
Abstract
Abstract
Background:
Antimicrobial prophylaxis is required to prevent surgical site infections (SSIs). However, it is difficult to maintain prolonged antimicrobial activity in the surgical incision. Fibrin sealants are used primarily for hemostasis, suture support, or the adhesion of tissues. The aim of this study was to develop fibrin sealants that exhibit antimicrobial activity due to the addition of an antimicrobial agent.
Methods:
We determined the potencies and activities of cefazolin, ampicillin-sulbactam, vancomycin, teicoplanin, and arbekacin eluted from fibrin sealants. The antimicrobial activity was evaluated using methicillin-resistant Staphylococcus aureus (MRSA), multi-drug-resistant Pseudomonas aeruginosa (MDRP), and multi-drug-resistant Acinetobacter baumannii (MDRAB), which are the major pathogens responsible for hospital-acquired infections.
Results:
Each antimicrobial agent eluted continuously from the fibrin clots for approximately two weeks. All eluates from fibrin clots containing antimicrobial agents maintained antimicrobial activity against MRSA for at least 7 d. The eluates from fibrin clots containing ampicillin-sulbactam inhibited the growth of both MDRP and MDRAB for at least 5 d.
Conclusion:
Our data suggest that the addition of an antimicrobial agent to fibrin sealants is a useful method to prevent SSIs caused by bacteria, including antimicrobial-resistant strains.
S
Antimicrobial prophylaxis is a major SSI prevention method [3]. Although antimicrobial prophylaxis maintains therapeutic concentrations of the drug in both the serum and tissues during surgery, the antimicrobial activity is not sustainable after surgery. In addition, antimicrobial-resistant bacteria are resistant to antimicrobial prophylaxis, and the improper use of systemic antimicrobial agents promotes the emergence of resistant bacterial strains. Furthermore, fibrin-enmeshed bacteria may be resistant to phagocytosis or may not interact with antimicrobial agents that diffuse from the incision [1]. Therefore, the most desirable method for the prevention of SSIs may be the direct topical use of antimicrobial agents on the surgical incision and fibrin membrane after surgery.
Fibrin sealants are used primarily for hemostasis, suture support, or the adhesion of tissues [4–6]. Fibrin sealants are sprayed into surgical incisions and dissolve slowly over time due to the action of the fibrinolytic system [7]. These sealants are removed completely by macrophages within two to four weeks. Fibrin sealants can be used after a range of surgical procedures, including cardiovascular, thoracic, and vascular surgery [4]. Recently, some studies have demonstrated that fibrin sealants can be used as drug delivery systems [8].
The addition of an antimicrobial agent to a fibrin sealant is expected to prevent SSIs. Previously, several studies reported the addition of an antimicrobial agent to fibrin sealants [7,9,10]. The published reports include clinical trials and studies on the effect of the sustained release of antimicrobial agents. However, the details of the antimicrobial activities of fibrin sealants containing antimicrobial agents against antimicrobial-resistant bacteria that cause SSIs are unknown. In the present study, we evaluated the characteristics of fibrin clots after the addition of antimicrobial agents. In addition, the amount of antimicrobial agents eluted from the fibrin clots and the duration of this elution were determined. Furthermore, the antimicrobial activity of the eluates from the fibrin clots was evaluated using MRSA, multi-drug-resistant Pseudomonas aeruginosa (MDRP), and multi-drug-resistant Acinetobacter baumannii (MDRAB), which are the major pathogens responsible for hospital-acquired infections.
Materials and Methods
Fibrin sealant and antimicrobial agents
Beriplast® P Combi-Set (CSL Behring, PA, USA) was used as the fibrin sealant. The fibrin sealant was prepared according to the manufacturer's instructions.
