post-operative sepsis was significantly (p=0.01) more frequent in patients homozygous for the TNFB2 allele. However, the likely source of significance is the TNFB2 homozygous versus the TNFB1/B2 heterozygous genotype, which was derived by logistic regression analysis (table not shown). When compared with patients carrying at least one TNFB1 allele (TNFB1 homozygous and heterozygous genotype), the TNFB2 homozygous genotype was associated with an OR of 2.60 (p=0.005; 95% CI 1.32–5.15) for the development of sepsis. Compared with that for the heterozygous genotype, the OR for the homozygous TNFB2 genotype was 3.00 (p=0.003; 95% CI 1.39–6.44). When the TNFB1 and TNFB2 homozygous genotypes were assessed, no significant (p=0.35; 95% CI 0.18–1.86) association of either was found with the development of post-operative sepsis.
Regarding overall mortality, 4.1% (9/211) patients expired during their post-operative hospital stay (eight of the nine patients had post-operative sepsis and one had no evidence of sepsis). In none of the nine patients who expired was a statistically significant difference (p=0.13) observed among the TNF-β genotype subgroups. Similarly, in terms of the deaths of eight of the nine patients with postoperative sepsis, no statistically significant difference (p=0.05; 95% CI 0.02,1.27) was observed between the TNFB2 homozygous and TNFBI/B2 heterozygous subgroups.
Serum concentrations of tumor necrosis factor-α
No significant difference (p=0.90) in serum TNF-α concentration was observed in the pre-operative samples of patients who did and did not develop post-operative sepsis, whereas on both POD 2 and 4, serum concentrations of TNF-α were significantly higher (p<0.001) in patients who developed sepsis following surgery (Table 1).
Tumor necrosis factor-α production in relation to different TNF-β genotypes
To study whether TNF-α production was influenced by the TNF-β genotype, we grouped the patients with and without post-operative sepsis according to their TNF-β genotypes and compared the TNF-α production in the groups. A significant increase (p=0.02) was observed in TNF-α production in the TNFB2 homozygous patients with sepsis as compared with that in patients in the other subgroups of TNF-β genotype, whereas no such increment was observed in patients without sepsis (Figs. 2 and 3).
