
Abstract
Background:
Aspergillus infections are associated commonly with immunocompromised states, such as transplantation and hematologic malignant disease. Although Aspergillus infections among patients having surgery occur primarily in transplant recipients, they are found in non-recipients of transplants, and have a mortality rate similar to that seen among transplant recipients.
Methods:
We conducted a retrospective analysis of a prospective data base collected from 1996 to 2010, in which we identified patients with Aspergillus infections. We compared demographic data, co-morbidities, and outcomes in non-transplant patients with those in abdominal transplant recipients. Continuous data were evaluated with the Student t-test, and categorical data were evaluated through χ2 analysis.
Results:
Twenty-three patients (11 transplant patients and 12 non-transplant patients) were identified as having had Aspergillus infections. The two groups were similar with regard to their demographics and co-morbidities, with the exceptions of their scores on the Acute Physiology and Chronic Health Evaluation II (APACHE II), of 23.6±8.1 points for transplant patients vs. 16.8±6.1 points for non-transplant patients (p=0.03); Simplified Acute Physiology Score (SAPS) of 16.6±8.3 points vs. 9.2±4.1 points, respectively (p=0.02); steroid use 91.0% vs. 25.0%, respectively (p=0.003); and percentage of infections acquired in the intensive care unit (ICU) 27.3% vs. 83.3%, respectively (p=0.01). The most common site of infection in both patient groups was the lung. The two groups showed no significant difference in the number of days from admission to treatment, hospital length of stay following treatment, or mortality.
Conclusions:
Although Aspergillus infections among surgical patients have been associated historically with solid-organ transplantation, our data suggest that other patients may also be susceptible to such infections, especially those in an ICU who are deemed to be critically ill. This supports the idea that critically ill surgical patients exist in an immunocompromised state. Surgical intensivists should be familiar with the diagnosis and treatment of Aspergillus infections even in the absence of an active transplant program.
A
Aspergillosis, as defined by the U.S. Centers for Disease Control and Prevention, is an infection caused by the Aspergillus fungus [1]. Aspergillosis is the second-most common opportunistic fungal infection in immunocompromised patients and the third-most common systemic fungal infection requiring hospitalization [4]. The pathway to infection most commonly begins with inhalation of Aspergillus conidia. Infection proceeds typically along one of the three pathways of allergic bronchopulomary aspergillosis, invasive aspergillosis, or aspergilloma [4]. In the immunocompetent patient, spores of Aspergillus are cleared through mucociliary function. Spores that migrate into the distal airways are surrounded by pulmonary macrophages and neutrophils, which stimulate a granulocytic response resulting in granuloma formation (chronic pulmonary aspergillosis–aspergilloma) before further tissue invasion by the organism is made possible [2,5].
However, in immunocompromised individuals, this method of defense is hindered and may lead to invasive aspergillosis. In this scenario, the conidia of Aspergillus fungi germinate, extending hyphae and invading surrounding tissue. Unrestricted growth results in local injury (occlusion of adjacent blood vessels and ischemic necrosis of distal tissue as a result of poor perfusion), but also in systemic dissemination of the organism [2].
Historically, aspergillosis has been a disease associated most commonly with hematologic malignant disease (acute leukemia), stem-cell transplant receipt (hematopoietic stem cell transplantation), solid-organ transplantation, and other causes of immunosuppression (e.g., acquired immunodeficiency syndrome [AIDS], burns, and chemotherapy) [2,6]. However, as increasing numbers of critically ill hospitalized patients without malignant disease survive for longer periods through advances in critical-care medicine, the incidence of invasive aspergillosis and its associated morbidity and mortality are increasing [6–10].
As a result of the recent increasing trend in the diagnosis of invasive aspergillosis in immunocompetent patients, we evaluated our surgical-patient population at the University of Virginia and compared the demographics, co-morbidities, risk factors, and outcomes of both transplant and non-transplant patients infected with Aspergillus over a 14-y period. We hypothesized that Aspergillus infections in non-transplant patients are common and are associated with critical illness, and that mortality in this patient population is similar to that observed among transplant patients.
