
Abstract
Abstract
Background:
Blood stream infection (BSI) is a major cause of mortality and morbidity for patients undergoing cardiac surgery. However, information is lacking about patients undergoing off-pump coronary artery bypass (OPCAB). The purpose of this study was to assess the incidence, risk factors, outcome and associated pathogens of BSI after OPCAB.
Methods:
One thousand ten consecutive patients undergoing OPCAB between 2001 and 2012 were included in a retrospective case-control study. A propensity-matched control was used for risk factor analysis.
Results:
Of the 1,010 patients, 26 patients (2.6%) had 32 episodes of BSI after surgery, which occurred at a median of 14 d after surgery. Gram-negative bacilli and gram-positive cocci were distributed equally. Methicillin-resistant Staphylococcus aureus was the pathogen identified most frequently, and the most common source of infection was a surgical site. The hospital mortality rate was 54%. By univariable analysis, diabetes mellitus, pre-operative renal impairment, pre-operative low hemoglobin, pre-operative endotracheal intubation, dialysis before or after surgery, cardiogenic shock, left ventricular ejection fraction of less than 40%, non-elective surgery, low number of distal anastomoses, atrial fibrillation after surgery, and re-operation for bleeding were significant risk factors. By multivariable analysis, the independent risk factors were left ventricular ejection fraction of less than 40%, low number of distal anastomoses, atrial fibrillation after surgery, and dialysis after surgery.
Conclusions:
Blood stream infections remained a common complication after OPCAB, and the mortality was high. Gram-negative bacilli and gram-positive cocci were distributed equally. Methicillin-resistant S. aureus was the pathogen identified most frequently. Preventive tactics should target likely pathogens and high-risk patients undergoing OPCAB.
N
Coronary artery bypass surgery has been performed traditionally with the use of cardiopulmonary bypass. The technique of operating on a beating heart, or “off-pump”, has been developed to decrease post-operative complications, some of which are related to the use of cardiopulmonary bypass [11,12]. Risk factors of post-operative BSI have not been assessed in the setting of off-pump coronary artery bypass (OPCAB). The purpose of this study was to describe the incidence, pathogens, and outcome of BSI after OPCAB and to identify the peri-operative risk factors that were associated with BSI.
Patients and Methods
In this retrospective study, we included all consecutive patients undergoing OPCAB between December 2001 and January 2012 at the National Taiwan University Hospital. Patients who underwent a combined procedure of coronary artery bypass surgery and valvular or aortic surgery were excluded. No patient was excluded from this study because of pattern of coronary artery disease, cardiogenic shock, or emergency surgery. Intention-to-treat data were obtained in the present study. OPCAB cases that were converted to on-pump procedures remained in this study. National Taiwan University Hospital is a 2,200-bed tertiary-care hospital. It serves an urban population of two million as both first-line and tertiary facilities. It also serves as a referral center for other hospitals in the country with a population of 23 million people. All data were collected by retrospective chart review. The local institutional medical ethics committee approved the study and waived the need for informed consent.
Antibiotic prophylaxis
Prophylactic antibiotic consisting of 1 g cefazolin given just before surgery and every 8 h thereafter was prescribed to every patient. Prophylaxis continued for 3 d or until the removal of mediastinal tubes. Hair was shaved in the operating room. Peri-operative mupurocin ointment was not used. Pre-operative disinfection of the skin of the thorax and legs was performed with povidone-iodine and chlorhexidine solution. All procedures were performed by the same surgical and nursing team.
Surgery
Beginning in December 2001, we treated all patients with coronary artery disease with coronary artery bypass grafting without the use of cardiopulmonary bypass, or systematic OPCAB. Surgery was performed through a median sternotomy. The heparin dose is two-thirds of the standard dose for cardiopulmonary bypass. It is administered prior to division of the internal mammary artery. The target activated clotting time is greater than 350 sec. This is partially reversed by administration of one-half the calculated protamine dose after the completion of coronary anastomoses. Cardiopulmonary bypass was on standby without priming the pump. Distal anastomoses were performed using a suction-type coronary stabilizer and intracoronary shunt. Pericardial traction suture and apical suction devices were not used for assistance. The usual order of bypass was anterior wall, posterior wall, and lateral wall. Surgery was converted to on-pump beating-heart coronary artery bypass if there was hemodynamic compromise during the procedure [13].
