Kennemer Gasthuis Haarlem Netherlands
St. Vincent's University Hospital, Dublin, Ireland
OVERTREATMENT OF COLONIC DIVERTICULITIS: A PLEA FOR A LESS AGGRESSIVE APPROACH
Background: Despite the fact there still is controversy about the appropriate management of the various stages of diverticulitis and its complications, one cannot help but noticing a shift away from invasive, operative treatment for both complicated and uncomplicated disease towards a less aggressive, non-operative approach. This shift is congruent with expanding evidence on optimal treatment and an increasing understanding diverticulitis comprises different disease entities with heterogeneity between patients.
Aim: In this study we present an overview of the development in treatment of colonic diverticulitis and address the available evidence for contemporary operative and non-operative management.
Methods: Literature search in Medline and Embase.
Results: The standard of care for perforated or complicated diverticulitis evolved from a Hartmann's procedure, to resection and primary anastomosis, to treatment with antibiotics and percutaneous drainage in a carefully selected patient subset. Recently laparoscopic lavage emerged as a promising treatment for Hinchey 3 cases. Likewise for uncomplicated diverticulitis the approach is becoming less aggressive with a change from intravenous antimicrobial therapy, starvation and admission, to oral antibiotics and finally to observation and outpatient treatment.
Conclusions: One might say we overtreated the majority of diverticulitis patients for decades. Avoidance of overtreatment has obvious benefits: less in hospital treatment, cost reduction, less antimicrobial resistance, reduction in complication rate and side effects and presumably a better quality of life. In the nearby future hopefully several unanswered questions regarding the pathogenesis and optimal management of different diverticulitis stages will be answered by various ongoing trials.
Skåne University Hospital, Malmö, Sweden
ADHESIVE SMALL BOWEL OBSTRUCTION FOLLOWING OPEN VERSUS LAPAROSCOPIC SURGERY FOR SUSPECTED APPENDICITIS—IS THERE A DIFFERENCE IN INCIDENCE?
Background: Appendicitis is a common surgical diagnose with a lifetime risk of approximately 7%. Appendectomy is the treatment chosen for most patients. Postoperative adhesions are common following abdominal surgery including appendectomy.
Aim: The aim of the present study was to compare the frequency of readmission for small bowel obstruction following open surgery versus laparoscopic surgery for suspected appendicitis.
Methods: All patients, >/=16 years, who had open appendectomy performed at Skåne University Hospital in Lund and all patients (same age) that underwent laparoscopic surgery for suspected appendicitis at Skåne University Hospital in Malmö between 1992 and 2007 were included. All patients' charts were retrospectively and individually studied and followed up until the end of 2009. Rehospitalization for small bowel obstruction, >/=30 days after index surgery, were registered.
Results: 2332 patients in the open group (OG) and 2372 patients in the laparoscopic group (LG) were included. The frequency of readmission leading to hospitalization for small bowel obstruction was low in both groups. A difference between the groups (0.7% in the OG and 0,3% in the LG) were identified but showed no statistical significance, p=0.06.
Conclusions: There was no significant difference in readmission between the two groups. There was a tendency towards less postoperative small bowel obstruction following laparoscopic surgery for suspected appendicitis.
AnderssonB1Andrén-SandbergÅ2NilssonJ3AnderssonR1
Department of Surgery, Skåne University Hospital, Lund, Sweden
Department of Surgery, Karolinska University Hospital, Stockholm
Department of Cardiothoracic Surgery, Skåne University Hospital, Lund, Sweden
Department of Surgery, Skåne University Hospital, Lund, Sweden
SURVEY OF THE MANAGEMENT OF ACUTE PANCREATITIS IN SWEDEN
Background: Several international guidelines concerning treatment of acute pancreatitis (AP) has been published during the last decades. However, Scandinavian guidelines are still missing.
Aim: The aim was to identify current treatment strategies for AP in Sweden, and to evaluate if there is a need for improvement.
Methods: A questionnaire was e-mailed to the surgical department at all Swedish hospitals (n=58) taking care of patients with AP. Comparisons were made between university and non-university hospitals, and between hospitals with a primary catchment area of more versus less than150,000 persons.
Results: Fifty-one hospitals responded (88%). In median 65 (12-200) patients with AP are treated yearly at each hospital. 18/51 performs a severity classification, with APACHE II being the most commonly used. A majority is of the opinion that a scoring system is not better than the judgement of a senior consultant. In severe AP, 29/48 administer antibiotics, 29/48 enteral nutrition and 25/49 have a standardized follow-up plan. In 29 hospitals ≥1 necrosectomies are performed yearly. The majority considered administration of intravenous fluids as the most important treatment in severe AP. After mild biliary AP, the corresponding answer was cholecystectomy, being more common at larger hospitals (p=0.002). 42/47 hospitals were interested in creating a Scandinavian quality register.
Conclusions: The results from this first Swedish national survey give a clear insight in current traditions of treatment of AP. We identified a lack of early severity stratification, limited use of enteral nutrition, and difference in standard care between hospitals.
BakaSGiokasGTsoumaILogothetisEYiallourouAKouskouniEVorosD
Department of Biopathology and 2nd Department of Surgery, Aretaieion Hospital, University of Athens, Athens, Greece
PATHOGENS ISOLATED FROM CENTRAL VASCULAR CATHETERS IN PATIENTS WITH POSITIVE BLOOD CULTURES
Background: The use of central vascular catheters (CVC) became essential to modern medical practice, especially in the intensive care units (ICU).
Aim: The aim of this study was to evaluate the etiology of CVC-related infections in patients with positive blood cultures.
Methods: Catheter tips from patients hospitalized during January 2008 to October 2010 were processed using the semiquantitative method and blood cultures were incubated in the automated BACTEC 9050 System (Becton Dickinson, USA). The positive blood cultures and the CVC were cultured under standard conditions. The identification of the isolated microorganisms and their susceptibility to different antimicrobial agents was performed using the automated system VITEK 2 (BioMerieux, Marcy l'Etoile, France).
Results: Samples from 127 CVC obtained from different patients were evaluated (42 in 2008, 58 in 2009 and 27 in 2010). Positive cultures were found in 115 (90.6 %) of cases [39 (92.9%) in 2008, 50 (86.2%) in 2009, and 26 (96.3%) in 2010]. Blood cultures were available from all patients studied. Out of the 115 positive CVC cultures, 96 (83.5%) yielded the same microorganism as from the blood culture, while in 19 (16.5%) cases a different pathogen was isolated in the blood culture. Out of the 96 cultures yielding the same pathogen with the blood cultures, gram-negative bacteria as well as Gram-positive cocci were isolated in the same percentage, 48%, while the remaining 4% was represented by fungi.
Conclusions: In the majority of cases, the same microorganisms were isolated from both CVC and blood cultures.
AnderssonBAppelgrenBSjödinVAnsariDTingstedtBAnderssonR
Lund University, Sweden
HEALTH CARE-RELATED COSTS IN ACUTE PANCREATITIS
Background: Acute pancreatitis (AP) can be everything from a mild to a fulminant disease with high morbidity and mortality.
Aim: The aim was to calculate total health care-related costs for AP.
Methods: All patients belonging to the primary catchment area of Skane University Hospital, Lund, admitted for AP during 2009 and 2010 were retrospectively reviewed. The Atlanta classification was used for severity stratification. Template costs for hospital services were used to calculate the total medical costs.
Results: 276 patients with altogether 315 admissions were identified. Forty-three patients (16%) had severe AP (SAP). Thirteen patients (5%) died. Average length of stay (LOS) was 6 days (4-9) for mild AP (MAP) and 17 days (7-29) for SAP (p<0.001). Total hospital stay was 2936 days, including 1669 (57%) days in the ward, 1146 (39%) days in intermediary ICU and 121 (4%) days in the ICU. The overall hospital cost including admission, readmission and outpatient costs was in median € 5,870 (€2,700 - €8,850) for MAP and €18,900 (€ 8,370 - € 42,800) for SAP (p<0.001). When extrapolated to a national perspective, the annual cost for handling AP would be approximately €44,500,000; corresponding to €5,000,000 per million inhabitants.
Conclusions: The health care-related costs of especially SAP hospitalization are high. These results highlight the need to continue the identification and focus on this group, in order to try to limit organ failure and infectious complications.
Department of Clinical Sciences Malmö, Skåne University Hospital, Section of Surgery, Lund University
Department of Clinical Sciences, Vascular Excitation-Transcription Coupling, Lund University, Malmö
Department of Clinical Sciences, Molecular Metabolism, Lund University, Malmö Sweden
Department of Physiology, Nursing School, University of Extremadura, Caceres Spain
NFATc3 REGULATES TRYPSINOGEN ACTIVATION, NEUTROPHIL RECRUITMENT, AND TISSUE DAMAGE IN ACUTE PANCREATITIS IN MICE
Background: Acute pancreatitis (AP) is an inflammatory disease with a wide clinical spectrum. Elevated cytosolic calcium, trypsinogen activation and inflammation are key components in the pathophysiology of AP but the molecular mechanisms leading to the initiation and propagation of these events are still unclear.
Aim: To explore the potential involvement of the calcium/calcineurin-dependent transcription factor nuclear factor of activated T- cells (NFAT) in AP.
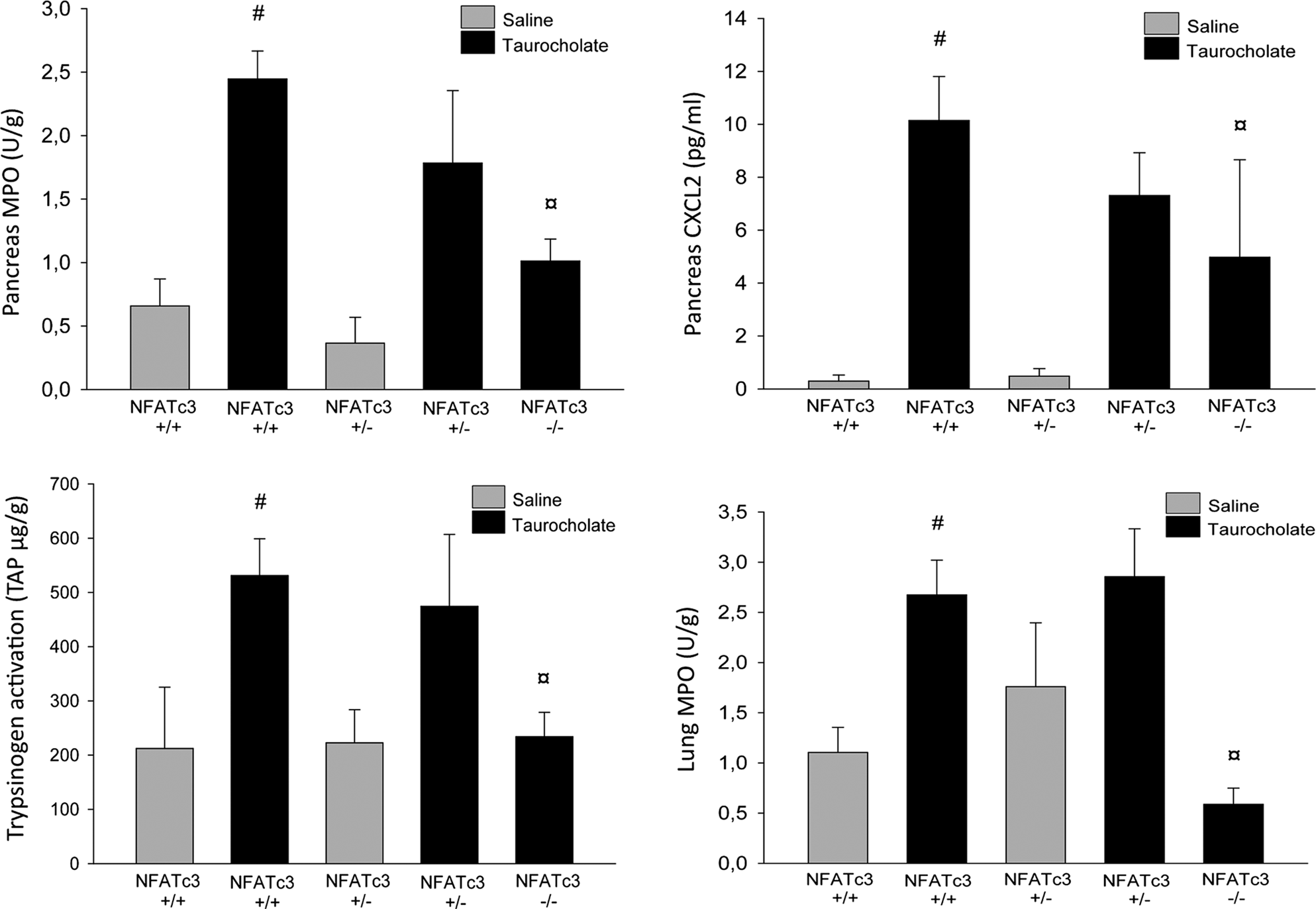
Methods: Retrograde infusion of sodium taurocholate into the pancreatic duct of mice caused a severe AP characterized by elevated blood amylase, pancreas and lung myeloperoxidase (MPO), pancreas macrophage inflammatory protein-2 (CXCL2), trypsinogen activation and severe tissue destruction (acinar cell necrosis, edema, leukocyte infiltration and hemorrhage) in the pancreas.