Patients and Methods
Because of the methodology of data collection and the removal of patient identifiers (anonymity) before the final data analysis in the study, a waiver of consent was granted by the University of Virginia Institutional Review Board for the patient data base that was used in the study.
A retrospective analysis was done on a prospectively collected and maintained data base of all surgical patients seen at the University of Virginia Health System who were treated as inpatients in the general surgery, trauma, and abdominal-organ transplant units at the University of Virginia Hospital. We queried the data base from 1996 to 2010 for surgical patients with confirmed infections caused by Aspergillus species. Demographic information, co-morbidities, risk factors, and outcomes for all of these patients were collected and compared in non-transplant patients and abdominal-organ transplant recipients. Pulmonary and cardiac transplant patients were excluded because a separate department manages their care at our institution.
The patient demographics, co-morbidities, and risk factors evaluated in the study included age, body mass index (BMI), Acute Physiology and Chronic Health Evaluation (APACHE) II Score, Acute Physiology Score, steroid use, white blood cell count (WBC), temperature maximum, days from admission to antibiotic treatment, gender, and race, and whether or not the patient's infection was community acquired, health-care associated, hospital-acquired, or acquired in the ICU. Outcomes evaluated included number of days of hospitalization after antifungal treatment had been initiated, total number of days treated with antifungal agents, and all-cause in-hospital mortality.
At our institution, the gold standard for diagnosis of invasive aspergillosis is a tissue biopsy done directly at the source of infection. However, in most of our patients with pulmonary aspergillosis this is not possible because of pulmonary instability, and other means of diagnosis were therefore utilized. Some of these included consideration of the patient's clinical picture (signs, symptoms, co-morbidities, risk factors) in conjunction with multiple positive bronchoalveolar lavage (BAL) cultures, detection of galactomannan (GM) antigen, and radiographic imaging, typically consisting of computed tomography (CT) of the chest showing a cavitation or halo sign characteristic of pulmonary aspergillosis (Fig. 1). The diagnosis of hematologic, cerebrospinal fluid, and invasive catheter infections was based on clinical signs and symptoms and cultures positive for Aspergillus.

Pathopneumonic radiographic halo sign or crescentic cavitation in aspergillosis.
Until 2002, the gold standard of antifungal treatment for invasive aspergillosis at our institution was amphotericin B, after which voriconazole became the first-line treatment for this disease [11]. We currently use voriconazole as a monotherapeutic agent unless rescue therapy is needed, in which case we add an echinocandin.
Statistical analysis
Categorical data were analyzed through χ2 analysis or Fisher exact tests. Continuous variables were analyzed with independent t-tests or the Mann–Whitney U test, depending on the normality of their distribution. Statistical significance was defined as a value of p<0.05.
Results
A total of 23 surgical patients were identified as having Aspergillus infections at our institution between 1996 and 2010. Demographically, 87% (n=20) of the patients were white and 13% (n=3) were black, 57% (n=13) were receiving chronic steroid therapy, 17% (n=4) had diabetes mellitus, 8.7% (n=2) had renal insufficiency, 17% (n=4) were on dialysis, 43% (n=10) were ventilator-dependent at the time of diagnosis of Aspergillus infection, and 4.3% (n=1) had malignant disease. The different species of Aspergillus isolated from the patients included A. fumigatus in 56.5% (n=13), A. versicolor in 8.7% (n=2), and A. niger in 4.3% (n=1). The sites of infection were the lung in 56.5% (n=13) of the patients, surgical site in 13% (n=3), intra-abdominal in 8.7% (n=2), central/peripheral intravenous catheter in 4.3% (n=1), bloodstream in 4.3% (n=1), skin/soft tissue in 4.3% (n=1), upper gastrointestinal tract in 4.3% (n=1), and cerebrospinal fluid in 4.3% (n=1) (Fig. 2). Some of the patients had co-infections with other organisms, which included Candida albicans, methicillin-sensitive Staphylococus aureus, methicillin-resistant S. aureus, Enterococcus faecium (VRE), Corynebacterium spp., Nocardia nova, Escherichia coli, Enterobacter aerogenes, E. taylori, Pseudomonas aeruginosa, Serratia marcescens, and Morgan morganii.