The following commercial antimicrobial agents were added to the fibrin sealant: Cefamezin® α (Astellas Pharma Inc., Tokyo, Japan), containing cefazolin; Unasyn®-S (Pfizer Inc., New York, NY), containing ampicillin-sulbactam; vancomycin (Shionogi & Co., Ltd., Osaka, Japan); Targocid® (Astellas), containing teicoplanin; and Habekacin® (Meiji Seika Pharma Co., Ltd., Tokyo, Japan), containing arbekacin. The following antimicrobials were purchased in bulk powder form and used as standards for determining the elution volumes of the antimicrobial agents from the fibrin sealants: Cefazolin (Sigma-Aldrich Co., Tokyo, Japan), ampicillin (Wako Pure Chemical Industries Ltd., Osaka, Japan), vancomycin (Wako), teicoplanin (Sanofi-Aventis S.A., Paris, France), and arbekacin (Meiji Seika Pharma).
Bacterial strains
A solution of Bacillus subtilis ATCC6633 spores (Eiken Chemical Co., Ltd., Tokyo, Japan) was used as the standard for the determination of the elution volumes of cefazolin, vancomycin, teicoplanin, and arbekacin from fibrin clots [11]. Kocuria rhizophila ATCC9341 was used as the standard strain for the determination of the elution volume of ampicillin-sulbactam from fibrin clots [12]. Staphylococcus aureus ATCC29213 and P. aeruginosa ATCC27853 were used as quality control strains for antimicrobial susceptibility testing. The clinical isolates MRSA 2008-57, MDRP 1479, and MDRAB 2106 were used as antimicrobial-resistant bacteria.
Preparation of fibrin sealants containing antimicrobial agent
Each antimicrobial agent was added to Beriplast P Combi-Set B, which contains thrombin and CaCl2. For cefazolin (500 mg of cefazolin), ampicillin-sulbactam (500 mg of ampicillin), and arbekacin (25 mg of arbekacin), one vial was added to Combi-Set B. A part of vancomycin (10 mg of 500 mg) and teicoplanin (10 mg of 200 mg) were also added to Combi-Set B. Combi-Set A, which contains fibrinogen and aprotinin, was prepared according to the manufacturer's instructions. Combi-Set A and Combi-Set B with antimicrobial agents were evenly sprayed onto five φ35 mm tissue culture dishes (Asahi Glass Co., Ltd., Tokyo, Japan). After the fibrin sealants coagulated and dried, the weights of the sealants were determined.
Determination of the elution volume of the antimicrobial agents from fibrin sealants
Sterile saline (1.5 mL) was added to five dishes coated with fibrin sealants containing an antimicrobial agent. After incubation at 35°C for 24 h, samples of eluates from the fibrin clots were collected daily. The antimicrobial elution volume was measured using the bioassay method [11]. The results are shown as the mean values of the elution volumes of five dishes. Fibrin sealant is eliminated gradually from the human body [13]. The elimination of fibrin sealants was modeled with the following equation [14]:
In the present study, the antimicrobial elution volumes were calculated based on the elimination rate of the fibrin sealants.
Antimicrobial susceptibility testing
The minimum inhibitory concentrations (MICs) of the antimicrobial agents were determined using the broth microdilution method according to the Clinical and Laboratory Standards Institute (CLSI) guidelines [15]. In addition, the antimicrobial activities of the eluates from fibrin clots were determined using the following method: The eluates from fibrin clots were added to equal volumes of 2×Mueller-Hinton broth (Oxoid Ltd., Hampshire, UK). Bacterial inoculation and incubation were performed according to the same method described for MIC determination.
Results
Characteristics of fibrin clots containing antimicrobial agents
Cefazolin and ampicillin-sulbactam
One vial was completely dissolved in Combi-Set B of Beriplast P. These fibrin clots were colorless and transparent (Fig. 1).
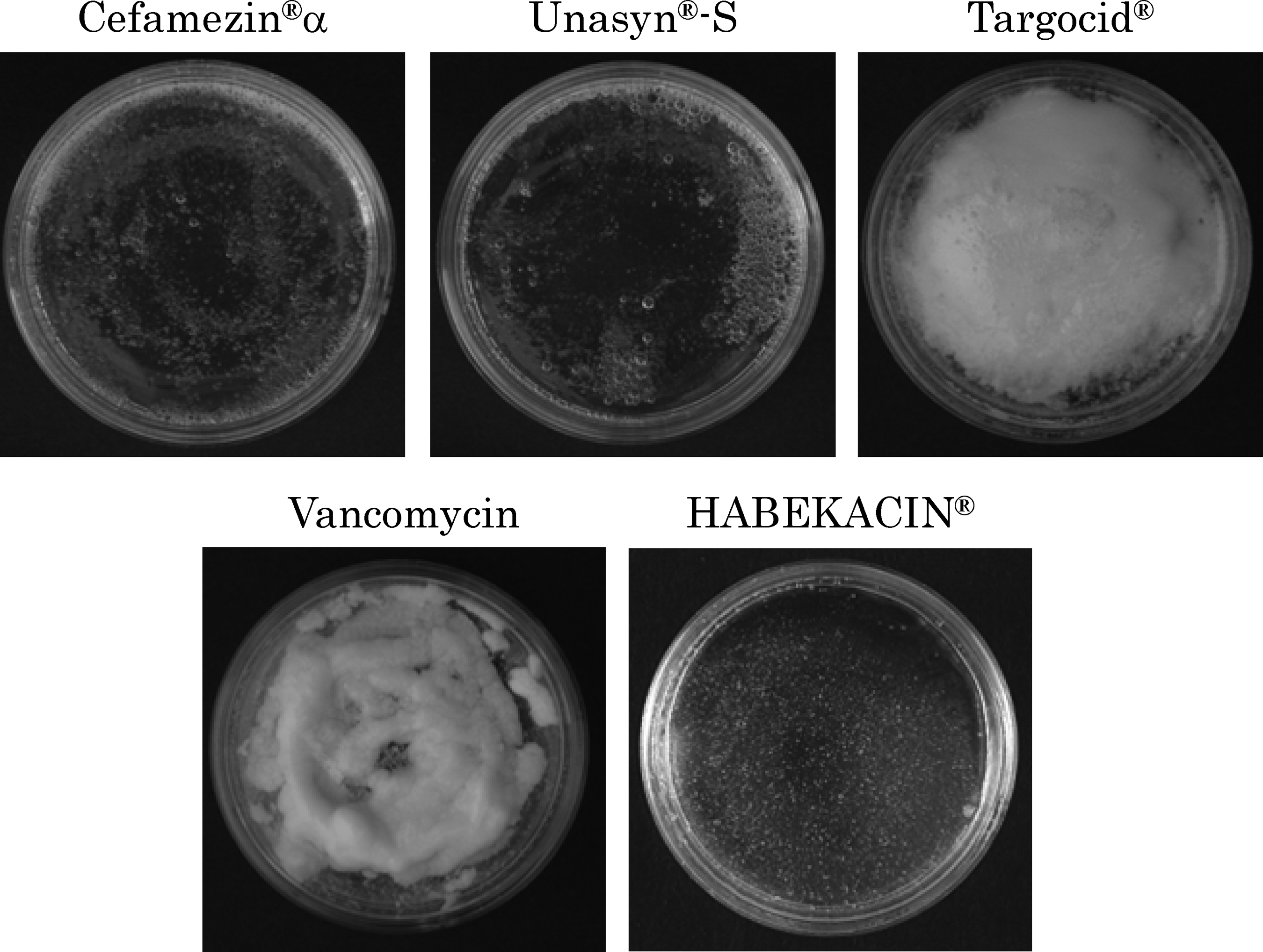
Characteristics of fibrin clots containing antimicrobial agents. See text for generic names.
Arbekacin
The fibrin clot was slightly cloudy but the agent dissolved completely (Fig. 1).
Vancomycin and teicoplanin
When one vial was dissolved in Combi-Set B of Beriplast P, the clots were cloudy and fragile, and precipitation occurred (Fig. 1). When the volumes of the glycopeptides added to Combi-Set B of Beriplast P were decreased, the transparency and strength of the clots were increased (Fig. 2). Although fibrin clots containing<15 mg/mL of the glycopeptides were cloudy, the strength was similar to clots containing other antimicrobial agents. Therefore, 10 mg each of vancomycin and teicoplanin was added to Beriplast P in the subsequent experiments.
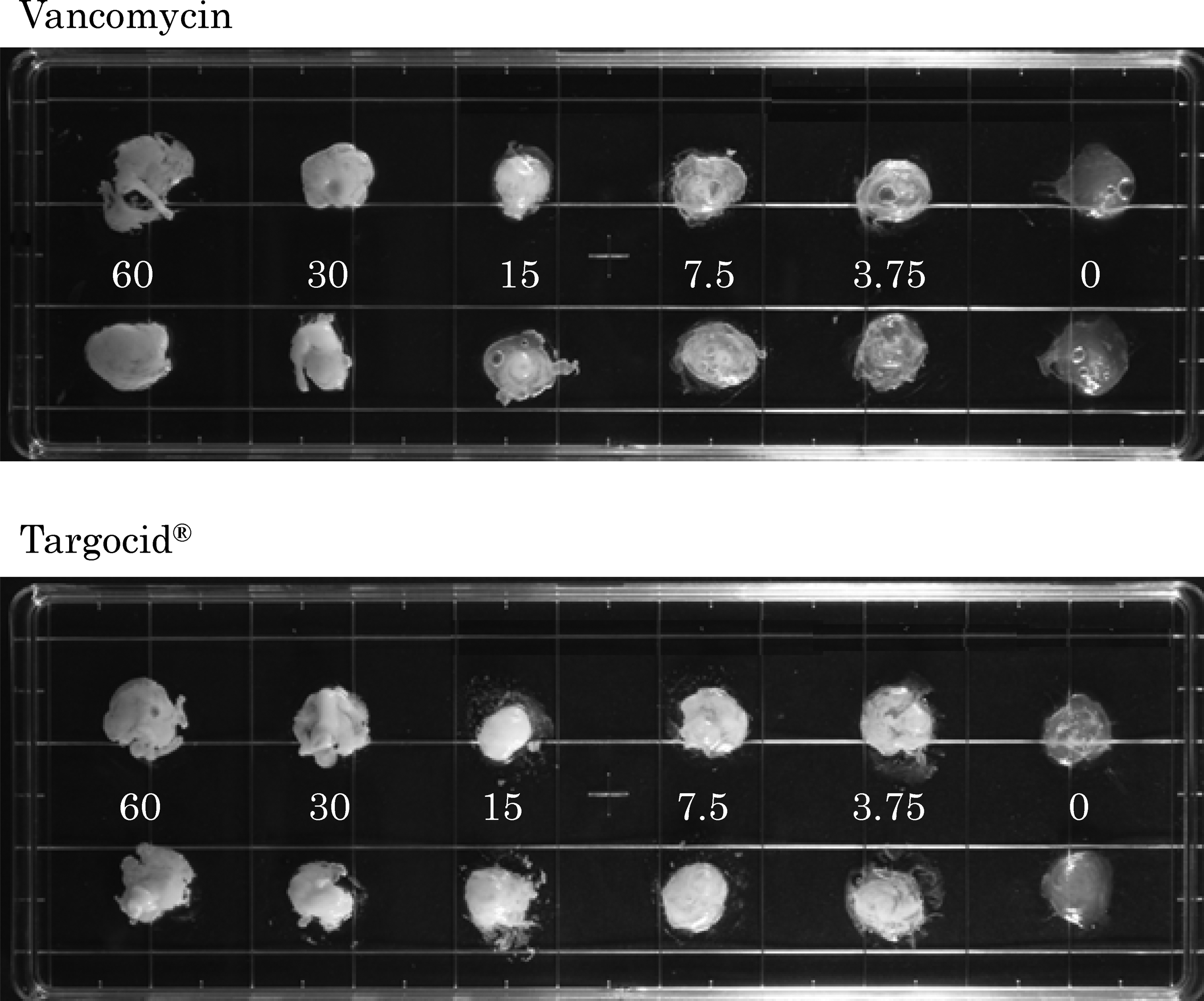
Changes in the coagulation of fibrin clots caused by glylopeptides. The numbers show the concentration (mg/mL) of glycopeptides. The upper and lower clots are the same samples. Targocid®, teicoplanin.
Elution durations and elution volumes of antimicrobial agents from the fibrin clots
Cefazolin
On the first day, 159.6 mg (31.9%) of cefazolin was eluted from the fibrin clot, and the cumulative weight was 258.8 mg (51.68%) over 13 d (Fig. 3).
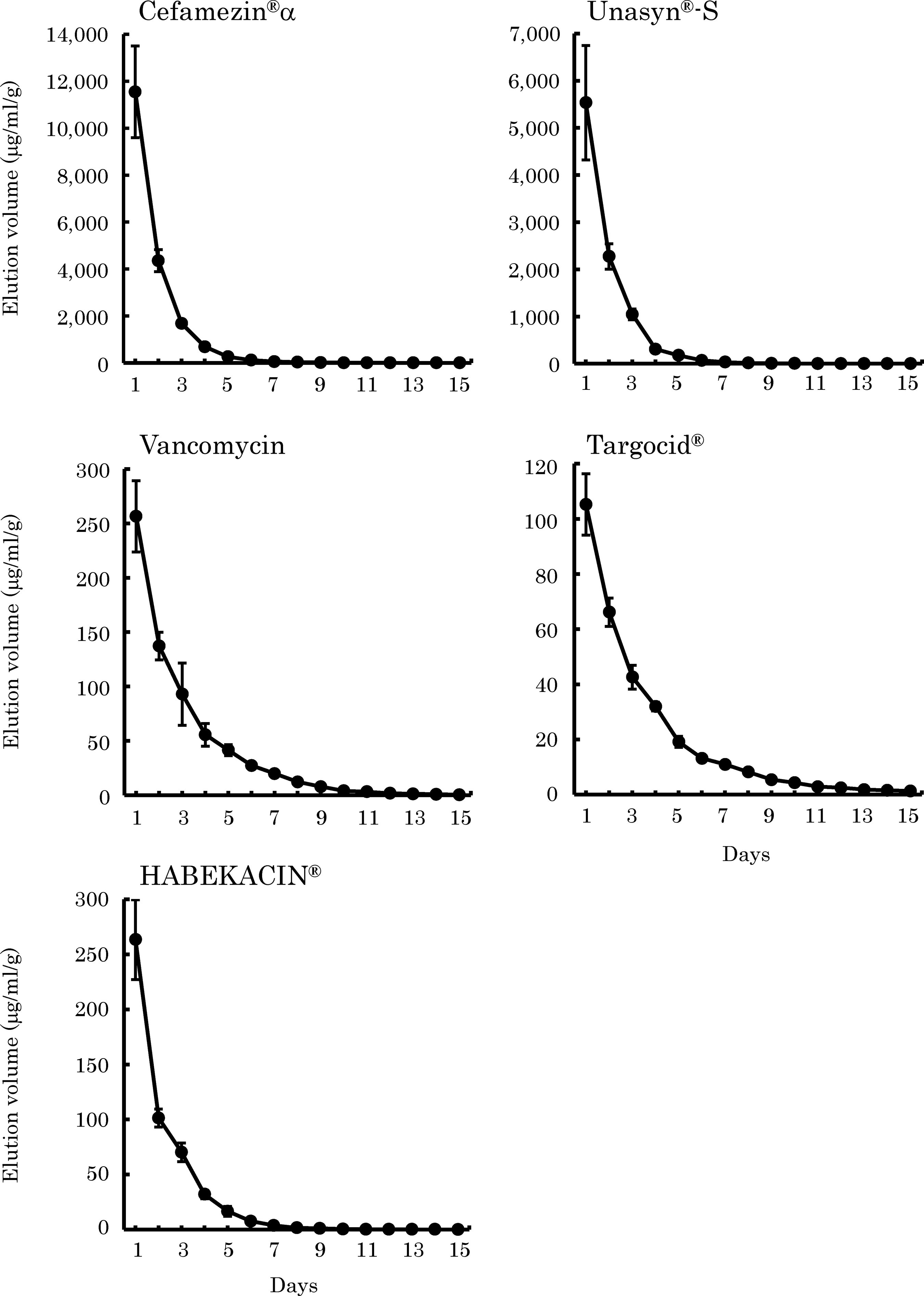
Elution of antimicrobial agents from the fibrin clots. The graphs show the concentration (mcg/mL) of antimicrobial agent per 1 g of fibrin clot. The results are shown as the mean±standard deviation. See text for generic names.
Ampicillin-sulbactam
On the first day, 77.9 mg (15.6%) of ampicillin was eluted from the fibrin clot, and the cumulative weight was 133.1 mg (51.8%) over 15 d (Fig. 3).
Vancomycin
On the first day, 3.4 mg (34.0%) was eluted from the fibrin clot, and the cumulative weight was 8.7 mg (87.0%) over 15 d (Fig. 3).
Teicoplanin
On the first day, 1.5 mg (15.0%) of teicoplanin was eluted from the fibrin clot, and the cumulative weight was 4.4 mg (44.0%) over 15 d (Fig. 3).
Arbekacin
On the first day, 3.6 mg (14.4%) of arbekacin was eluted from the fibrin clot, and the cumulative weight was 6.9 mg (27.6%) over 14 d (Fig. 3).
Thus, these data indicate that all antimicrobial agents used in this study elute from the fibrin clots over approximately two weeks.
Antimicrobial activity of the eluates from fibrin sealants containing antimicrobial agents
The MICs of the antimicrobial agents used in this study for the major bacteria causing hospital-acquired infections were determined using the bulk powder form of those (Table 1). Staphylococcus aureus was susceptible to all tested antimicrobial agents. The MIC values of the β-lactams cefazolin and ampicillin for MRSA were markedly higher than those for methicillin-susceptible S. aureus (MSSA) strain ATCC29213. No antimicrobial activity against P. aeruginosa, multi-drug-resistant P. aeruginosa, and MDRAB was found for the β-lactams and glycopeptides. Multi-drug resistant P. aeruginosa and MDRAB showed low susceptibility to the aminoglycoside arbekacin.
MIC=minimum inhibitory concentration (mcg/mL); IC=inhibitory concentration (mcg/mL) of the antimicrobial agents recovered from a fibrin clot exhibiting antimicrobial activity; S. aureus=Staphylococcus aureus; MRSA=methicillin-resistant Staphylococcus aureus; P. aeruginosa=Pseudomonas aeruginosa; –=antimicrobial activity was not detected; MDRP= multidrug-resistant Pseudomonas aeruginosa; MDRAB=multidrug-resistant Acinetobacter baumannii.
The antimicrobial activities of the eluates recovered from the fibrin clots were determined at daily intervals (Table 1 and Fig. 4). The eluates from the fibrin clot containing cefazolin maintained antimicrobial activity against MSSA, MRSA, and MDRAB for >13 d, 7 d, and 3 d, respectively. However, no antimicrobial activity against P. aeruginosa and MDRP was found for cefazolin. The eluate from the fibrin clot containing ampicillin-sulbactam maintained antimicrobial activity against MSSA, MRSA, P. aeruginosa, MDRP, and MDRAB for >15 d, 10 d, 7 d, 5 d, and 10 d, respectively. Although the eluates from the fibrin clots containing the glycopeptides vancomycin and teicoplanin maintained antimicrobial activity against MSSA and MRSA for >15 d, no antimicrobial activity against P. aeruginosa, MDRP, and MDRAB was found. The eluate from the fibrin clot containing arbekacin maintained antimicrobial activity against MSSA, MRSA, P. aeruginosa, and MDRP for 12 d, 12 d, 12 d, and 9 d, respectively. However, MDRAB grew on all eluates from the fibrin clot containing arbekacin. The volumes of antimicrobial agents eluted from fibrin clots corresponded well with the MICs of the bulk antimicrobial powders.