Results: In transgenic NFAT-luciferase (NFAT-luc) reporter mice NFAT-dependent transcriptional activity was significantly increased in pancreas, as well as in aorta, lung and spleen after taurocholate challenge. Treatment with the NFAT inhibitor A-285222 completely blocked taurocholate-induced NFAT activation in all organs and led to restored levels of inflammatory mediators as well as preserved tissue architecture. Similarly, NFATc3-deficient mice were protected from taurocholate-induced trypsinogen activation, inflammation and destruction of pancreatic tissue. Secretagogue-induced activation of trypsinogen in acinar cells ex vivo was also NFAT-dependent, since pharmacological inhibition with A-285222 or lack of NFATc3 protein abolished the response.
Conclusions: Our data suggests that NFATc3 is a critical regulator of trypsinogen activation, neutrophil recruitment and pancreatic tissue damage and may be a potential therapeutic target in AP.
Effects 24 hours after taurocholate infusion in the pancreatic duct in wildtype (NFATc3+/+) and NFATc3 knock out mice. #=p<0.05 vs saline infused control and ¤=p<0.05 vs wildtype taurocholate challenged mice. Bars represent mean and SEM.
LeeuwenburghM1WiardaB2WiezerM3VrouenraetsB4GratamaJ5SpiltA6RichirM2BossuytP1StokerJ1BoermeesterM1
Academic Medical Centre, Amsterdam
Alkmaar Medical Centre, Alkmaar
Sint Antonius Ziekenhuis, Nieuwegein
Sint Lucas Andreas Ziekenhuis, Amsterdam
Gelre Ziekenhuizen, Apeldoorn
Kennemer Gasthuis, Haarlem Netherlands Academic Medical Centre, Amsterdam Netherlands
CAN MRI REPLACE CT IN ADULTS WITH SUSPECTED APPENDICITIS?
Background: Computed tomography (CT) is frequently used in patients with suspected appendicitis to substantiate clinical diagnosis but carries a risk of contrast nephropathy and radiation induced cancer. Magnetic resonance imaging (MRI) is an alternative imaging technique.
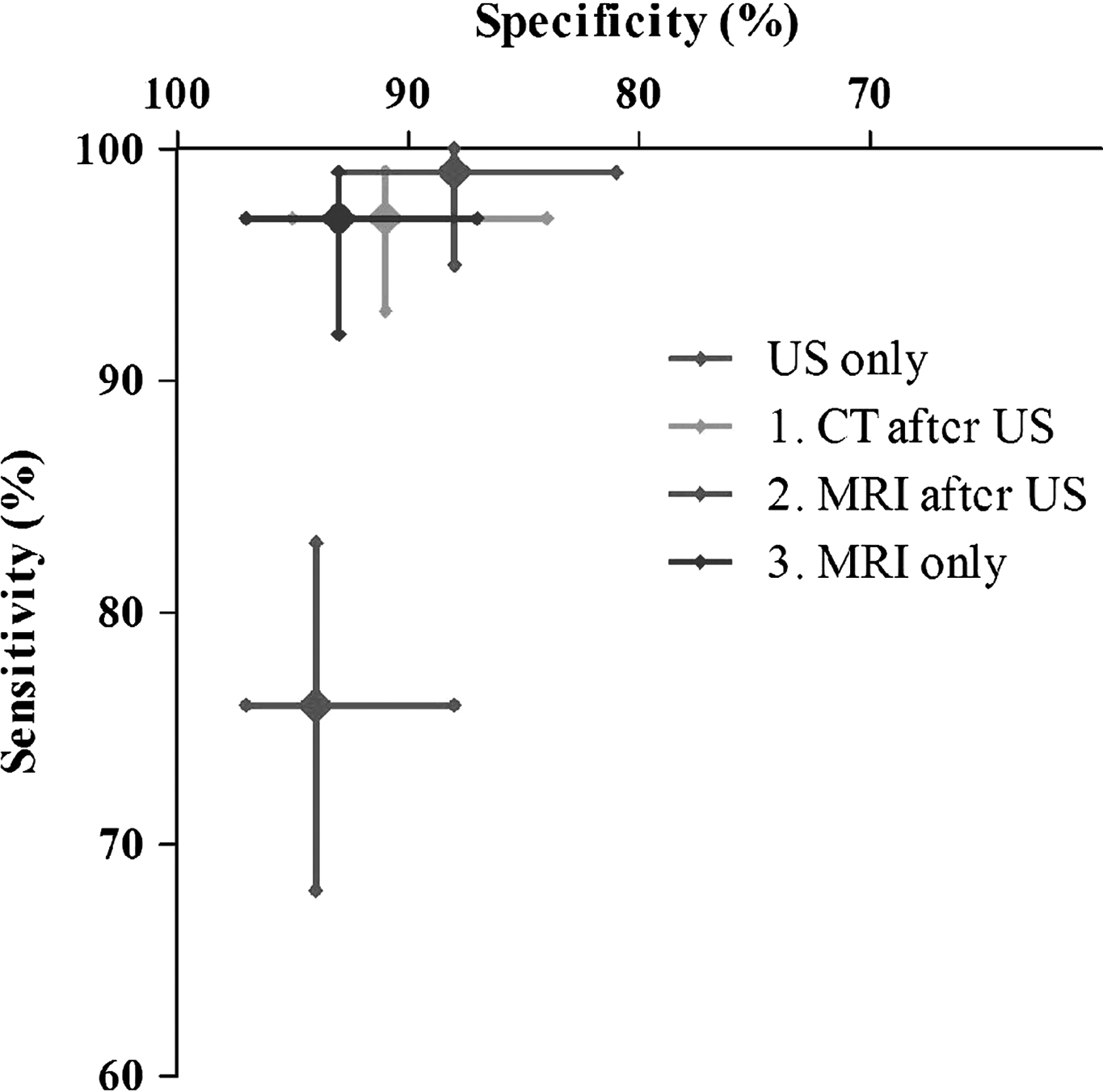
Methods: In a multicenter diagnostic accuracy study, adults with clinically suspected appendicitis were prospectively identified at the emergency department. Consenting patients underwent ultrasound (US) and subsequent CT if US was negative or inconclusive. Additionally, all patients underwent MRI, with the reader blinded for other imaging findings. An expert panel assigned final diagnoses after three months. We evaluated the accuracy of three imaging strategies: conditional CT after US, conditional MRI after US, and immediate MRI.
Results: We performed 229 US, 115 CT and 223 MRI examinations in 230 patients (median age 35, 40% male); appendicitis was the final diagnosis in 118 cases (51%). Conditional and immediate MRI had a sensitivity and specificity comparable to conditional CT, which resulted in 3% missed appendicitis (95% CI: 1 to 7%) and 8% false positives (95% CI: 4 to 14%). Conditional MRI missed appendicitis in 2% (95% CI: 0 to 6%) and generated 10% false positives (95% CI: 6 to 16%). Immediate MRI missed 3% appendicitis (95% CI: 1 to 8%) with 6% false positives (95% CI: 3 to 12%). Conditional strategies resulted in significantly more false positives in women than in men, whereas immediate MRI did not.
Conclusions: The accuracy of conditional or immediate MRI is similar to conditional CT in patients with suspected appendicitis. (Trial registration: NTR2148.)
V. B. HviidCSamulin ErdemJKunkeDAhmedSF. KjeldsenSWangYAttramadalHO.AasenA
Oslo University Hospital–Rikshospitalet, Norway
CYR61 IS REGULATED IN EXPERIMENTAL SEPSIS WITH MULTIPLE ORGAN DYSFUNCTION
Background: The presence of organ failure has a cumulative effect on sepsis-related death. The matri-cellular protein Cyr61 (CCN1) has been found to process organ-protective capabilities. Furthermore, mediators of sepsis-induced organ dysfunction are also potent regulators of CCN1 expression. This indicates a potential involvement of CCN1 in the development of sepsis-induced organ dysfunction.
Aim: To investigate CCN1 regulation simultaneously in the heart, lung, and liver of rats using a cecalligation and puncture (CLP) model.
Methods: 50 Wistar rats were subjected to 18 hours of CLP or Sham operation. Serum markers of organ function were measured. The organs were analyzed for CCN1 mRNA and protein expression, in addition to cytokine and chemokine mRNA expression. For molecular studies of CCN1 regulation, a human hepatocarcinoma cell line (HepG2) was used.
Results: The inflammatory genes were severely induced in the liver and lungs, while little activated in the heart. The measured serum markers of organ affection confirmed significant hepatic and pulmonary impairment.
CCN1 mRNA was induced in liver and lungs but unaffected in the heart. Moreover, hepatic and pulmonary CCN1 mRNA expression patterns mimicked that of the inflammatory markers and a close statistical correlation was observed between the two. To address this potential relationship, HepG2 cells were exposured to TNF. By this treatment, HepG2 cells responded with a specific and dosage-dependent CCN1 mRNA response.
Conclusions: This study provides novel evidence for CCN1 regulation in sepsis. Moreover, it implies for a role of inflammatory cytokines in provoking CCN1 regulation.
KlarinB1AdolfssonAJeppssonB2
Society of Anaestesiology and Intensive Care Swedish Surgical Society Sweden
PROPHYLACTIC USE OF PROBIOTICS FOR REDUCTION OF SECONDARY INFECTIONS
Background: Avoiding secondary infections for surgical as well as for other patient categories is a major issue for the intensivist. As the frequency of multi resistant bacteria is increasing and driven by the use of antibiotics, the demand for alternative and complementary treatments and prophylaxis increases. The easiest way of treating an infection is by avoiding it. Effective prophylactic procedures result in fewer infections.
Ventilator associated pneumonia (VAP) is a frequent complication to intensive care and causes increases in human suffering, costs, prolonged ICU and hospital stay, and prolonged antibiotics therapies. Aspiration of infected secretions from the oropharynx to the lungs is the main cause of VAP and reduction of pathogenic bacteria through oral care is of vital importance.