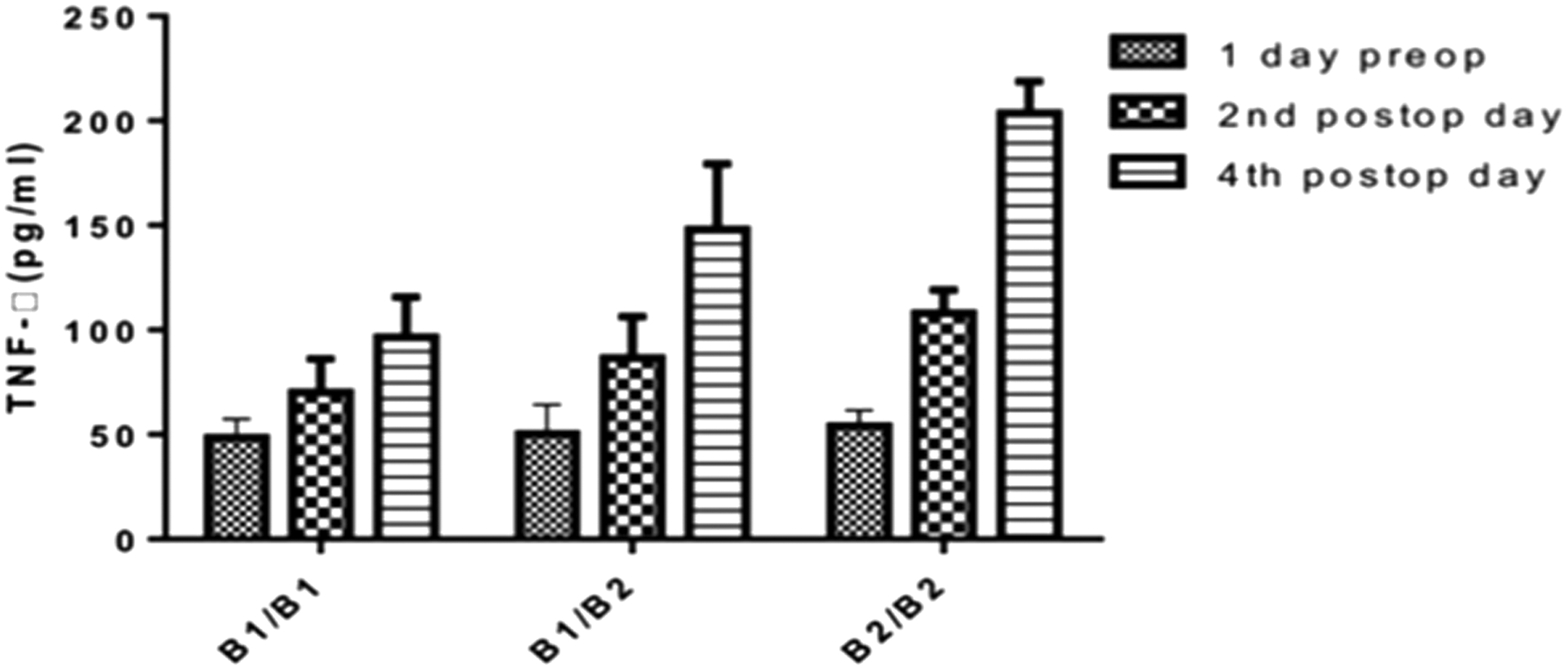
Comparison in the pre- and post-operative concentrations of tumor necrosis factor (TNF)-α in patients with post-operative sepsis and in TNF-β genotype subgroups. Statistical analysis using one-way analysis of variance showed a significant difference (p=0.02) in the serum concentration of TNF-α on post-operative day 4 in different TNF-β genotype subgroups, whereas no such significant difference was observed pre-operatively or on post-operative day 2 (p=0.93 and p=0.31, respectively).
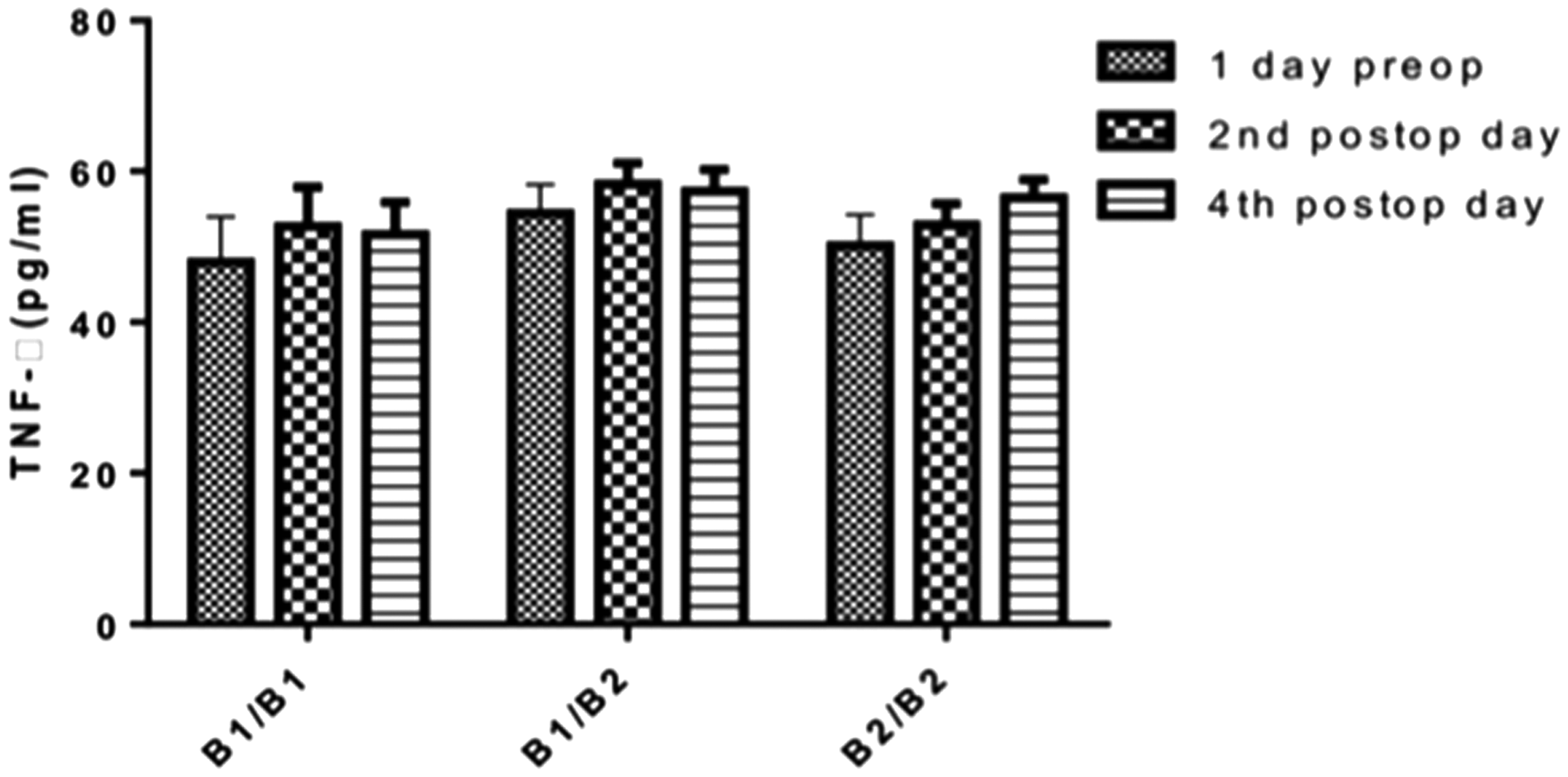
Comparison in the pre- and post-operative concentrations of tumor necrosis factor (TNF)-α in patients without post-operative sepsis and in genotype subgroups. Statistical analysis using one-way analysis of variance showed an insignificant difference in the pre- and post-operative concentrations of TNF-α in the different genotype subgroups (pre-operatively: p=0.63; post-operative day 2: p=0.34; post-operative day: p=0.58.
Discussion
Tumor necrosis factor-α is believed to be a pivotal pro-inflammatory mediator in the host defense against infection [18,19]. However, only a limited number of studies have been done of the relationship of cytokine production to genetic susceptibility to sepsis [12,20]. Several polymorphic elements in the region of the TNF gene have been related to TNF production, but the precise location of the genetic elements controlling the TNF response remains unclear, and their expression has been shown to be regulated only in part by transcriptional events [21–23]. Two single nucleotide polymorphisms (SNP) in the human TNF-α/TNF-β gene that might influence TNF-α secretion have been described as being associated with clinically severe forms of infectious diseases [15,23–25]: the Nco1 polymorphism of the TNF-β gene and a G/A polymorphism at position −308 in the promoter region of the TNF-α gene. Reports of an association between polymorphism of the TNF-β gene and increased susceptibility to severe sepsis [15,26,27] encouraged us to examine the distribution of the TNF-β genotype in patients undergoing elective abdominal operations and to determine their post-operative status in terms of the development of sepsis.
In the view of the contradictory findings in previous studies [17,26,28], we studied the functionality of biallelic TNF-β Nco1 polymorphism in relation to susceptibility to post-operative sepsis. We found the allele frequencies and genotype distributions of TNF-β Nco1 polymorphisms to be similar to those previously described in a German population [26,28,29]. In our study, the TNFB2/B2 genotype was present in 46.91% of the population, in which the observed incidence of septic complications was 30%, and was associated with an OR of 2.60 for the development of post-operative sepsis as compared with the other genotypes of TNF-β. At the same time, the low prevalence (11.84%) of the TNFB1 homozygous genotype makes its estimation less accurate as a factor in reducing the risk of post-operative sepsis. Although the TNFB2/B2 homozygous genotype was commonly observed in the patients in our study who did not survive after surgery, the association of this genotype with mortality after surgery was not statistically significant (p=0.05). Previous studies of the relationship to sepsis of the TNFB2/B2 genotype among the Nco1 polymorphisms of the TNF-β gene demonstrated a poor prognosis and an increased mortality for this genotype as compared with the other genotypes of TNF-β [15,26,28,30]. The possibility that variation in the immune response associated with different TNF-β genotypes may be responsible for the development of sepsis cannot be ruled out. Given that a strict protocol for asepsis was used for all of the patients in our study for the entire duration of the study, we believe that the results of the study do not reflect a breach in anti-infective measures, but instead reflect genetic differences in the immune response to septic insult itself.