Definition
We considered BSI as important when one or more microorganisms were isolated in one or several blood cultures. Specimens for culture were obtained when indicated clinically, and no surveillance was performed routinely. In cases involving microorganisms of doubtful (e.g., Bacillus spp., nonhemolytic Streptococcus spp., coagulase-negative Staphylococcus spp.), relevant episodes were defined as those in which there was evidence of clinical infection with no other explanation and in which the microorganisms were isolated from two or more different blood cultures. The source of BSI was considered documented if there were focal signs or symptoms of infection or the same microorganism was isolated from blood and the infected site. In the absence of a recognized source, BSI was classified as primary.
Risk factors
During the study period, 130 patients who were propensity-matched for age and sex and did not have BSI were selected as the control group. Data were compared between the study patients and control patients.
Statistical analysis
Continuous variables were expressed as median with range or mean±standard deviation and were compared by use of Mann-Whitney U test. Categorical variables were expressed as percentages and analyzed by Fisher exact test. To identify risk factors for BSI, univariate analysis of pre-operative, operative, and post-operative characteristics was performed by comparing study and control patients. To evaluate independent risk factors for BSI, variables with a p value of less than 0.1 by univariate analysis were included in the multivariable stepwise logistic regression analysis. The calibration and discrimination of the final logistic model was provided by Hosmer-Lemeshow goodness-of-fit test and area under the receiver operating characteristic curve (AUROC) statistics, respectively. A p value of less than 0.05 was considered statistically significant. All analyses were carried out using SPSS statistical software (SPSS 15.0; SPSS Inc., Chicago, IL).
Results
Incidence
A total of 1,010 consecutive patients underwent systematic OPCAB. There were 809 men and 201 women, with a median age of 67 y (range, 26 to 91y). The mode of surgical intervention was elective in 737 patients, urgent in 176 patients, and emergent in 97 patients. The hospital mortality rate was 0.4 % in elective cases, 8% in urgency cases, and 33% in emergency cases. The major causes of in-hospital death were cardiogenic shock in 28 patients, severe sepsis in 18 patients, ischemic stroke in two patients, and aortic rupture in one patient.
Of the 1,010 patients undergoing systematic OPCAB, 26 patients (2.6%) developed 32 episodes of BSI after surgery. The annual incidence ranged from 0 to 5.6% during the study years (Fig. 1). Patient data are listed in Table 1. There were 19 males and seven females with a median age of 69.5 y (range, 46 to 86). Successful OPCAB was performed in 21 cases (80%). Surgery was converted to on-pump beating-heart coronary artery bypass because of intra-operative hemodynamic compromise in five cases. The mode of surgical intervention was elective in seven patients, urgent in 14 patients, and emergent in five patients. Re-operation for bleeding was required in three patients. The timing of re-operation was within 24 h after surgery in two patients and on the second post-operative day in one patient. Blood stream infection occurred at the median of 14 d (range, 1 to 201d) after surgery, and only three of them (0.3%) occurred within the first 4 d after surgery. The hospital mortality rate was 54% (Table 1). The causes of in-hospital death were severe cardiogenic shock in two patients, severe sepsis in 11 patients, and ischemic stroke in one patient.