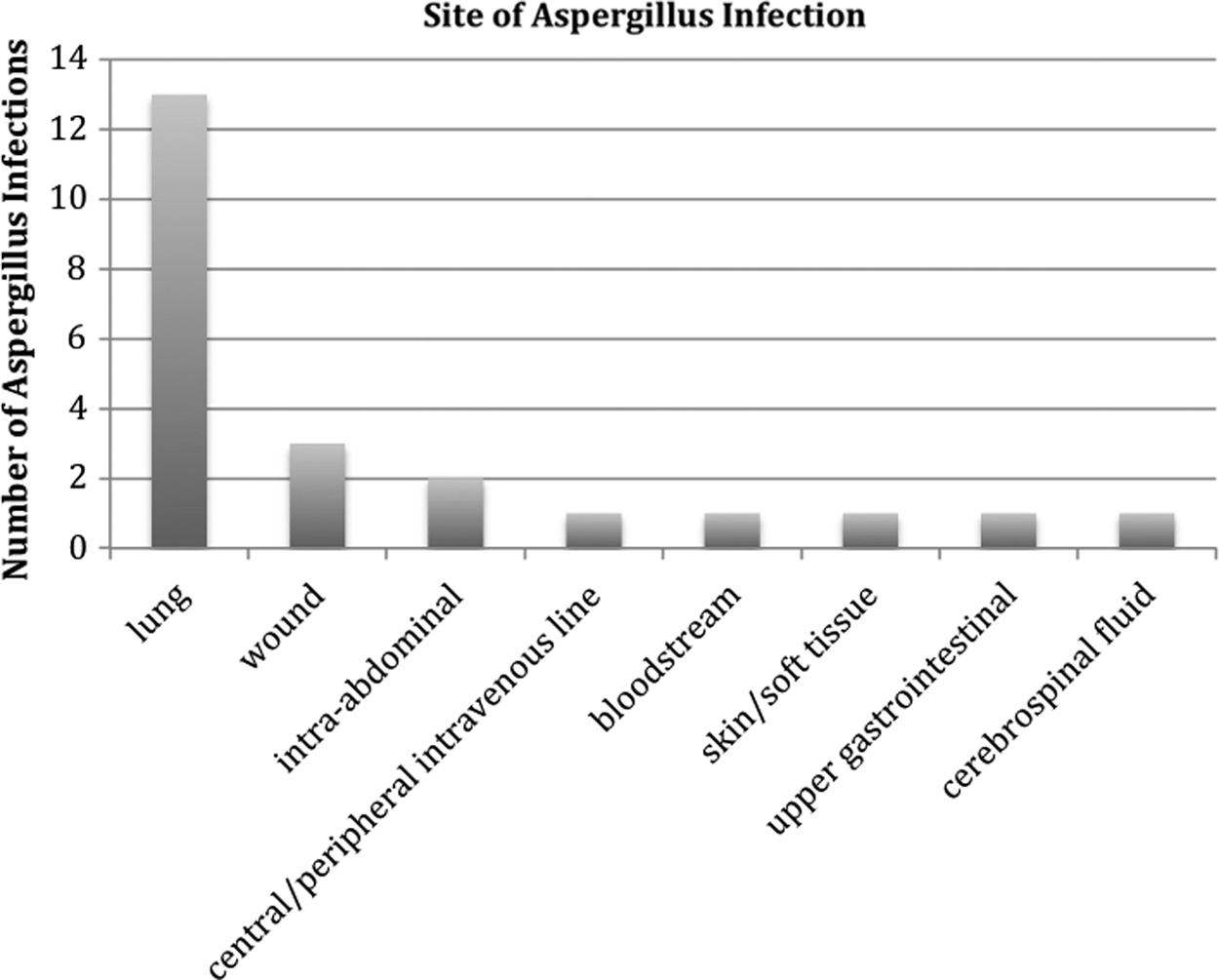
Sites of Aspergillus infection in study patients.