Aim: To compare the effectiveness of an established procedure for oral care to an ecologic alternative procedure.
Methods: Prospective randomized multicenter study. The established use of the antiseptic chlorhexidine (CHX) soaked swabs is compared to the application of the probiotic bacterium Lactobacillus plantarum 299. Cultures from oropharynx and tracheal secretions are analyzed. Daily routine chemistry.
Results: Demografic and ICU-admission data are similar. CRP is lower in the probiotic group from day 3. Difference is not significant; WBC values are similar. In the CHX group, emerging pathogens were cultured from 57% cent in oropharyngeal samples and 38% in the probiotic group.
Conclusions: This biologic method is at least as effective as the established procedure using the antiseptic chlorohexidine in prohibiting emerging enteric bacteria to establish in the oropharynx.
PeterssonU1NobaekS2MontgomeryA1
Lund University, Sweden
University of Copenhagen, Denmark
INFECTED SYNTHETIC MESHES AFTER INCISIONAL HERNIA MESH REPAIR CAN BE SALVAGED USING NEGATIVE PRESSURE WOUND THERAPY (NPWT)
Background: Mesh-infection has often led to mesh-explantation in order to cure infection and heal the wound. NPWT has become commonplace in treatment of difficult wounds but reports on NPWT of infected meshes are few.
Aim: The aim was to evaluate the result of NPWT of mesh-infection.
Methods: Records for patients treated with NPWT, after incisional hernia repair during 2010, were reviewed retrospectively.
Results: Eleven patients (10 females and one male), with heavy-weight polypropylene mesh repair were included. Ten healed while because one patient still has a small wound residue after two years, which has recently been revised and sutured since severe concomitant disease prevented earlier intervention. Four of the five secondary sutured patients healed without complications and one had a small wound relapse that healed after a month. In the other five successfully healed patients, NPWT was terminated when fresh granulations were encountered and the treatment continued with other wound dressings. All patients had positive cultures at the time of initiating NPWT and also at the time NPWT was terminated, including the patients whose wounds were secondary sutured. No mesh was partially or totally explanted.
Conclusions: Infected mesh can be salvaged with NPWT. Median time needed for wound healing was almost four months in the total group. Secondary suturing of the wound seems to shorten time to healing without major complications. We propose a regimen of initial NPWT and secondary suture as soon as granulation tissue is present in a macroscopically clean wound.
Median (range)
Age (years)
60 (23–82)
BMI (kg/m2)
33 (27–66)
Interval hernia repair-NPWT start (days)
16 (0–62)
NPWT (days)
53 (13–69)
NPWT dressing changes (n)
15 (5–22)
Total time to healing (days), n=10
117 (31–167)
Healing time for secondary sutured (days), n=5
72 (31–105)
Healing time not secondary sutured (days), n=5
149 (57–167)
DepreeuwM1Van NieuwenhoveY2De WaeleJ1
Dept of Critical Care Medicine, Ghent University Hospital
Dept of Surgery, Ghent University Hospital, Belgium
CHARACTERISTICS OF CLINICAL STUDIES EVALUATING ANTIBIOTIC THERAPY FOR INTRA-ABDOMINAL INFECTIONS: ASYSTEMATIC REVIEW
Background: Multiple studies have been performed to determine the efficacy of antimicrobial agents in treating IAI, but there may be considerable variation in infections included as well as reporting of these studies.
Aim: To analyze prospective studies on antibiotic treatment of IAI and compare patients and infections included, as well as evaluate the reporting in the studies.
Methods: A PubMed search (1949-2010) was used to identify prospective studies on the antibiotic treatment of IAI. These studies were evaluated for specific criteria such as inclusion criteria and patient and infection characteristics, as well as the reporting of these and outcome parameters.
Results: 74 studies were included in the analysis. Detailed reporting of the focus of infection was absent in 26% of the studies. When reported, the focus of IAI was highly variable, with the appendix being the most frequent focus (39%±21.2%). Only 33 studies (46%) reported outcomes of the microbiological evaluable population. Median success rate was around 86% (IQR 78%-93%). Severity of illness was specified in 48 studies (65%), but overall severity was low.
Conclusions: In studies on IAI, there is considerable variability in included patients and diseases, and multiple deficits exist in the reporting of the data. This limits proper interpretation of some studies, makes comparison of several studies difficult and restricts application of the results of these trials in clinical practice.
RahmanMZhangSZhangSChewMSykIJeppssonBThorlaciusH
Clinical Sciences, Malmö, Lund University, Sweden
PLATELET SHEDDING OF CD40L IS REGULATED BY MATRIX METALLOPROTEINASE-9 (MMP-9) IN ABDOMINAL SEPSIS
Background: Platelet-derived CD40L regulates neutrophil recruitment and lung damage in sepsis. However, the mechanism regulating shedding of CD40L from activated platelets remains elusive.
Aim: We hypothesized that MMP-9 might cleave surface expressed CD40L and regulate pulmonary accumulation of neutrophils in sepsis.
Methods: Wild-type and MMP-9 gene-deficient male C57BL/6 mice were exposed to cecal ligation and puncture (CLP). Edema formation, CXC chemokine and MPO levels and neutrophils in the lung as well as plasma levels of CD40L and MMP-9 were quantified. Flow cytometry was used to determine surface expression of CD40L and MMP-9 on platelets.
Results: CLP increased plasma levels of MMP-9 but not MMP-2. The CLP-induced decrease of platelet surface CD40L and increase of soluble CD40L levels were attenuated in MMP-9-deficient mice. Pulmonary MPO activity and neutrophil infiltration in the alveolar space as well as edema formation and lung injury were markedly decreased in septic animals lacking MMP-9. In vitro studies revealed that activated platelets up-regulate surface expression of MMP-9 and that inhibition of MMP-9 decreased platelet shedding of CD40L. Recombinant MMP-9 was capable of directly cleaving surface expressed CD40L on activated platelets.
Conclusions: Thus, our novel data propose a novel role of MMP-9 in regulating platelet-dependent infiltration of neutrophils and tissue damage in septic lung injury by controlling CD40L shedding from platelets.
SmirnovD
Chelyabinsk State Medical Academy, Russia
PLASMA ENDOTOXINS AND PREOPERATIVE SYSTEMIC INFLAMMATION AS EARLY DIAGNOSTIC PREDICTORS OF POSTOPERATIVE INFECTIOUS COMPLICATIONS IN PATIENTS UNDERGOING RESECTIONS FOR INTESTINAL CARCINOMA
Background: The presence of systemic inflammation before surgery predicts poor long-term survival in cancer patients. However, few studies have investigated the relationship between preoperative systemic inflammatory response and postoperative complications in the field of intestinal cancer surgery.
Aim: Our aim was to evaluate the significance of preoperative systemic inflammatory response on postoperative infectious complication of patients with intestinal cancer.
Methods: 105 consecutive patients who were to undergo elective resection for intestinal carcinoma were investigated within 2 years. Blood samples was obtained at the time of patients admission and daily after surgery for measuring interleukins-1β, −6, C-reactive protein. Plasma levels of endotoxin (LPS) were measured from the same time using the LAL endotoxin scattering photometry. The systemic inflammatory response was classified on the basis of admission data according to the standard methods.
Results: After surgery, 12 (11,43%) patients developed a postoperative infectious complication, which was diagnosed on postoperative days 4-9. Univariate analysis revealed that the expressiveness of preoperative systemic inflammatory response was the most sensitive predictor of postoperative infectious complication (odds ratio, 2.775; P=0.0063). Multivariate analyses using factors including pre- and postoperative serum LPS levels, operation time, distant metastasis and systemic inflammatory response revealed that systemic inflammatory response (odds ratio, 2.462; P=0.0257) and preoperative serum LPS levels (odds ratio, 2.589; P=0.0167) were associated with a postoperative infection.
Conclusions: Preoperative systemic inflammatory response and preoperative serum LPS levels may be an additional early diagnostic predictors of postoperative infectious complications in patients undergoing resection for intestinal cancer.
YokoyamaYMizunoTSugawaraGAsaharaTNomotoKNaginoM
Nagoya University Graduate School of Medicine, Department of Surgery, Division of Surgical Oncology; Yakult Central Institute for Microbiological Research Japan
INTRAOPERATIVE BACTERIAL TRANSLOCATION DETECTED BY BACTERIUM-SPECIFIC RIBOSOMAL RNA-TARGETED RT-QPCR FOR THE MESENTERIC LYMPH NODE STRONGLY PREDICTS POSTOPERATIVE INFECTION COMPLICATIONS
Background: There is a little evidence for the association between bacterial translocation (BT) and postoperative infectious complication (POIC) following major hepatectomy.
Aim: To investigate correlation between the occurrence of BT in the mesenteric lymph node (MLN) sampled during surgery and POIC.
Methods: Patients who underwent major hepatectomy for biliary malignancies involving (n=65) were included in this study. Mesenteric lymph nodes (MLNs) in the jejunum were harvested at two times during the operation (MLN-1, harvested immediately after laparotomy; MLN-2, harvested after tumor resection). Microorganisms were detected by a bacterium-specific rRNA-targeted RT-qPCR method. Perioperative factors and POIC were recorded prospectively.
Results: Among 65 patients, 51 completed the study. Microorganisms were detected in MLN-1 and MLN-2 in 15 patients (29.4%) and 19 patients (37.3%), respectively. The detection of microorganisms in MLN-1 was significantly correlated with the incidence of preoperative cholangitis (P=0.04). The detection of microorganisms in MLN-2 was significantly correlated with the incidence of POIC (P=0.002). Among 19 patients with positive microorganisms in MLN-2, 11 patients (58%) developed POIC. On multivariate analysis, a positive microorganism in MLN-2 was one of the independent predictive factors of POIC (odds ratio 26.1, P=0.012).
Conclusions: Intraoperative analysis of MLN-2 by rRNA-targeted RT-qPCR strongly predicts the occurrence of POIC following hepatectomy of biliary malignancy. This method is more sensitive and rapid than the conventional culture method. Therefore, we can easily select the group of patients with high risk for POIC.
Toyota Kosei Hospital
Tokai Hospital
Yamashita Hospital
Chubu Rosai Hospital
Yachiyo Hospital
Shizuoka Saiseikai General Hospital, Japan
RISK FACTORS FOR INCISIONAL HERNIA IN ASSOCIATION WITH SURGICAL SITE INFECTIONS IN ABDOMINAL SURGERY: A LARGE MULTIPLE-INSTITUTIONAL PROSPECTIVE STUDY
Background: Incidence rate of incisional hernia (IH) in associated with surgical site infection (SSI) after abdominal surgery is not fully investigated.
Aim: The purpose of this study was to identify risk factors for IH in abdominal surgery, especially in association with SSIs.
Methods: From November 2009 to February 2011, we prospectively collected 3892 consecutive patients who underwent abdominal surgery for gastrointestinal, colorectal, and hepato-biliary-pancreatic diseases in the Division of Surgical Oncology, Department of Surgery, Nagoya University, and 18 affiliated hospitals. Patients were followed up for >180 days after operation to evaluate the incidence of SSI and incisional hernia.