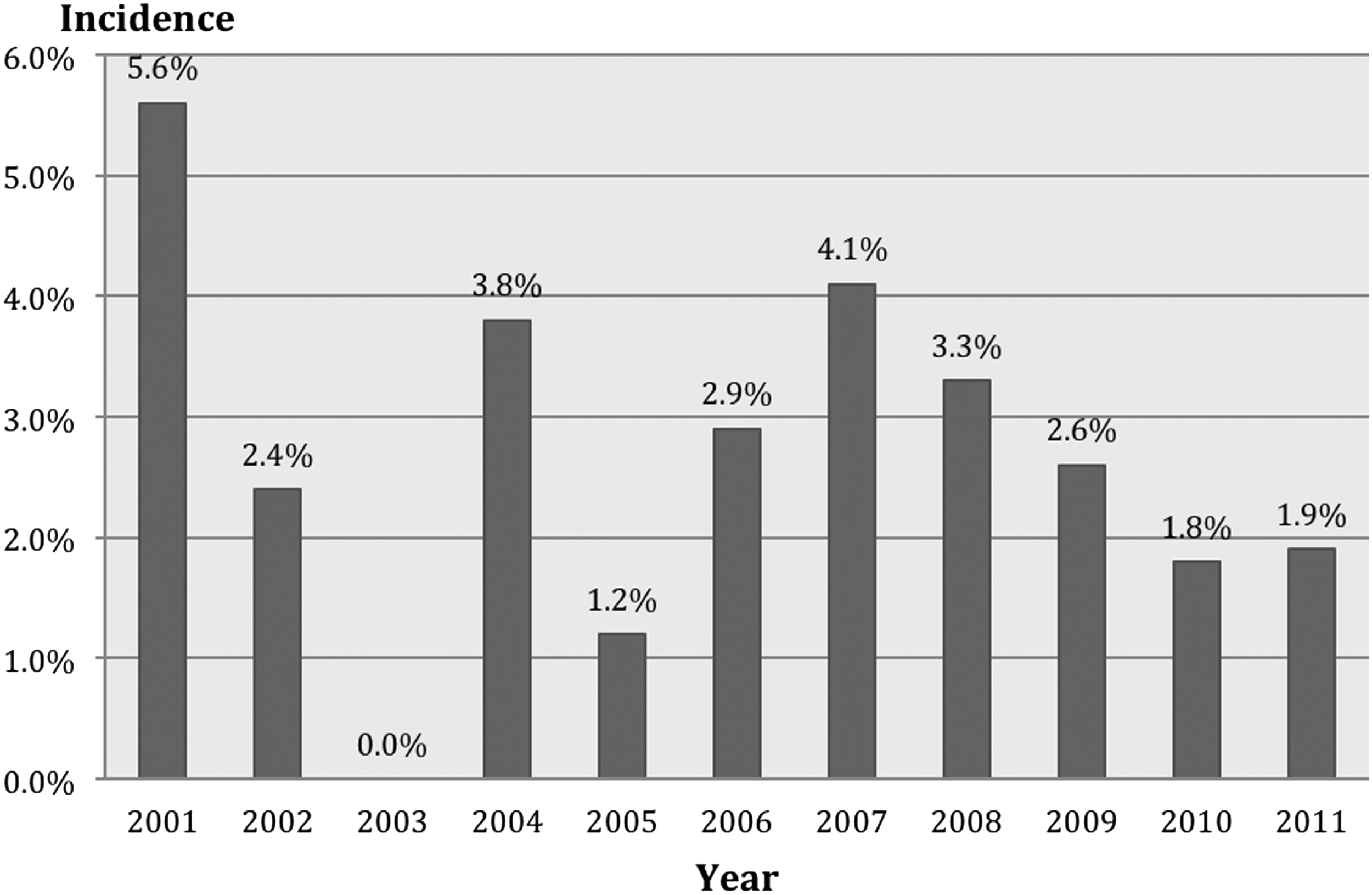
Annual incidence of blood stream infection after off-pump coronary artery bypass.
Categorical variables were presented as number (percentage) and continuous variables were presented as median with range or mean±standard deviation.
Pathogens
There were 33 pathogens isolated from 32 episodes of BSI. One episode was polymocrobial. The number of pathogens and associated mortality are listed in Table 2. Gram-negative bacilli and gram-positive cocci were distributed equally. Methicillin-resistant Staphylococcus aureus was the pathogen identified most frequently followed by S. epidermidis and Pseudomonas aeruginosa. The hospital mortality rate was 60% in gram-positive infection and 50% in gram-negative infection.
The source of BSI in these 32 episodes of BSI is listed in Table 3. The most common source was surgical site infection, occurring in 11 patients (34%), followed by pulmonary infection in seven patients (22%) and catheter-related infection in six patients (19%). The source of infection was not evident in eight patients. Among the eight episodes of BSI caused by methicillin-resistant S. aureus, the source was deep sternal wound infection in seven patients and thoracotomy surgical site infection in one patient undergoing re-operative coronary artery bypass through thoracotomy.
Risk factors
Table 1 showed the clinical data in 26 study patients who had BSI and 130 propensity-matched control patients who did not. By univariate analysis, diabetes mellitus, pre-operative renal impairment, pre-operative low hemoglobin concentration, pre-operative endotracheal intubation, dialysis before or after surgery, cardiogenic shock, left ventricular ejection fraction of less than 40%, non-elective surgery, low number of distal anastomoses, atrial fibrillation after surgery, and re-operation for bleeding were significant risk factors. The hospital mortality rate was significantly increased in patients with BSI (Table 1). Table 4 shows the independent risk factors for BSI by multivariable stepwise logistic regression. The independent predictors of BSI were left ventricular ejection fraction of less than 40%, low number of distal anastomoses, atrial fibrillation after surgery, and dialysis after surgery. The goodness-of-fit χ2 of the model was 8.04 (p=0.235) where the non-significant Lemeshow and Homser test statistic warrants the calibration of the final logistic model. In addition, The AUROC statistic was 0.90%, which indicates excellent discrimination of the model.
Discussion
This was the first study to examine the incidence, pathogens, risk factors, and outcome of BSI after OPCAB. Blood stream infection was diagnosed in 2.6% of patients undergoing OPCAB. Patients who developed BSI had a high hospital mortality rate of 54%. Several peri-operative risk factors were identified. They included diabetes mellitus, pre-operative renal impairment, pre-operative low hemoglobin concentration, pre-operative endotracheal intubation, dialysis before or after surgery, cardiogenic shock, left ventricular ejection fraction of less than 40%, non-elective surgery, low number of distal anastomoses, atrial fibrillation after surgery, and re-operation for bleeding. The independent predictors of BSI were left ventricular ejection fraction of less than 40%, low number of distal anastomoses, atrial fibrillation after surgery, and dialysis after surgery.
The risk of developing post-operative BSI varies substantially with the type of surgery and is generally highest for cardiac surgery [14]. Because the complexity of cardiac surgery affects the rate of post-operative BSI [2–10], we focused this study on a homogeneous group of patients who underwent OPCAB. Blood stream infection was a common post-operative complication after coronary artery bypass surgery. The reported rate of BSI after coronary artery bypass surgery varied from 2.4% to 3.5% [2,5,7,9]. The comparison of incidence between studies was difficult due to different follow-up durations after surgery [2,5,7,9]. In a recent study involving 4,515 patients [5], BSI occurred in 3.3% of patients within 90 d after surgery. (OPCAB was performed in 9.9% of their patients.) The median time of onset was 16 d and the 90 d mortality rate was 35%. We had a comparable result in incidence and time of onset. However, our data showed that OPCAB did not seem to lower the rate of post-operative BSI significantly, probably because the rate of early BSI related to the use of cardiopulmonary bypass was low [3].
Traditionally, gram-positive bacteria were the main cause of post-operative BSI [1,2,4–7]. Olson et al. reported that BSI was caused by gram-positive cocci in 63%, gram-negative bacilli in 32.1%, fungi in 14.1%, and was polymicrobial in 10.3% [5]. However, recent data have reported a shift in the spectrum of organisms causing BSI. Gram-negative bacteria have re-emerged as causative organisms for BSI [8,10]. In this study, gram-negative bacilli and gram-positive cocci were distributed equally.
Surgical site infection, pneumonia, and catheter-related infection were the main sources of BSI after cardiac surgery [4,14]. Deep sternal surgical site infection occurred in 1% to 3% of all patients undergoing median sternotomy. Gram-positive bacteria were the major pathogens responsible for deep sternal surgical site infection after cardiac surgery [7]. Ventilator-associated pneumonia also was one of the major nosocomial infections after cardiac surgery. Ventilator-associated pneumonia among intubated patients was caused predominantly by gram-negative bacteria [2,15]. Central venous catheters are the catheters used most commonly after cardiac surgery. The National Nosocomial Infections Surveillance System reported the microorganisms most commonly associated with vascular catheter-related infection to be coagulase-negative staphylococci [14]. Recently, gram-negative bacteria have become the predominant isolates in catheter-related BSI [4,8,16]. Our study, as did others [4,8,16], has shown an increase of gram-negative infection for post-operative BSI. Gram-positive bacteria were the predominant isolates in patients with BSI secondary to surgical site infection, whereas gram-negative bacteria were the predominant isolates in patients with BSI secondary to pneumonia or vascular catheter-related BSIs.
The increased prevalence of gram-negative infections in this study may be attributed to the current clinical practice of using prophylactic cefazolin that covers primarily gram-positive organisms in the post-operative period. The emergence of enetric gram-negative bacteria may be typical of those acquired from the hospital environment [17,18] or may be of endogenous origin [3]. Infection caused by gram-negative bacteria has been reported to be associated with contaminated intravascular devices and intravenous solutions [17,18].
The reported hospital mortality rate of post-operative BSI varies from 11% to 37% [2,4,5,8,10]. The risk of death was higher among patients with BSI due to gram-negative bacteria [5] and methicillin-resistant S. aureus [19,20]. In this study, the hospital mortality rate of BSI was 54%, which was higher than would be expected from previous studies [2,5,8,10]. This finding was probably due to the high prevalence of BSI caused by multi-drug-resistant gram-negative bacteria and methicillin-resistant S. aureus at our hospital [19,21].
Several peri-operative risk factors have been identified as contributing to BSI after cardiac surgery. They included the age of patients, length of post-operative follow-up duration, obesity, pre-operative morbid conditions, use of cardiopulmonary bypass, a complex cardiac procedure, and certain major post-operative complications [2–10]. Some published reports have described the incidence and mortality of BSI after coronary artery bypass surgery [2,5,7,9]. However, there is scant information about the risk factors [9] and the risk factors were not assessed in OPCAB. In a study by Spelman et al. of 693 patients undergoing coronary artery bypass surgery [9], the rate of post-operative BSI was 2.7% and obesity was the only identified risk factor for BSI. Further recognition of risk factors for post-operative BSI in patients undergoing coronary artery bypass surgery may help to improve their prognosis and may allow more organized surveillance and infection control measures.
In this study, we identified several independent predictors of BSI: left ventricular ejection fraction of less than 40%, low number of distal anastomoses, atrial fibrillation after surgery, and dialysis after surgery. Although re-operation for bleeding was a significant risk factor by univariate analysis, it lost its significance in the multivariable analysis. Three patients with re-operation underwent urgent or emergency surgery because of refractory heart failure. Patients with left ventricular ejection fraction of less than 40%, post-operative atrial fibrillation, and emergency or urgent operations were usually critically ill, and the preparation of surgical sites, and the insertion site for central venous catheters may not be prepared satisfactorily. Because of the patients' illness, the central venous catheters, urinary catheters, and endotracheal tubes were more likely to be left in situ for prolonged periods of time [1]. Patients with dialysis-dependent end-stage renal disease were more likely to be colonized with S. aureus [22] and to need a longer duration of central venous catheters use for dialysis after surgery. All of these conditions were contributing factors to a higher risk of nosocomial infection in the dialysis patients undergoing urgent or emergency coronary artery bypass.
Several limitations of our study should be recognized. First, the study population was small, and hence we could not examine properly the independent risk factors of BSI in the setting of OPCAB. Second, none of our patients had pre-operative screening for nasal colonization, thus the rate of methicillin-resistant S. aureus nasal carriage was unknown. However, this is the first study to address the incidence, pathogen, outcome, and risk factors of BSI after OPCAB. Our data suggest that future preventive measures should focus on prevention of surgical site infection, ventilator-associated pneumonia, and vascular catheter-related infection, especially in patients undergoing non-elective surgery and requiring post-operative dialysis. A care-bundled approach has been particularly successful in preventing nosocomial infections after cardiac surgery [23–25]. Most control measures have focused on pre-operative identification of methicillin-resistant S. aureus carriers, decolonization with intranasal mupirocin ointment, and intravenous vancomycin for surgical prophylaxis.
In conclusion, BSI are a common complication after OPCAB, and the mortality was high. Gram-negative bacilli and gram-positive cocci were distributed equally. Methicillin-resistant S. aureus was the pathogen identified most frequently. Preventive strategies should target likely pathogens and high-risk patients undergoing OPCAB.
Footnotes
Author Disclosure Statement
No competing financial interests exist.