Of the 23 patients, 11 (48%) had functional abdominal organ transplants and 12 (52%) were non-transplant surgical patients. Approximately 200 total kidney, liver, and pancreas transplants are performed annually at our institution. Of the 11 infections in the transplant patients, eight were associated with liver transplants and two with kidney/pancreas transplants, and one occurred in a kidney transplant recipient. The two patient groups in the study were comparable with regard to age, BMI, WBC, temperature maximum, days from admission to antibiotic treatment, gender, and race. However, there was a significant difference between the two groups in their APACHE II scores, Acute Physiology Scores, steroid use, and number of Aspergillus-related infections acquired while in the ICU (Table 1).
Continuous data as mean±standard deviation.
All categorical data are presented as % (N).
ICU=intensive care unit.
The outcomes of the two patient groups were comparable (Table 2). The duration of antifungal treatment and hospital mortality were greater in the transplant patients and the number of days of hospitalization after initiation of antifungal treatment were greater in the non-transplant patients, although the differences were not statistically significant in either case. The numerically greater mortality for transplant patients may be explained by the greater severity of their illness as reflected by their mean APACHE II score (Table 1).
Continuous data as mean±standard deviation.
All categorical data as % (N).
Discussion
Historically, invasive aspergillosis was divided into the three groups of: 1) Proved invasive aspergillosis, 2) probable invasive aspergillosis, and 3) possible invasive aspergillosis, on the basis of a classification system developed in 2002 by the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) and restricted to patients immunocompromised as a result of hematologic malignant disease and/or stem cell transplant receipt (Table 3) [12].
AIDS=acquired immunodeficiency syndrome; GM=galactomannan.
Although the algorithm described above (Algorithm for Defining Aspergillosis in Immunocompromised Patients) pertains to immunocompromised patients, our data emphasize the need to consider the possibility of aspergillosis in non-immunocompromised patients. Recognition of this will allow more rapid initiation of appropriate treatment for aspergillosis, expedient diagnosis and the implementation of appropriate therapy for aspergillosis have a favorable impact on survival. More specifically, one study showed that a delay in treatment of more than 10 d after the onset of pneumonia resulted in a mortality of 90%, as opposed to a mortality of 40% when treatment was initiated within 10 d [13].
Invasive aspergillosis in the immunosuppressed population has a predicted mortality of 30%–85% [2]. As noted earlier, aspergillosis has been a disease associated most commonly with hematologic malignant disease (acute leukemia), hematologic stem cell transplant (HSCT) receipt, and solid-organ transplantation [2,6]; however, there has more recently been an observed increase in the incidence of Aspergillus infection among patients who lack these classic risk factors, and a recognition of its appreciable lethality. A recent review of invasive fungal infections in critically ill patients with similar Simplified Acute Physiology Scores showed that aspergillosis was responsible for the highest crude mortality, of 63% [14]. Conditions associated with aspergillosis in these “non-immunosuppressed patients” include chronic obstructive pulmonary disease (COPD), immunoparalysis secondary to sepsis, diabetes mellitus, chronic kidney disease, surgery, and steroid treatment [7,8,15–17]. Our study population was characterized by diabetes, acute kidney injury requiring dialysis, ventilator dependency, malignant disease, trauma, underlying lung disease, and blood transfusion. All of these conditions demonstrate the association between aspergillosis and critical illness, and the immunosuppression induced by aspergillosis itself.