Antimicrobial activity of the eluates from fibrin clots containing antimicrobial agents. The arrows indicate bacterial growth.
Discussion
Our data showed that one vial of cefazolin, ampicillin-sulbactam, and arbekacin can be added directly to Beriplast P. In contrast, the glycopeptides vancomycin and teicoplanin had to be adjusted to <15 mg/mL for addition to the fibrin clots. Therefore, cefazolin, ampicillin-sulbactam, and arbekacin are easy to add to Beriplast P at the time of surgery.
All antimicrobial agents were eluted continuously from fibrin clots over approximately two weeks. The order of the elution rates of the antimicrobial agents from the fibrin clots was vancomycin>ampicillin-sulbactam>cefazolin α>teicoplanin>arbekacin. Whereas the elution rate of arbekacin (27.6%) was the lowest among the antimicrobial agents used in this study, a previous report showed that 90% of amikacin, which is the same as the aminoglycoside arbekacin, could be eluted from the fibrin sealant at 24 h [16]. Additionally, despite both drugs being glycopeptides, vancomycin and teicoplanin had markedly different elution rates. The plasma protein-binding ratios of amikacin and arbekacin are 0 and 15%, respectively [17,18]. Dykhuizen et al. reported that the plasma protein-binding ratio of vancomycin (36.9%) was significantly lower than that of teicoplanin (97.4%) [19]. Therefore, the differences in the elution rates from the fibrin clots between vancomycin and teicoplanin were considered to be caused by the differences in the plasma protein-binding ratio. Our data suggested that the addition of an antimicrobial agent with a high plasma protein-binding rate to Beriplast P enables the slow release of the antimicrobial agent and long-term antimicrobial activity in the surgical wound.
The bacterial growth inhibitory concentrations of the antimicrobial agents eluted from fibrin clots corresponded well to the MICs of the bulk antimicrobial powders. Thus, no degradation of antimicrobial potency was observed as the result of addition to Beriplast P. In cardiovascular surgery, the most important pathogenic bacteria responsible for SSIs are gram-positive bacteria, such as S. aureus, especially MRSA [20]. A previous study by Kuehn et al. reported the antimicrobial activity of the fibrin sealant containing daptomycin to S. epidermidis [21]. The authors showed that the antimicrobial activity of the fibrin sealant was maintained for 7 d. Our data revealed that all eluates from fibrin clots containing antimicrobial agents maintained antimicrobial activity against MSSA for >10 d. We also revealed that the eluates from fibrin clots containing vancomycin and teicoplanin maintained antimicrobial activity against MRSA for >15 d. Although the MICs of cefazolin and ampicillin for MRSA were high, the eluates from fibrin clots containing cefazolin and ampicillin-sulbactam maintained antimicrobial activity for at least 7 d because a large amount of antimicrobial agent was present in the clots. Therefore, all tested Beriplast P clots containing antimicrobial agents can be used to prevent SSIs due to S. aureus, including MRSA. However, among the five Beriplast P clots containing antimicrobial agents, only the ampicillin-sulbactam-containing clot was able to inhibit the growth of both gram-positive and gram-negative bacteria, including MDRP and MDRAB, for at least 4 d. Therefore, our data suggest that the addition of ampicillin-sulbactam to Beriplast P at the time of surgery may be a suitable approach to prevent SSIs.
In conclusion, our data suggest that the addition of an antimicrobial agent to fibrin sealants is a useful method to prevent SSIs caused by bacteria, including antimicrobial-resistant strains. Further study is necessary to demonstrate the in vivo activity of fibrin sealants containing antimicrobial agents.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.