Because most of the patients in our study who developed septic complications post-operatively were of the TNFB2/B2 genotype, we doubted that this genotype influenced the post-operative production of TNF-α by leukocytes in the blood. To assess this, we analyzed serum concentrations of TNF-α pre- and post-operatively in our patients who did and did not develop post-operative sepsis in relation to their TNF-β genotypes. In accord with the available literature on patients with severe sepsis [15,26], patients in our study who had a TNFB2/B2 homozygous genotype had a greater serum TNF-α response post-operatively than that of the patients with other TNF-β gentoypes. Although an increased cytokine response may be related to surgical stress, Majetschak et al. [31] reported that the stress associated with surgery is transient and does not contribute significantly to an increased cytokine response for more than 24 h after surgery. In contrast to a previous report [32], we found that the degree of TNF-α production in whole blood in our patients who did not have complications was unrelated to the polymorphism of the TNF-β gene. Although the source of the measured serum concentration of TNF-α in patients with post-operative sepsis is unknown, the difference found in serum TNF-α concentrations in the TNF-β genotypic subgroups in our study may be associated with the distinct capacity of monocytes to produce TNF-α as an inflammatory cytokine that affects susceptibility to sepsis, and this genotype-related difference has been shown to be associated with the Nco1 polymorphism. The preoperative identification of patients at high-risk for developing post-operative sepsis may be useful in clinical practice for preventing post-operative sepsis. Our study suggests that the early identification of patients at high risk of developing severe post-operative sepsis can be achieved with the use of easily collectable markers. These markers represent an inexpensive way in which to identify the high-risk patients in whom the effects of early, aggressive, goal-directed antiseptic treatment can be evaluated in future studies.
It is well known that various factors related to the nature of an operation or to the patient will influence the occurrence of major post-operative complications. The same team operated the patients in the current study and as the first case of the day in the operating room. This aimed to maintain uniformity in the study. We found that the amount of intra-operative blood loss and duration of surgery statistically significantly influenced the development of post-operative sepsis (Table 1), a finding also reported by other investigators [32–35], but we found no association of this with TNF-β genotypes. Other patient-related factors, such as age and gender, had no influence on the development of post-operative sepsis. Although various studies indicate that pre-existing patient-related factors (e.g., advanced age, male gender) may influence the development of post-operative complications [33,34,36–40], the findings in this regard are inconsistent. Ansari et al. [41] reported that age influences the development of post-operative complications, whereas Tang et al. [33] could not identify age as a risk factor for the same type of surgery as in the study by Ansari et al. Some studies found male gender to be an independent risk factor for the development of post-operative complications such as sepsis [38,34], whereas others could not confirm these findings [39,40]. Vogel et al. [42] described the rates of sepsis for a variety of hospital-based surgical procedures. Gastrointestinal, cardiovascular, and thoracic procedures accounted for nearly 50% of cases, and the rates of post-operative sepsis were highest for esophageal, pancreatic, gastric, small bowel, hepatic, and biliary procedures. Hensler et al. [43] reported a greater frequency of post-operative sepsis after esophagectomy. In our study, pancreatic operations, among all major elective gastrointestinal procedures, accounted for most (30.43%) of the instances of post-operative sepsis.
The major finding in the present study was that the biallelic Nco1 polymorphism of the TNF-β gene is associated significantly with the development of sepsis after major surgery. However, it cannot be ruled out that the Nco1 polymorphism is not itself related directly to susceptibility to sepsis, but rather serves as a marker linked to the major histocompatibility complex (MHC) because of its location in the class III region of the MHC [21,23].
A limitation of the present study is that the influence of TNF-β genotypes on the development of post-operative sepsis according to type of surgical procedure could not be established because of the small number of patients undergoing each type of surgery. Similarly, the small number of TNFB1 homozygous patients in the study makes the estimation of this genotype less accurate as a risk-reducing factor for sepsis, demanding a larger cohort for evidence of this, although the possibility of a high risk of the TNFB2 homozygous genotype for sepsis as compared with the risk of TNFB2 heterozygotes should not be dismissed.
Our data provide evidence of a genetic susceptibility to sepsis in surgical patients. In our study, the development of sepsis was associated with a greater capacity to produce TNF-α after surgery. The Nco1 polymorphism of the TNF gene was associated with the development of post-operative sepsis through an increased serum concentration of TNF. Analysis of this polymorphism appears to be a useful means for identifying patients at high risk for sepsis after surgical trauma. Further studies of molecular pathways with larger cohorts are needed to investigate the mechanism of increased susceptibility to sepsis in relation to the TNF Nco1 polymorphism.
Footnotes
Acknowledgments
We thank the Council of Science and Technology of the Government of Uttar Pradesh, Lucknow, India for financial support.
Author Disclosure Statement
The authors declare no conflicts of interest in the work described in this paper.