Similarly, a recent study of the mortality attributable to invasive aspergillosis in critically ill patients in medical ICU settings found that such patients were more likely to experience acute kidney injury, longer ICU stays, more extended periods of mechanical ventilator dependency, and higher mortality (an attributable mortality of 18.9%) than critically ill patients without invasive aspergillosis [18]. However, our data are the first to focus specifically on surgical patients, and demonstrate that they, too, are susceptible to this disease.
Additionally, we noted similar mortality among transplant and non-transplant patients despite significantly higher APACHE II and Acute Physiology Scores in the transplant group. This may be attributable to renal transplant recipients having comprised 25% (n=3) of our transplant recipient population. A study done by Sawyer et al. in 1995 found that while although APACHE II scoring may be useful in predicting the outcomes of post-operative liver transplant recipients, it consistently over-predicted mortality in renal transplant recipients [19]. Other studies have shown that APACHE II scores predict questionable mortality rates in individual surgical patients as compared with larger patient cohorts, for which it becomes more accurate. This especially holds true for trauma patients, for whom APACHE II scores may undersestimate the predicted mortality rate, owing to a younger population without the chronic health problems seen in an older population [20,21]. Thus, in a hospital of moderate size such as ours, surgeons caring for critically ill patients may expect to treat a fair number of non-transplant patients with aspergillosis with outcomes similar to those of transplant recipients.
Limitations of our study include its having been a retrospective cohort analysis and thus subject to selection bias, potentially confounding the interpretation of outcomes for the two study groups. This was a single-center study, and as a result its external validity may be limited in generalizing its results to other areas in which the demographics and co-morbidities may differ from those of our patient population. The small population size of our study limits its statistical power, which in turn increases the risk of a type II error (the odds of stating that there is no treatment effect when in fact there is one). Additionally, the small population size of the study limited our ability to perform a multivariable analysis and thus analyze more closely discrepancies between the transplant and non-transplant groups with regard to pre-operative risk factors and co-morbidities. Lastly, our exclusion of lung transplant recipients limits our ability to compare incidences of colonization, infection, and mortality related to aspergillosis in lung transplant recipients with those of other solid-organ transplant recipients, as well as with the non-transplant groups. Multiple studies have shown that lung transplant recipients experience a higher incidence of aspergillosis than do recipients of other solid-organ transplants. This, coupled with the poor radiographic imaging resulting from post-operative changes in lung-transplant recipients, has prompted the recommended use of antifungal prophylaxis in this population [22–26]. Other studies have demonstrated a difference in the time of onset of infection and death among lung-transplant recipients, with patients experiencing Aspergillus infections of late-onset having a significantly higher mortality than those with infections of early onset [25]. It would be difficult to predict how these patients might fit within our study population, given that our patients were followed only during their initial hospitalization. Presumably, mortality for our transplant group would underestimate the true mortality if the period from onset of infection to death were included.
Conclusions
It is clear that the stereotypical symptoms of chest pain and hemoptysis, combined with the radiographic halo sign or crescentic cavitation of pulmonary aspergillosis may not be present in non-immunocompromised patients. Instead, the presentation of aspergillosis in this population may be more akin to that of antibiotic-resistant pneumonia or exacerbation of COPD, with radiographic imaging showing persistent or rapidly developing infiltrative abnormalities despite antibiotic treatment, or bronchoscopy showing erythema, ulcerations, nodules, or pseudomembranes [6,15]. When these signs and symptoms occur in the setting of critical illness, prolonged hospitalization, ICU admission, an extended period of mechanical ventilator dependency, COPD, or multiple medical co-morbidities, a culture positive for Aspergillus should not be disregarded as a contaminant, and additional studies for Aspergillus infection should be done. Persistently positive cultures in the setting of suspicious findings on chest imaging suggest that treatment for aspergillosis should be initiated.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest.