
Abstract
Abstract
Background:
Thoracic complications resulting from gallstone spillage during laparoscopic cholecystectomy are rare and may occur years after the index surgery. We present the case of a chronic lung abscess resulting from trans-diaphragmatic migration of gallstones spilled and “lost” during a laparoscopic cholecystectomy.
Methods:
Case report and literature review.
Case Report:
A 66-year-old female who had undergone a laparoscopic cholecystectomy 5 y previously presented with hemoptysis and was found to have a chronic lung abscess caused by “lost” gallstones. Her symptoms resolved with video-assisted thorascopic surgery, pulmonary decortication, and wedge resection.
Conclusions:
Thoracic complications from “lost” gallstones following laparoscopic cholecystectomy include empyema, hemoptysis, and cholelithoptysis. These rare complications sometimes require surgery but not all presentations of thoracic gallstones mandate operative intervention. Because of these potential complications of “lost” gallstones, reasonable efforts should be made to retrieve gallstones spilled during cholecystectomy. Persistent pulmonary symptoms following laparoscopic cholecystectomy mandate further radiologic examination and a review of the patient's operative report for “lost” gallstones.
T
Case Report
A 66-year-old female with a history of a laparoscopic cholecystectomy in 2007 presented with hemoptysis in March 2012. A chest radiograph showed a right pleural effusion and right lower lobe atelectasis, and a computed tomographic (CT) scan of the chest demonstrated three hypodense foci resembling gallstones, with surrounding peri-diaphragmatic inflammatory changes (Fig. 1). An outpatient bronchoscopy was done and each bronchial segment was visualized, with no evidence found of bleeding or a mass lesion. However, a bronchoalveolar lavage of the right lower lobe demonstrated abundant acute inflammatory cells and scattered macrophages. The final lavage culture grew the common biliary pathogen Klebsiella pneumoniae, which was resistant to ampicillin and ciprofloxacin but sensitive to cefazolin, co-trimoxazole, aztreonam, and meropenem. The patient then began a 3-wk course of oral co-trimoxazole and was seen in the cardiothoracic surgery clinic on the day that her antibiotic treatment was begun.
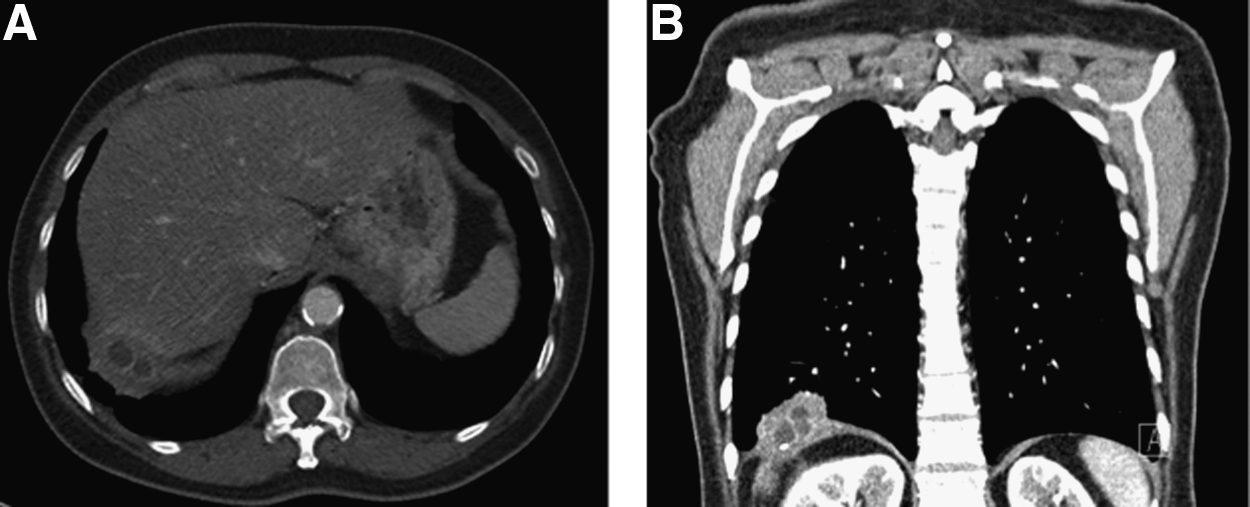
Pre-operative computed tomographic scan showing
One week after being seen in cardiothoracic surgery clinic, the patient was taken to the operating room for definitive management. For prophylaxis against surgical site infection, she was given intravenous cefazolin before her surgical incision was made, but this was not continued post-operatively. Video-assisted thorascopic surgery (VATS) was then performed, including a right pulmonary decortication and wedge resection after the finding of dense pleural adhesions and a right lower lobe abscess associated with three gallstones. The gallstones had migrated through the patient's diaphragm and directly into the posterior basal segments of the lower lobe of her right lung (Fig. 2). The final pathologic examination of the patient's wedge resection demonstrated a pulmonary abscess associated with interstitial fibrosis and chronic inflammation. Gross examination of the gallstones retrieved from her lung demonstrated three irregular brown–tan stones measuring from 1.2 x 1.5 cm in greatest dimension, consistent with cholesterol gallstones. The patient completed a 3-wk course of oral co-trimoxazole post-operatively and her hemoptysis resolved.
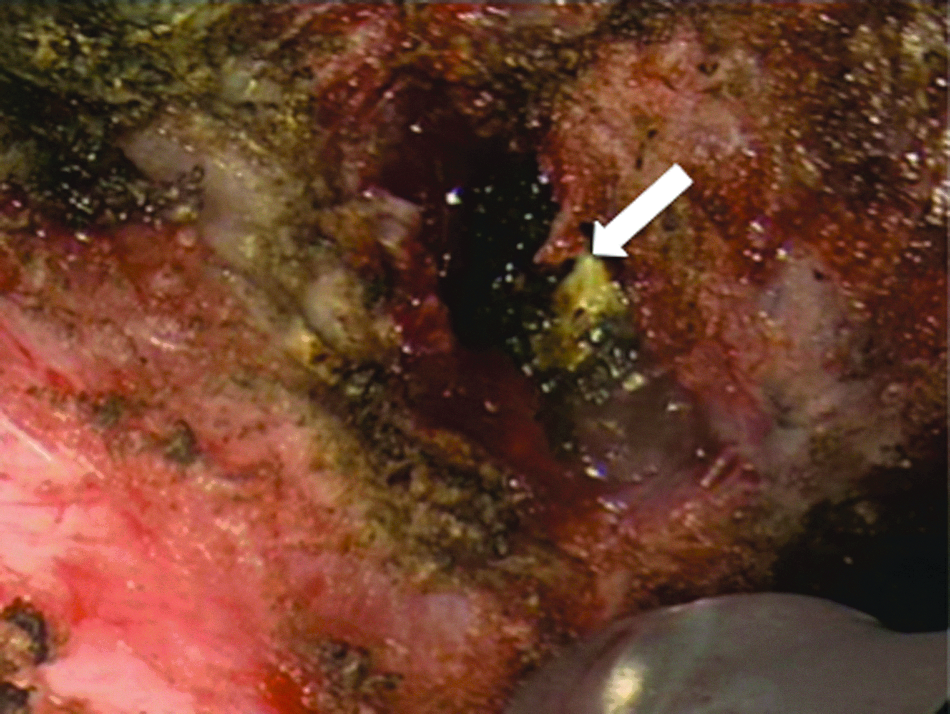
Gallstone (arrow) that has eroded through the diaphragm (screen left), causing a chronic lung abscess and hemoptysis. Color image is available online at www.liebertpub.com/sur
Discussion
Rarely discussed or reported, thoracic complications associated with “lost” gallstones following laparoscopic cholecystectomy include empyema, hemoptysis, and cholelithoptysis. These complications arise from gallbladder perforation during cholecystectomy with spillage of gallstones. If not retrieved, these stones may lead to various abdominal as well as thoracic complications. The incidence of gallbladder perforation in a review of eight large studies done with laparoscopic cholecystectomy was estimated at 12%–36%, with “lost” gallstones occurring in approximately 2% of cases overall [2]. We have been able to find 19 published cases of thoracic complications following laparoscopic cholecystectomy, with the first such study dating to 1993. Thoracic complications may occur from weeks to years after this procedure, as in the present case [5].
The most common complications of spilled gallstones result from abscess, fistula, or both [2]. Once spilled gallstones have migrated into the thoracic cavity, it appears that their final destination determines the clinical presentation and whether surgical management will be required to resolve their effects. Spilled gallstones may give rise to a subphrenic abscess [6] leading to a fistulous tract through the diaphragm and into either the pleural cavity, causing empyema, or into the lung parenchyma, leading to hemoptysis, cholelithoptysis, or a lung abscess. Whether the subphrenic abscess decompresses into the pleural cavity or lung parenchyma is likely to depend on whether there are pleural adhesions between the lung and diaphragm as the result of chronic inflammation and the underlying abscess. As in the case reported here, the perforation of the gallbladder in a previously reported case occurred into the posterior basal segment of the right lower lobe of the lung [4]. Our patient had extensive pleural adhesions, leading to the discovery of a chronic abscess in the lower lobe of her right lung, rather than an empyema, prompting a wedge resection of her right lower lobe.
Because of persistent hemoptysis, our patient was treated with VATS, pulmonary decortication, and a wedge resection. However, surgical intervention is not required in every case of diaphragmatic gallstone transmigration. Five of the 19 previously reported cases of such transmigration were treated non-surgically with antibiotics alone after a thorough work-up including bronchoscopy and CT scanning. In all five of these cases the patient presented with cholelithoptysis, and expectoration of the stones achieved source control, averting the need for surgical management [4–9]. It is apparent that patients presenting with cholelithoptysis whose symptoms appear to have resolved may be safely managed non-surgically. However, a thorough work-up is required to rule out an associated pulmonary abscess, bronchiectasis, and even tuberculosis. Bronchoscopy is optimal for assessing any endobronchial lesions and guiding antimicrobial therapy.
Because of the potential for migration of gallstones, we recommend that surgeons make reasonable efforts, including judicious, targeted irrigation and intra-operative repositioning of the patient, to retrieve any stones spilled during cholecystectomy. We also urge surgeons to document spillage of stones. Our patient's prior surgical report made no mention of this having occurred. Indeed, we believe that patients should be informed when gallstones are spilled and efforts made to retrieve them. Patients need to know that rarely, complications may arise much later when stones are left in the body after being spilled. In a review of six studies involving 18,280 laparoscopic cholecystectomies, Woodfield et al. found that the incidence of gallbladder perforation was 18.3%, that spillage occurred in 7.3% of cases, and that gallstones were lost in 2.4% of cases [1]. Moreover, the risk of future complications increases when all spilled gallstones are not retrieved, as indicated by the finding of Woodfield et al. that gallstone spillage resulted in a complication rate of 2.3%, which increased to 7% when gallstones were lost [1]. Consideration should be given to adding this information to pre-operative informed consent discussions with patients scheduled for cholecystectomy.
Gallstone spillage is not always a benign event. Surgeons should be diligent and persistent in their attempts to retrieve spilled gallstones and be aware that patients with persistent pulmonary symptoms even years after laparoscopic cholecystectomy may be experiencing the consequences of “lost” gallstones.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Disclaimer
The views expressed herein are the authors,’ and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the U.S. Government.