Results: The incidence of overall SSI, superficial/deep incisional SSI (SD-SSI), and organ space SSI were 18.5%, 9.0%, and 10.9%, respectively. Wound dehiscence occurred in 350 patients (9.0%), and most of these patients had concomitant SD-SSI. Postoperative IH within 180 days occurred in 127 patients (3.3%). In univariate analysis, risk factors for IH were age, body mass index, American Society of Anesthesiology score, history of making colostomy, previous usage of anticancer drugs, emergency operation, wound classification, blood transfusion, suture materials for fascial closure, incidence of SDSSI, and depth of wound dehiscence. Independent risk factors for IH by multivariate analysis were age, suture materials for fascial closure, depth of wound dehiscence, and body mass index.
Conclusions: To reduce the incidence of incisional hernia, it is crucial to prevent SD-SSI and wound dehiscence.
KacelnikOEriksenHLøwerHSkjeldestadF
National Institute of Public Health, Norway
SURGICAL SITE INFECTIONS FOLLOWING CHOLECYSTECTOMY IN NORWAY 2006–2010
Background: Since 2005 The Norwegian Surgical Site Infection (SSI) register has collected data on SSI related risk factors and patient outcomes on all cholecystectomies performed during a defined three month period each year by participating hospitals.
Aim: To use register data to identify SSI risk factors following cholecystectomy. This was In order to determine whether infections proportions were In line with international standards and to identify specific risk factors to promote better care.
Methods: Data comprised all cholecystectomies registered between 2006 and 2010. End points were either infection within 30 days, death or being infection free at 30 days post-surgery.
Results: Twenty-seven hospitals have contributed data on over 1900 (1684 fully followed-up) patients over five years. Infection rates were 7% for laparoscopic operations (n=1567) and 9% for open procedures (n=117). 85% of SSIs were found after hospital discharge. Univariate analysis revealed no effect of sex, acute/elective, day-surgery, prophylactic antibiotic use or laparoscopy on infection rates. Infections were also not predicted by NNIS risk stratification or hospital type.
Conclusions: Norwegian infection rates following cholecystectomies are in line with international rates. At present we do not have a good statistical way of stratifying patients by risk of infection. It appears that neither the type of hospital nor the hospital itself is a factor. The high proportion of infections found post discharge suggest that keen follow-up is needed. Lastly, there is a need more information about comorbidities to accurately target at-risk groups.
Nagoya Daiichi Red Cross Hospital
Nagoya Daini Red Cross Hospital
Handa City Hospital
Tsushima City Hospital
Chukyo Hospital
University of Nagoya, Japan
RISK FACTORS FOR SURGICAL SITE INFECTION IN ABDOMINAL SURGERY IN JAPAN. A MULTI-INSTITUTIONAL PROSPECTIVE STUDY
Background: The incidence of surgical site infection (SSI) has a great impact on patients' outcome and economic perspective.
Aim: The purpose of this study was to identify risk factors for SSI in abdominal surgery by performing a large multiple-institutional prospective data collection.
Methods: From November 2009 to February 2011, we prospectively collected 4305 consecutive patients who underwent abdominal surgery for gastrointestinal, colorectal, and hepato-biliary-pancreatic diseases in the Division of Surgical Oncology, Department of Surgery, Nagoya University Graduate School of Medicine, and 18 affiliated hospitals.
Results: The Incidence of overall SSI, superficial/deep incisional SSI (SD-SSI), and organ/space SSI (OSSSI) were 19.2%, 9.1%, and 11.7%, respectively. Postoperative hospital stay with overall SSI (38±27 days), SD-SSI (32±23 days), or OS-SSI (32±29 days) was significantly longer than that without any SSI (16±11 days). Independent risk factors for SD-SSI by multivariate analysis were liver cirrhosis, history of previous abdominal operation, emergency operation, wound length, usage of wound protector, and suture material for fascial closure. Independent risk factors for OS-SSI were male gender, American Society of Anesthesiology score, history of previous abdominal operation, operation time, blood loss, wound classification, and types of operation.
Conclusions: It is crucial to practice CDC guidelines as well as to make an effort to reduce operation time and blood loss, in order to prevent the incidence of SSI.
GarauJ1BlasiF2MedinaJ3ÁvilaM4McBrideK5OstermannH6
Hospital Universitari Mutua de Terrassa, Spain
University of Milan, Italy
AstraZeneca Spain
AstraZeneca Europe, Belgium
Instat Services, United States
University Hospital Munich, Germany, Hospital Universitari Mutua de Terrassa Spain
CURRENT MANAGEMENT OF PATIENTS HOSPITALIZED WITH COMPLICATED SKIN AND SOFT TISSUE INFECTIONS ACROSS EUROPE (2010–2011): ASSESSMENT OF PATIENTS WITH SURGICAL SITE INFECTION (RETROSPECTIVE STUDY TO ASSESS THE CLINICAL MANAGEMENT OF PATIENTS WITH MODERATE-TO-SEVERE CSSTI OR CAP INFECTIONS IN THE HOSPITAL SETTING [REACH] STUDY)
Background: Surgical site infections represent a significant burden in terms of patient morbidity and cost to health services worldwide. Outcomes and resource use are presented for surgical site infections recorded in REACH - a retrospective, observational cohort study designed to provide data on current clinical management of patients hospitalized with complicated skin and soft tissue infections (cSSTI) in European hospitals (NCT01293435).
Methods: Data were collected from 129 sites in ten European countries. The population comprised patients ≥18 years hospitalized between March 2010 and February 2011 with a cSSTI requiring intravenous antibiotic treatment. Variables were collected via an electronic Case Report Form.
Results: Of the total population (N=1996), 12.6% (n=252) of patients diagnosed with cSSTI had surgical site infections. The majority of these patients had been previously hospitalized (56.0%; n=141) or had invasive surgery (60.3%; n=152) in the 3 months prior to index visit, compared with 20.9% (n=418) and 14.0% (n=279) in the total population, respectively. Microbiological diagnosis (n=192) was similar to the total population, 65.6% (n=126) being infected with Gram-positive cocci; 65 Staphylococcus aureus infections (51.6%) and of those, 20 (30.8%) were methicillin-resistant. A further 40.6% (n=78) had Gram-negative pathogens.
Conclusions: Patients hospitalized with cSSTI resulting from surgery often experience complications, such as treatment failure to initial therapy, and require further surgery, increasing length of hospital stay and placing increased burden on hospital resources. These data highlight the need for reassessment of management regimens for this vulnerable patient group.
Surgical intervention after cSSTI diagnosis, n (%)
739 (37.0)
147 (58.3)
Development of septic shock during treatment, n (%)
55 (2.8)
8 (3.2)
ICU=intensive care unit; SD=standard deviation.
Need for antibiotic treatment modification.
Based on switch from IV to oral therapy.
Patients hospitalized again due to same cSSTI.
Rubio-PerezI1GallegoP2Martin-PerezE1FiguerolaA2LarrañagaE1
Department of General Surgery, La Princesa University Hospital, Madrid
Department of Preventive Medicine, La Princesa University Hospital, Madrid, Spain
AIMING FOR 0% SURGICAL SITE INFECTIONS: ARE STANDARDIZED PROTOCOLS USEFUL?
Background: Quality improvement techniques are being implemented in surgery as protocols, to reduce the incidence of infections.
Aim: In 2007, a standardized protocol was implemented in the General Surgery Department of our University Hospital in Madrid (Spain) to reduce surgical site infection (SSI) rates and improve the quality of patient care.
Methods: A prospective evaluation of the protocol's application was performed by the Department of Preventive Medicine. Variables included correct preoperative measures, administration of prophylaxis and rates of postoperative infection.
Results: With the application of the protocol, the global rate of infection in General Surgery patients decreased from 17% (2008) to 8% (2011) χ2 tend 52′3 p<0′001. SSI decreased from 13% (2008) to 6′7% (2011) χ2 tend 29′3 p<0,001. When compared with other institutions under a national quality control group (INCLIMECC), our results were below the national rates of SSI. Among the risk factors for infection, age>65, surgical time>120 minutes, emergency surgery and preoperative hospitalization>3 days were statistically significant. In 2011, the compliance of preoperative measures and correct prophylaxis reached 94%. Among the various interventions, one of the best results in adherence and SSI reduction was obtained with cholecystectomies, with a progressive yearly reduction of the SSI rate, reaching 1% in 2011.
Conclusions: The application of the standardized protocol significantly reduced the rate of SSI in our General Surgery Department. It also improved the compliance of prophylactic measures. The identification of factors associated with infection will allow further improvement in the future.
LøwerHEriksenHKacelnikOSkjeldestadF
Norwegian Institute of Public Health, Norway
SURVEILLANCE OF SURGICAL SITE INFECTIONS: WHAT IS MISSED AFTER HOSPITAL DISCHARGE?
Background: Surveillance of healthcare-associated infections is a cornerstone of prevention. Surveillance systems with feedback to surgeons may reduce rates of surgical site infections by around 20% in 4-5 years. The Norwegian Surveillance System for Healthcare-associated Infections (NOIS) was introduced by regulation in 2005.
Aim: The aim of this presentation is to describe the importance of following up patients after discharge from hospital in order to obtain a true picture of the burden of disease.
Methods: NOIS is based on the protocols published by European Centre for Disease Prevention and Control. It has an active, mandatory post-discharge follow-up by mail-in questionnaire after 30 days (one year for implants) following surgery. The surveillance system comprises: coronary artery bypass graft, cesarean section, hip arthroplasty, cholecystectomy, appendectomy (discontinued in 2009), and colon surgery (from 2009).
Results: The surveillance system volume has increased from 2371 procedures in 2005 to 6520 in 2010. 91% of the patients met our criteria for post-discharge follow-up being completed. 84% (1350/1608) of the infections were detected post-discharge. The mean number of days until infection for all surgeries was 13 whereas the mean postoperative length of stay was 5.5 days. Only 27% of these infections would have been detected by passive follow-up through readmissions and re-operations.
Conclusions: Post-discharge follow-up is important in order to detect all infections. Surveillance systems which do not include active post- discharge follow-up give an incomplete picture of the burden of surgical site infections.
ChaturvediALommeRHendriksTVan GoorH
Radboud University Nijmegen Medical Centre, Netherlands
ULTRAPURE ALGINATE BASED GEL PREVENTS POSTOPERATIVE PERITONEAL ADHESIONS AS EFFECTIVE AS SODIUM HYALURONATE/CARBOXYMETHYLCELLULOSE MEMBRANE (SEPRAFILM™)
Background: Abdominal surgery inevitably leads to peritoneal trauma. Peritoneal trauma, how insignificant it may seem, leads to the formation of adhesions. Complications of adhesion formation include intestinal obstruction, infertility, and prolonged surgical time. Different tissue separating barriers have been developed, all being effective in research settings; a few demonstrated significant efficacy in human trials.
Aim: To assess the adhesion reducing properties of a new ultrapure alginate gel in comparison with the gold standard bioresorbable membrane (Seprafilm®).
Methods: 72 male Wistar rats underwent laparotomy. The cecum was exteriorized and the cecal wall was abraded with 20 strokes of surgical gauze and a 1×2 cm area of the peritoneal sidewall opposite the injured cecum was excised exposing the abdominal wall muscle. The abraded cecum was sutured in place to the abraded region on the peritoneal sidewall with two sutures at the edges. The rats were randomly assigned to one of the following groups: Controls (n=29), ultrapure alginate gel (n=29) and Seprafilm™ (n=14). At day 14, adhesions were scored in a blinded fashion using a scoring method comprising type, extent, and tenacity. The sum of the three scores was used as the total adhesion score.
Results: 24.1% (7/29) in the control group had no adhesions, whereas 86.2% (25/29) in the ultrapure alginate gel group and 85.7% (12/14) in the Seprafilm™ group had no adhesions. ( P<0.0001 for alginate gel vs. control, P<0.0007 for Seprafilm™ vs. control.
Conclusions: Ultrapure alginate gel decrease the incidence of postoperative adhesions in rats.
Comparison of Ultrapure alginate gel and Seprafilm™ for reducing primary postoperative adhesions
Groups
Adhesion score (mean±SD)
Tenacity of adhesions (mean±SD)
Extent of adhesions (mean±SD)
Total scores (mean±SD)
Control (n=29)
1.93±1.43
2.1±1.47
2.06±1.66
6.09±4.5
Alginate gel (n=29)
0.34±0.93
0.37±1.01
0.17±0.46
0.88±2.4
Seprafilm (n=14)
0.35±0.92
0.35±0.92
0.30±0.85
1.01±2.69
ChenT1WangX2ZhouL1XieH1ZhengS1
Department of Hepatobiliary and Pancreatic Surgery, First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou
Biomedical Research Center, Zhongshan Hospital, Fudan University, Shanghai, China
DYNAMIC CHANGES OF PERIPHERAL REGULATORY B CELLS IN PATIENTS WITH HBV RELATED HEPATOCELLULAR CARCINOMA DURING PERIOPERATIVE PERIOD
Background: Regulatory B cells (Bregs) have been proved to be critical in the modulation of immune responses of chronic inflammatory states and cancer microenvironment. However alterations of Bregs of patients with Hepatitis B (HBV) related hepatocellular carcinoma (HCC) remain unclear.
Aim: We investigated perioperative alterations of peripheral Bregs in HBV related HCC patients to reveal the relationship between Bregs and its clinical implications.
Methods: We have studied 23 patients with HBV related HCC and 14 controls, including patients with chronic HBV infection (CHB) and healthy donors. Frequency of peripheral IL-10+ CD19+ Bregs was measured by flow cytometry before, and after surgery. Clinical informatics of HCC patients was then collected using Digital Evaluation Score System for assessing disease severity. Finally, correlations between digitalized clinical features and kinetics of circulating Bregs were analyzed.
Results: Frequency of Bregs in CHB patients was higher than healthy donors. Preoperative level of Bregs in HCC patients was significantly lower than both control groups, but increased right after surgery (P<0.05). It was even higher than CHB patients about 7 days after surgery (P<0.05). Frequency of circulating Bregs was correlated with HBV related features including HBeAg and HBV DNA copy number.
Conclusions: Bregs were associated with active HBV infection, frequencies of peripheral Bregs in HBV related HCC patients increased after surgery. These results suggest that Bregs may play a role in the generation of HCC in patients with HBV infection opening a novel pathway to study immunopathogenesis of HBV related HCC.
Frequencies of peripheral regulatory B cells of different study groups.
Frequencies of peripheral regulatory B cells were analyzed in the healthy donors(Healthy), patients with chronic HBV infection (CHB), and patients with HBV related hepatocellular carcinoma (HCC) before surgery (HCCb), 1-2 days (HCCa1) or about 7 days (HCCa7) after surgery. Frequency of IL 10+CD19+ cells of total CD19+ B cells in the peripheral blood (B). The mean±SEM is shown,* and** stand for P<0.05 and 0.01, respectively.
Albert Schweitzer Ziekenhuis
ANTIBIOTICS RELATED ADVERSE DRUG EVENTS IN SURGICAL PATIENTS
Background: Medication related problems are a considerable cause of morbidity and mortality in hospitalized surgical patients. In contrast with other hospitalized patients, such as general medical patients, patients undergoing a surgical procedure are exposed to multiple medication changes associated with the surgical intervention. One of these medications is antibiotics, a great proportion of adverse drug events (ADEs) in hospitalized are attributed to these drugs. Another problem in prescribing antibiotics is intolerance or allergies for the drug.
Aim: The aim of this study is to determine the proportion of ADEs attributable to antibiotics and the incidence of allergies for antibiotics in surgical patients.
Methods: A multicentre study was performed in seven surgical units in three different hospitals: One university hospital and two teaching hospitals. Elective surgical patients with a hospital stay longer than 48 hours were included, ADEs were determined using chart review and an expert panel.
Results: During the study period, 567 patients were included, 49% male, mean age 62 years. Medication allergies were described in 87 of 545 patients (18.6%); in 51 patients (9.4%) there was an allergy for antibiotics, most frequently for penicillin. We found 156 ADEs in 130 of the 567 patients. Antibiotics were attributable to 4 (2.6%) of these ADEs, one ADE was preventable: a rash caused by ciproxin in a patient with a known allergy.
Conclusions: In surgical patients, antibiotics account for only a small proportion of ADEs; nevertheless caution and a good alert system is needed in patients with a known allergy for antibiotics.
Academical Medical Center, Amsterdam, Department of Surgery
St. Antonius Hospital
Department of Gastroenterology and Hepatology, Netherlands
SYSTEMATIC REVIEW AND META-ANALYSIS OF SOMATOSTATIN ANALOG FOR THE TREATMENT OF PANCREATIC FISTULA
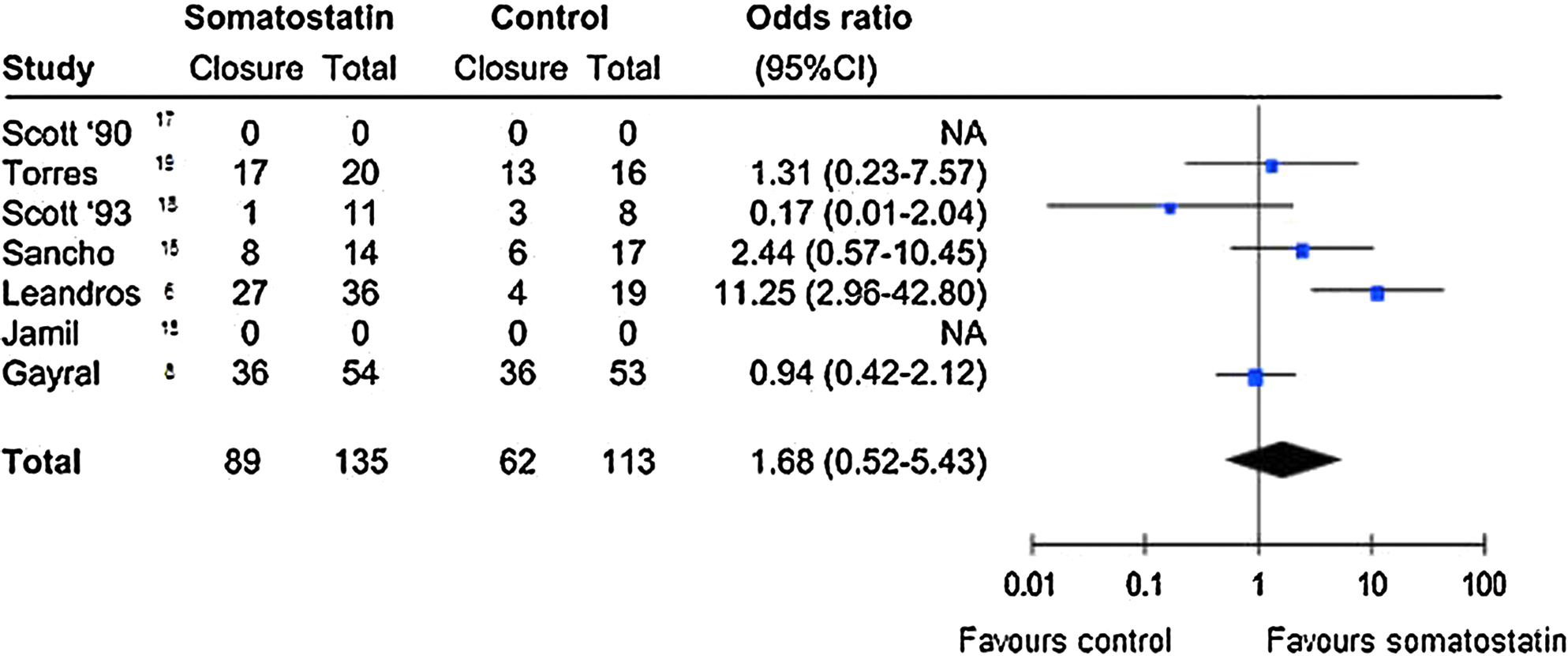
Background: Somatostatin analog are used for the treatment of pancreatic fistula designed to achieve fistula closure or reduction of output.
Aim: Trials comparing the effect of current standard management with standard management including somatostatin analog were identified to evaluate the effect of somatostatin on closure rate and time to pancreatic fistula closure.
Methods: PubMed, EMBASE, and Cochrane databases were systematically searched for relevant articles followed by hand searching of reference lists. Data on patient recruitment, intervention, and outcome were extracted and meta-analysis performed where reasonable.
Results: Seven randomized controlled trials met the inclusion criteria and included a total of 297 patients with fistulas of the gastrointestinal tract; of these, 102 patients had fistulas of pancreatic origin. Pooling of results for closure rate showed no significant difference between patients treated with somatostatin analog compared with controls, OR 1.68 (0.52–5.43). Due to inconsistent descriptions, pooling of results was not possible for other endpoints, such as time to closure.
Conclusions: There is no solid evidence that somatostatin analog result in a higher closure rate of pancreatic fistula compared with other treatments.
BakaSTsoumaILogothetisEYiallourouAGiokasGVorosDKouskouniE
Department of Biopathology and 2nd Department of Surgery, Aretaieion Hospital, University of Athens, Athens, Greece
BLOODSTREAM INFECTIONS IN THE INTENSIVE CARE UNIT: PATHOGENS AND ANTIMICROBIAL RESISTANCE
Background: Bloodstream infections occur more often in patients hospitalized in intensive care units (ICU) rather than in other settings within the hospital.
Aim: The prevalence of different pathogens isolated from positive blood cultures and their antimicrobial resistance.
Methods: All the bloodstream infections reported during January 2008 to October 2010 were included in the study. After incubation in a blood culture system (BACTEC 9050, Becton Dickinson, USA), positive blood-cultures were cultured in standard aerobic and anaerobic conditions and incubated at 37°C for 24h and 48h, respectively. The isolated pathogens were identified using the automated system VITEK 2 (BioMerieux, Marcy l'Etoile, France) which was also used to test the susceptibility of the isolates to different antimicrobial agents.
Results: One hundred and seventy-six positive blood cultures from 95 different ICU patients were included in the study. Out of the 176 positive blood-cultures we isolated 1 microorganism in 149 (84.7%) cases, 2 microorganisms in 25 (14.2%) and from the remaining 2 (1.1%) positive blood cultures, 3 microorganisms were isolated. In total, 231 pathogens were isolated: 107 (46.3%) staphylococci, 91 (39.4%) Gram-negative rods, 25 (10.8%) enterococci and 8 (3.5%), Candida species. All staphylococci were susceptible to vancomycin, teicoplanin and linezolid. 36% of the Enterococcus faecium strains were resistant to vancomycin, while all the E. faecalis strains were susceptible. Finally, the Gram-negative rods were characterized by increased level of resistance against most of the antimicrobials tested.
Conclusions: Staphylococci were most frequently isolated from the positive blood cultures studied.
EfstathiouP
Microbiology Laboratory of Aretaieio Hospital, Athens University School of Medicine, Greece
IMPLEMENTATION OF ANTIMICROBIAL COPPER AT EDUCATIONAL FOUNDATION PREMISES AS MEANS OF PUBLIC HEALTH PROTECTION
Background:
Aim: The aim of this report is the application of antimicrobial copper alloys in multi – touch surfaces at educational institutions (mass gathering areas) for the reduction of microbial flora in order to protect public health.
Methods: We used antimicrobial copper alloys (Cu 63%–Zn 37%) to cover or replace multi - touch surfaces (door handles, railings, hand-push surfaces, etc.) in a specific elementary school. Estimation of microbial flora and viral load carried out in two phases. Prior and after antimicrobial copper implementation. Samples were taken from surfaces, cultured in appropriate-selective culture media for microbial growth and molecular techniques for isolating viruses.
Results: Results showed clear reduction in the amount of microbial loads in all surfaces and objects replaced by antimicrobial copper. The number of bacteria isolated in the respective surfaces before the copper implementation was a multiple of bacteria isolated after copper implementation. The correlation resulted in the findings of a reduction in the number of bacteria colonies (CFU / ml) after antimicrobial copper implementation.
Conclusions: Researchers have shown great interest in antimicrobial copper because usage of both antimicrobial copper and its alloys for the protection of public health gives encouraging results. Usage of the antimicrobial properties of copper in multi-touch surfaces of mass population concentrations, such as in schools, has already started to apply worldwide. Limiting the spread of germs and viruses in those areas in combination with the implementation of the basic methods of infection preventing (clean hands, etc.) is a strong antimicrobial ally to public health.
HedmanDThomassonJTingstedtBAnsariDWilliamssonCAnderssonBAnderssonR
Lund University, Sweden
IMPACT OF CENTRALIZATION ON PERIOPERATIVE OUTCOMES AFTER PANCREATICODUODENECTOMY
Background: In Sweden, high-risk oncological surgery such as pancreaticoduodenectomy has been centralized following the volume–outcome relationship reported in the literature.
Aim: The objective of the present study was to report the perioperative results of performing pancreaticoduodenectomy at a center specialized in hepatopancreaticobiliary surgery, also investigating the transition of this institution from a low volume to a high volume center by comparing operative and complication parameters.
Methods: A retrospective review was conducted of 175 consecutive patients undergoing pancreaticoduodenectomy at the Department of Surgery, Skane University Hospital, Lund, between 2000 and 2011. Complications were graded according to the Clavien-Dindo Classification.
Results: Major postoperative complications (Clavien-Dindo III or above) were found in 25% of cases (44 patients). Median length of stay was 17 days. Comparing the low volume and high volume periods, median operation time decreased from 555 min to 450 min (p<0.0001) and median blood loss dropped from 1000 ml to 475 ml (p<0.0001). Rate of delayed gastric emptying (DGE), surgical infections and postoperative bleeding decreased significantly, although no significant decrease in the rate of overall complications could be seen. Postoperative mortality was 1% (2 patients), both deaths occurring in the low volume group.
Conclusions: Even though no significant decrease in overall complications could be found, operative time, blood loss, DGE, surgical infections and postoperative bleeding favorably decreased during the high volume period.
AnsariD1GianottiL2SchröderJ3AnderssonR1
Lund University, Sweden
Milano-Bicocca University, Italy
Marien-Krankenhaus Bergisch Gladbach, Germany
FAST-TRACK SURGERY: WHAT IS THE PROCEDURE-SPECIFIC EVIDENCE?
Background: Fast-track (FT) surgery can be defined as a coordinated perioperative approach aimed at reducing surgical stress and facilitating early recovery.
Aim: To review the literature on the procedure-specific application of FT surgery.
Methods: PubMed was searched for randomized controlled trials (RCTs), quasi-RCTs, cohort studies, case-control studies and case series. The following key words were used: fast-track, enhanced recovery, accelerated rehabilitation and multimodal optimization. Trials documenting a minimum of 4 FT components were selected. Non-English language articles were excluded. One of the authors reviewed and abstracted the following data: first author, year of publication, study population, study design, length of stay, and major findings.
Results: Most studies (n=132) investigated the effects of FT in colorectal surgery. The remainder dealt with orthopedic surgery (n=42), hepatopancreaticobiliary surgery (n=17), urological surgery (n=17), upper gastrointestinal surgery (n=15), gynecological surgery (n=14), vascular surgery (n=10), thoracic surgery (n=8), endocrine surgery (n=5), breast surgery (n=4), pediatric surgery (n=3) and hernia repair (n=2). Overall quality of included studies was moderate, and there was considerable heterogeneity in the number of included FT elements. However, FT surgery was safe and feasible and demonstrated a clear benefit through the different procedures/specialties where the concept has been implemented.
Conclusions: The principles of FT surgery can be applied in most organ-specific procedures. Standardized protocols should be provided on a procedure-specific basis.
Oral Poster Presentations
YoshidaY
Ichinomiya Hot Spring Hospital, Japan
ANNUAL REPORT ON THE JAPAN SOCIETY FOR SURGICAL INFECTION 2011-2012
Background: JSSI is a core scientific organization in the Asia-Pacific region.
Aim: To promote the mutual understanding and friendship with SISs.
Methods: JSSI is dedicated to providing its members and the scientific community, as events, publications, investigation, and research around the surgical infections, relations, and others.
24th Annual Meeting in 2011 / President: Professor Kusunoki
25th Annual Meeting in 2012 / President: Professor Oda (Chiba on November 21–22)
(Publications)
Bi-monthly official journals and original articles
(Investigation and Research)
Prospective Clinical Trials Committee had requests from the company
RCT Committee done RCTs on antimicrobial prophylaxis and intravenous immunoglobulin
(Relations)
2011 Invitation Lecture of the President of SIS-E
First Asian Symposium
Appealed for holding joint session of SIS-E, SIS-NA, and JSSI in the next SIS combined meeting
2012 Invitation Lecture of the President of SIS-NA,
Second Asian Symposium.
(Others)
The Certification Committee authorized 94 surgeons to take charge of education provisionally until it raises the medical specialist of surgical infection, and authorizes 44 institutions as educational facilities. The Educational Committee created the educational programs, with four boards classified by color, and held the workshop using this. The Guideline Committee and Quality and Safety Committee carried out unique works. A standing committee (Conflict of Interest Committee) and a provisional committee (Election Administration Committee) increased in 2011.
Conclusions: JSSI is one society that lead the world, which contributes quality and safely of perioperative medical treatment, and achieves social responsibility.
Toribio-GarcíaJCordero ComaMRodríguez DomingoE
University Hospital of León, Ophthalmlogy Service, Spain
POST-CATARACT SURGERY ENDOPHTHALMITIS BY PSEUDOMONAS AERUGINOSA
Background: Intraocular infections after cataract surgery have remarkably decreased due to intracameral cefuroxime injection at the end of the surgery. This antibiotic is currently very popular all over Europe since it has demonstrated a 75% decrease of post-cataract surgery endophthalmitis rate. However, intraocular infections are still developed in some cases.
Methods: An 84-year-old male patient underwent cataract surgery in his right eye by emulsification. His visual acuity before surgery was 20/200. There were no complications at the surgery. At the end of the surgery, 1 mg of cefuroxime in 0.1 ml of balance saline solution was put in the anterior chamber. Nine days after surgey, the patient complained of visual loss and pain in the operated eye. Visual acuity of his right eye was hand movement and there was 1 mm of hypopyon and profuse fibrin exudate in the anterior chamber. A sample of aqueous humour was taken and sent to the microbiology deparment. He was admitted and topical and endovenous treatment with vancomycin and ceftazidime was initiated. The following day, the hypopyon had disappeared but the fibrin exudate still remained. The microbiologic study revealed growth of Pseudomonas areuginosa. Three weeks later, the patient had a visual acuity of 20/60 and a transparent cornea without fibrin remains.
Results:
Conclusions: Systematic use of cefuroxime is changing the spectrum of involved bacterias, from gram positive cocci to gram negative bacilli, like Pseudomonas. We must take into account that prompt and aggressive treatment with broad spectrum antibiotics is mandatory in such patients.
San MiguelB1MarcolinE2TieppoJ2CulebrasJ3MarroniN2TuñónM1González-GallegoJ1
Institute of Biomedicine (IBIOMED) and CIBERehd, University of León, Spain
Laboratorio de Hepatologia Experimental Fisiologia HCPA/UFRGS, Porto Alegre, Brazil
Hospital of León, Spain
QUERCETIN ATTENUATES METHIONINE AND CHOLINE-DEFICIENT DIET-INDUCED STEATOHEPATITIS IN C57BL/6 MICE
Background: Nonalcoholic steatohepatitis (NASH) is a metabolic condition characterized by lipid accumulation in hepatocytes, inflammatory infiltration and fibrosis. Flavonoids have demonstrated a high therapeutic potential in various pathologies and a protective role in inflammatory processes. Quercetin is the major flavonoid found in the human diet.
Aim: This study aims to elucidate the effects of quercetin on inflammatory status and expression of pro-fibrogenic factors in a nutritional model of NASH.
Methods: Feeding a methionine-choline-deficient (MCD) diet to rodents reproducibly elicits NASH with fibrosis mimicking the severe form of NASH that occurs in some humans. We used C57BL/6 males divided into four experimental groups (n=12): control, NASH, quercetin-treated control, and quercetin-treated NASH mice. Quercetin (50 mg/kg) was administered intragastrically for 4 weeks.
Results: Quercetin significantly reduced gross damage and histopatological scores in the liver of treated NASH mice. Animals in the NASH group showed a marked increase of mRNA levels of tumour necrosis factor-alpha (TNF-alpha), interleukin-6 (IL-6), transforming growth factor-beta (TGF-beta), Smad3, and alpha-smooth muscle actin (alpha-SMA). Expression of these inflammatory and fibrogenic markers were inhibited by administration of quercetin.
Conclusions: In summary, this study indicates that quercetin treatment prevents inflammation and fibrosis in a rodent model of NASH. This result supports that trials of quercetin may be reasonable in patients with established liver disease and inflammation.
Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBERehd) and Institute of Biomedicine (IBIOMED), University of León, Spain
Institute of Biomedicine (IBIOMED), University of León, Spain
Laboratory of Experimental Hepatology and Physiology, Porto Alegre Clinical Hospital, Federal University of Rio Grande do Sul, Porto Alegre, Brazil and Institute of Biomedicine (IBIOMED), University of León, Spain
Universitary Hospital of León and Institute of Biomedicine (IBIOMED), University of León, Spain
GLUTAMINE TREATMENT ATTENUATES ENDOPLASMIC RETICULUM AND APOPTOSIS STRESS IN TNBS-INDUCED COLITIS
Background: Inflammatory bowel diseases result from complex interactions among many factors, including overproduction of proinflammatory cytokines and reactive oxygen mediators, induced endoplasmic reticulum (ER) stress response, and apoptosis.
Aim: To investigate the ability of glutamine to reduce ER stress and apoptosis in a model of experimental colitis.
Methods: Colitis was induced in male Wistar rats by intracolonic administration of 30 mg of 2,4,6- trinitrobenzene-sulfonic-acid (TNBS). Glutamine (25mg/dL) was given by rectal route daily for 2 or 7 d. Rats were killed at 2 or 7 d and the distal 8 cm of the colon was collected.
Results: Both oxidative (TBARS concentration and oxidized/reduced glutathione ratio) and ER stress markers (CHOP, BiP, calpain 1 and caspase-12 expression) increased significantly within 48 h of TNBS instillation, and glutamine attenuated the extent of the changes. Colonic phospho-JNK and PARP-1 expression was also significantly higher in TNBS-treated rats compared to the control group, and treatment with glutamine significantly decreased JNK phosphorylation and PARP-1 proteolysis. TNBS instillation resulted in a significant increase in p53 and cytochrome c expression, and a reduced Bcl-xL expression and Bax/Bcl-2 ratio. These effects were significantly inhibited by glutamine. Treatment with glutamine also resulted in significant decreases of caspase-9, caspase-8, and caspase-3.
Conclusions: In addition to the antioxidant and anti-inflammatory properties of glutamine, data indicated that protection against damage in TNBS-induced colitis might be partly mediated by early inhibition of the ER stress response and anti-apoptotic effects.
EnholmB1RabahS2PirkkaV3MaaretK2MarcB2AriL1
Department of Abdominal Surgery, Helsinki University Central Hospital
Protein Chemistry Unit, Biomedicum Helsinki
Department of Vascular Surgery, Helsinki University Central Hospital, Finland
A COMPARISON OF THE PLASMA PROTEOME OF PATIENTS WITH APPENDICITIS, MESENTERIAL ISCHEMIA, AND SECONDARY PERITONITIS
Background: The acute abdomen is a diagnostic challenge and acute mesenterial ischemia is particularly dependent on an expedient diagnosis for optimal treatment.
Aim: Samples from patients with confirmed appendicitis, secondary peritonitis, or mesenterial ischemia were analyzed by LC MS/MS and the resultant plasma proteome profiles were compared for identification of peritonitis and ischemia-specific molecular determinants.
Methods: Plasma samples were subjected to depletion of albumin, IgG, antitrypsin, IgA, transferrin, haptoglobin, and fibrinogen, trypsin-digested and analyzed by LC MS/MS consisting of nano-Acquity UPLC coupled to a Synapt G2 HDMS mass spectrometer (Waters, UK). ProteinLynxGlobalServer (PLGS) version 2.4v software was used for the processing of raw data and protein database searching. Results were interpreted in terms of PLGS Mowse score protein readouts for peptide hits.
Results: To date, 10 patients have been analyzed: Six with appendicitis, three with peritonitis, and one with mesenterial ischemia. All patient groups had higher levels of C-reactive protein (CRP) and serum amyloid A (SAA) as compared to controls. Peptides detected specifically in peritonitis samples included Light chain of factor I (495.94 vs. 0 mean scores) and leucine-rich alpha 2 glycoprotein (595.45 vs. 108.06 mean scores). In contrast, the mesenterial ischemia sample displayed a divergent proteome that included elevated levels of complement component 4 binding protein (760.21 vs. 0 mean score) and low levels of Apo-E (300.11 vs. 22,539.8 mean score).
Conclusions: High-throughput profiling of the plasmaproteome in patients with an acute abdomen displays diverging proteomic profiles for different etiologies.
Centro de Investigación Biomédica en Red de Enfermedades Hepáticas y Digestivas (CIBERehd) and Institute of Biomedicine, University of León
Department of Surgery II, Complejo Asistencial Universitario de León, Hospital of León
Department of Oncology, Complejo Asistencial Universitario de León, Hospital of León, Spain
PPI-2458 ADMINISTRATION ON HEPG2 HEPATOCARCINOMA CELLS: INDUCTION OF STAT3 AND INFLUENCE ON CYTOKINES AND CELL CYCLE
Background: PPI-2458, a fumagillin derivative, has been tested in different tumor cells types. In HepG2 liver cancer cells this drug has demonstrated its efficacy reducing cell viability, inducing cycle progression and apoptosis.
Aim: We have investigated the effect of PPI-2458 on STAT3 pathway, its relation with cell cycle control and cytokine release on HepG2 hepatocarcinoma cells.
Methods: HepG2 cells were treated with PPI-2458 at the concentration of 10 nM at different times (2-6 days). Cell viability was determined by MTT assay. Moreover, expression of the different markers was analyzed by Western blot and RT-qPCR.
Results: Treatment with PPI-2458 resulted in a marked decrease of cell viability reaching a maximum in cells treated for 6 days. The inhibition on cell viability was accompanied by an increase in phospho-STAT3 in association with upregulation of cyclin D1 and P21 protein levels. Inhibition of STAT3 resulted in a marked decrease of cyclin D1 and P21. Furthermore, PPI-2458 induced the expression of inflammatory cytokines such as TNFα, IL-1β and VEGF. STAT3 inhibition did not modify TNF-α mRNA levels. However, IL-1β mRNA levels were augmented, whereas VEGF levels were decreased by STAT3 inhibition
Conclusions: PPI-2458 is able to induce an increase on phospho STAT3 protein levels, which could, at least in part, drive the expression of P21 and cyclin D1. In our experiments, STAT3 seems to be able to regulate VEGF and IL-1β transcription, but further investigations are necessary to elucidate the precise mechanism involved.
Centro de Investigación Biomédica en Red: Enfermedades Hepáticas y Digestivas (CIBERehd), and Institute of Biomedicine, University of León
Department of Surgery II, Complejo Asistencial Universitario de León, Hospital of León, Spain
I Department of Internal Medicine, University Medical Center, Johannes-Gutenberg-University, Mainz, Germany
MELATONIN INDUCES APOPTOSIS IN HEPG2 HEPATOCARCINOMA CELLS THROUGH TRANSCRIPTIONAL REGULATION OF BIM BY FOXO3A
Background: Hepatocellular carcinoma (HCC) is diagnosed in more than half a million people worldwide per year. Aggressive surgery or liver transplant are the only successful treatments available. Advances in understanding proliferation and apoptosis processes are needed to develop effective therapies. We have previously demonstrated that melatonin administration induces cycle arrest and apoptosis in HCC, but the precise pathways involved remain unclear. FoxO transcription factors play an important role in tumor suppression up-regulating target genes such as the pro-apoptotic protein Bim.
Aim: In line with these findings, we focused our study on the FoxO3a regulation of Bim after melatonin treatment.
Methods: HepG2 HCC cells were treated with 1000 and 2000 μM melatonin concentration. Expression of pro-apoptotic gene Bim was analyzed by qRT-PCR and Western Blot. FoxO3a activation was determined by luciferase reporter gene assay in transfected HepG2 cells, and its phosphorylation status by Western Blot. Nuclear translocation of FoxO3a was visualized by immunofluorescence.
Results: Both doses resulted in a significant induction of Bim at mRNA and protein levels, and increased FoxO3a transcriptional activity. Furthermore, melatonin was able to decrease the phosphorylated forms of FoxO3a at Thr32 and Ser253, increasing total FoxO3a. Dephosphorylation at these specific sites has been associated with changes on the FoxO3a subcellular location, to promote its transcriptional activity.
Conclusions: Together these data confirm that Bim plays a significant role in melatonin-induced apoptosis, most likely thought FoxO3a is a transcription factor in HepG2 cells, suggesting its safe use in HCC treatment, at least as a coadyuvant.
Institute of Biomedicine (IBIOMED) and CIBERehd. University of León
Department of Animal Health, University of León
Hospital of León, Spain
PROTECTIVE EFFECT OF MELATONIN IN AN ANIMAL MODEL OF VIRALLY INDUCED FULMINANT HEPATIC FAILURE
Background: Impaired liver regeneration is one of the most critical issues in the prognosis of fulminant hepatic failure (FHF).
Aim: To investigate the effect of melatonin on inflammatory and regenerative response in an animal model of FHF of viral origin.
Methods: Rabbits were experimentally infected with 20,000 hemagglutination units of a rabbit hemorrhagic disease virus (RHDV) isolate and received melatonin (10 and 20 mg/kg) at 0, 12, and 24 h postinfection.
Results: RHDV infection induced an inflammatory response in the liver, with increased expression of reactive C protein (CRP), interleukin (IL)-1beta, IL-6, and tumour necrosis factor (TNF). These effects were attenuated by melatonin in a concentration-dependent manner. In addition, melatonin treatment also resulted in a reduced expression of toll-like receptor (TLR)4 and matrix metalloproteinase (MMP)9. RHDV infection induced an inhibition of the hepatic regenerative/proliferative response, with a reduced expression of hepatocyte growth factor (HGF), epidermal growth factor (EGF), platelet-derived growth factor (PDGF)B, and vascular endothelial growth factor (VEGF) that were prevented by melatonin administration. Pro-regenerative effects of melatonin were related to a reduced expression of phosphorylated Janus kinase (JNK) expression and enhanced expressions of extracellular mitogen-activated protein kinase (ERK) and signal transducer and activator of transcription (STAT)3.
Conclusions: Our findings show that anti-inflammatory effects and stimulation of regenerative mechanisms contribute to the beneficial effects of melatonin in rabbits with experimental infection by RHDV, and support a potential hepatoprotective role of melatonin in FHF.
PejcicVJovanovicSDjordjevicMPavlovicAJovanovicBMiticN
Clinical Center, Nis Serbia
WOUND INFECTION TREATMENT AFTER THE OPERATION OF POSTOPERATIVE HERNIA WITH HYDROCOLLOID DRESSINGS—OUR FIVE YEARS' EXPERIENCE
Background:
Aim: Our aim was to treat most frequent complications after operation of large ventral hernias such as seromas and wound infextions.
Methods: In treatment of wound infection we used hydrocolloid dressings AQUACEL (Convatec, UK). Aquacel Ag dressings make use of ionic silver compound distributed within the dressing itselfe. Aquacel Ag prevents drying of the wound, it is easy to remove and does not induce bacterial resistance. Aquacel Ag in each dressing ensures a continuous release of silver for up to seven days (recommendation of the producer).
During the period April 4, 2005 to December 31, 2010 in the Center for Minimally Invasive Surgery Nis were performed in 682 operations of primal ventral and incisional hernias. There were 29 mesh infections. Prospectively, we analyzed 29 patients (ASA I-III) with mesh infection. We analyzed choice of anesthesia, operating time, postoperative complications, the need for antibiotics, hospitalization time, and time before returning to work.
Results: Median age was 59 (21-70). They were 10 male and 19 female patients. Patients were operated in local(12) and general anesthesia(17). The average operating time was 90 minutes (40-120 minutes). We made 12 patients with classical treatment and 17 patients with hydrocolloid dressings AQUACEL (Convatec, UK). Recovery time in the first group was an average of 34 days and in second group was 17 days. In all cases, the wound was opened and bandaged.
Conclusions: The percent of patients who would be underwent to MESH extraction because of the wound infection was minimized by using hydrocolloid dressings.
ChenY1ChenI2ChenC2WangF3
Department of Infection Control, Taipei Veterans General Hospital, Department of Nursing, Taipei Veterans General Hospital, Taipei
Taipei City Hospital, Branch for Women and Children, Taipei
Division of Infectious Diseases, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
ANTIBIOTIC-RESISTANT ORGANISMS AND ATTRIBUTABLE MORTALITY OF SURGICAL SITE INFECTION
Background: Surgical site infections (SSIs) are a real risk associated with any surgical procedure and its impact on morbidity and mortality, particularly in patients with antimicrobial-resistant pathogen SSIs.
Aim: The aim of this study was to identify the association between nosocomial SSIs and attributable mortality.
Methods: A retrospective cohort study was conducted in a 2,900-bed tertiary refer medical center in Taiwan. All patients who received a surgical procedure that had developed SSIs from 2009 to 2010 were eligible. The definitions of the Centers for Disease Control and Prevention were used to categorize superficial incision site, deep incision space, or organ space.
Results: Seven hundred and sixty-nine patients with a SSI were identified. The incidence rate was 8.1%. The frequent sites were superficial incision site (45%), organ space (32%), and deep incision space (23%). The most common organisms were Staphylococcus aureus (11.6%), Pseudomonas aeruginosa (7.1%), and Enterococcus spp. (6.4%). The most common antibiotic-resistant organisms were Klebsiella pneumonia and Escherichia coli producing extended spectrum beta-lactamase (ESBL) 3.1%. After controlling prognostic factors for mortality, ESBL (odds ratio [OR] 3.45; 95% confidence interval [CI] 1.32, 9.04), length of stay before onset of SSI (OR 1.009; CI 1.003, 1.015), and age (OR 1.027; CI 1.010, 1.044) were independent factors.
Conclusions:S. aureus was the most common organisms of SSIs. K. pneumonia and E. coli ESBL SSIs were the important prognostic factors after adjusting for covariates. This emphasizes the importance of continuous efforts in the prevention of SSIs, especially antimicrobial resistance.
ChooklinSBihalskyyIHranatO
Medical University of Lviv, Ukraine
N-ACETYLCYSTEINE AND LOCAL PURULENT PROCESSES IN SEVERE ACUTE PANCREATITIS
Background: Severe acute pancreatitis (SAP) is associated with significant morbidity and mortality. The majority of deaths related to SAP are the result of infectious complications. In patients with acute necrotizing pancreatitis after percutaneous drainage or necrectomy there are often lengthy selection drains, mainly because of the increased viscosity of secretions.
Aim: The aim of the study was the effect of N-acetylcysteine on the course of purulent process in acute pancreatitis.
Methods: We used N-acetylcysteine locally in six patients with acute pancreatitis.
Results: In five patients after necrectomy and one after the percutaneous drainage, catheter-type "pig-tail" remained fluid accumulation, maintained septic episodes (continued rises in body temperature for seven days). The number of discharges was 50–70 ml. These patients began to enter through drains to 1200-1800 mg N-acetylcysteine in the day. After 6.7 days marked increase in emissions to 270-300 ml, normalization of body temperature. Gradually, a 2-3 week, the number decreased to the 50 ml. Further outpatient treatment allowed the recovery of patients after an average of two months.
Conclusions: To improve the drainage function of postoperative interventions to reduce the viscosity of secretions appropriate to the local input of N-acetylcysteine.
MózesT1GornicsarK2GroszA3DomjánZ2BuzogányI2
Ministry of Defense Health Centre
Department of Urology, Péterfy Hospital
Department of Aerospace Medicine, University of Szeged, Hungary
CAN WE PREDICT POST-OPERATIVE INFECTIONS?
Background: Many patients develop infections following operations. Decreased immune competence has been demonstrated in acute neurological conditions.
Aim: A strong cytokine mediated anti-inflammatory response was observed in stroke patients at infection, although infection due to the decreased pro-inflammatory mediators can be expected as well. To investigate this question the following experiment was performed.
Methods: Ten urinary bladder cancer patients with radical cystectomy and lymphadenectomy were studied. Blood samples were taken on Day 0 before and Day 1, 3, 6, 9, and 14 after operation as well as on Day 30, 60, 90, and 270 during follow up.
TNF, soluble TNF receptor I, and IL-6 levels in sera were determined by HS ELISA and/or ELISA. Plasma ACTH and cortisol values were measured by RIA kits.
Results: From 10 urinary bladder cancer patients five deep wound and urine infections were found in 14 days and three urine infections in 30 days after surgery, all survived. All patients were bacterially contaminated. On Day 0 the circulating TNF values were lower in infected patients. TNF started to increase from Day 3 till Day 9, never reaching values of uneventful healing group. Soluble TNF receptor I, IL-6, ACTH, and cortisol concentrations did not demonstrate any difference on Day 0, however, from Day 1 started to increase transiently, reaching higher levels in septic patients.
Conclusions: An excessive decrease in pro-inflammatory response is a key facilitating factor for the development of infection. Thus, measuring serum TNF levels before and after operations can predict the outcome.
SURGICAL MANAGEMENT OF ACUTE CHOLECYSTITIS IN A LOW-VOLUME HOSPITAL
Background: Laparoscopic cholecystectomy(LC) has become the preferred approach for most patients with acute cholecystitis.
Aim: To present our outcomes changing our surgical approach from OC to LC in acute clolecystitis management.
Methods: Preoperative and intraoperative data were collected from 597 patients (53% female, 47% male),mean age 61 years who underwent cholecystectomy in 10 years time (2002–2011). The patients divided into two groups: Group A (2002-2006): 217 patients, Group B (2007-2011): 380 patients. 278 patients were operated on for acute calculous cholecystitis, 98 Group A and 180 Group B. The diagnosis was based on clinical, laboratory, and U/S findings. The decision for LC was based on less than 5 mm thickness of the gallbladder wall, C reactive protein level below 10 mg%, and the time passed from the onset of the symptoms (<72 h).
Results: 23 (23%) patients from Group A underwent LC, 75 (77%) patients, OC. 108 (60%) patients from Group B, LC; 72 (40%) patients, OC. There were no deaths,no iatrogenic common bile duct injuries, and no residual common bile duct stone. 5 (21%) patients from Group A and 18 (16%) from Group B underwent conversion. 3 patients from Group A and 2 from Group B developed bile leaks postoperatively and they repaired by our team. Postoperative hospitalization ranged between 48-72 h.
Conclusions: LC for acute cholecystitis is performed with increasing frequency in our unit. Acute clolecystitis can be managed safely via laparoscopic approach in selected cases and in low volume surgical units.
MarakutsaE
Transnistrian State University, Moldavia
FOURNIER'S GANGRENE: EXPERIENCE OF SEVEN CASES
Background: Fournier's gangrene (FG) is a specific form of necrotizing fasciitis with a high mortality rate.
Aim: To describe patients diagnosed with FG between 2006 and 2011.
Methods: All patients with FG who were treated between 2006 and 2011 were retrospectively analyzed for history, clinical presentation, laboratory parameters, intraoperative findings, and postoperative course. Standardized approach included immediate and radical debridement, intensive care and antibiotic treatment. Following programmed daily revisions, wound closure was achieved by reconstructive surgery. Statistical analysis was performed by using MedCalc v. 12.
Results: 7 patients were treated, 1 female and 6 males with a median age of 63 years. Many of them had predisposing diseases. The etiology was colorectal in five patients, genitourinary in 1 and idiopathic in 1. The symptoms were scrotal and perineal pain, perianal and scrotal erythema, necrosis and purulent discharge. Treatment included hemodynamic support, broad-spectrum antibiotic therapy and surgical debridement. Colostomy was performed in 2 patients, urinary diversion in 1 due to urethral destruction, and orchiectomy in 1 due to testicle abscess. Microbiological cultures isolated mainly E. coli, Bacteroides, Enterococcus faecalis, and multiresistant strains of Klebsiella pneumoniae. 5 patients survived (71%) and 2 died (29%), with an average hospital stay of 38 days. Preexisting malignancy and higher percentage of affected body surface area was associated with an increased mortality.
Conclusions: FG is a rare disease with a high mortality rate. Treatment usually consists of the surgical debridement of necrotic tissue and the administration of broad-spectrum intravenous antibiotics.
Department of General Surgery, La Princesa University Hospital, Madrid
Department of Clinical Microbiology, La Princesa University Hospital, Madrid, Spain
DIVERTICULAR DISEASE COMPLICATED BY FISTULAE: WHAT CAN WE LEARN FROM THESE PATIENTS?
Background: The incidence of fistulae in patients with diverticular disease, the most common cause of colovesical fistula, is accepted to be around 2%. Symptoms include suprapubic pain, dysuria, and frequency and chronic urinary tract infections (UTI), usually treated with various courses of antibiotics. Fecaluria can be considered pathognomonic.
Aim: To present our experience in the management of vesicoenteric fistulae secondary to diverticular disease.
Methods: Descriptive, retrospective study of patients with vesicoenteric fistulae in our institution in the last 5 years. Evaluation of the clinical presentation, diagnosis and treatment.
Results: Six patients presented colovesical fistulae, and one a rectovesical fistula. Male–female ratio was 3:4. Mean age: 71 years. Patients' data are shown in the table 1 below. All patients underwent elective open surgery. The standard procedure for colovesical fistulae was a sigmoidectomy and T-T colorectal anastomosis. Four patients needed primary repair of the bladder. A rectal stump resection, extended right hemicolectomy and ileo-colic anastomosis was performed on the patient with the rectovesical fistula.
Patient
Presentation (symptoms)
Duration of symptoms
Chronic UTI?
Previous antibiotics?
Diagnosis
Positive urinary culture?
Isolated bacteria
1
Pain, dysuria, tenesmus
1 month
No
Yes
CT and colonoscopy
Yes
E.coli ESBL
2
Constipation, pain, dysuria
2 months
Yes
Yes
CT and colonoscopy
No
-
3
Pain, rectal bleeding
1 week
Yes
Yes
CT and colonoscopy
Yes
Mixed flora
4
Pain, fecaluria, pneumaturia
6 months
Yes
?
CT
Yes
E.coli
5
Anal discharge
2 months
No
Yes
Colonoscopy
Yes
E.coli
6
Fecaluria, pneumaturia
2 years
Yes
Yes
CT
Yes
E.coli
7
Fecaluria, fever
5 months
Yes
Yes
CT
Yes
K.pneumoniae ESBL
Conclusions: A better knowledge of the characteristics and presentation of diverticular disease complicated by fistulae can help to improve our management of these patients. Surgical resection of the involved segment of colon and primary anastomosis is the treatment of choice.
Toribio-GarcíaJ1Casas RoderaP2Casas RubioC2
University Hospital of León, Ophthalmology Service
University Hospital of León. Otolaryngology Service, Spain
SUBPERIOSTEAL ORBITAL ABSCESS AFTER MAXILLARY AND ETHMOIDAL ANTRECTOMY FOR CHRONIC SINUSITIS
Background: Chronic sinusitis is usually associated with a small ostium of drainage. The maxillary antrectomy improves mucus evacuation and prevents infection. However, if surgical technique is not correct and the medial orbital wall is broken, it can produce a subperiosteal orbital abscess.
Aim: This surgical infection can threaten visual acuity and even the life of the patient.
Methods: A 32-year-old female patient with chronic sinusitis underwent antrectomy in an other clinical center by endoscopic sinus surgery in her right maxillary and ethmoidal sinus. The following three days, despite being treated with amoxicillin/clavulanic acid, she developed temperature, headache, proptosis, and visual acuity loss in her right eye so she was referred to our hospital. When she arrived at our hospital her visual acuity was no light perception in her right eye. Orbital computed tomography (CT) revealed a subperiosteal abscess in the medial orbital wall and apex. She was admitted and underwent an emergency medial anterior orbitotomy to drain the subperiosteal abscess. We initiated endovenous treatment with linezolid and meropenem.
Results: Culture of abscess fluid showed growth of methicillin-resistant Staphylococcus aureus. On following days, her general condition improved but she did not recover vision.
Conclusions: Paranasal sinuses surgery is a possible local infection source. The proximity of these cavities to the orbit allows the passage of microorganisms into the orbit. Choosing the most accurate antibiotic therapy and making a prompt orbital CT and drainage of abscess are the treatment of this infection with an important morbility.
Department of General Surgery, La Princesa University Hospital, Madrid
Department of Clinical Microbiology, La Princesa University Hospital, Madrid
Department of Preventive Medicine, La Princesa University Hospital, Madrid, Spain
SURGICAL INFECTION BY MULTI-RESISTANT PSEUDOMONAS AERUGINOSA AFTER EVENTROPLASTY: IS REMOVAL OF THE MESH MANDATORY?
Background: Infections by multidrug-resistant P. aeruginosa are increasingly being reported in the surgical setting. Management can be complicated, with almost no choice of antibiotics left for treatment.
Aim: To describe a case of soft tissue infection by P. aeruginosa involving mesh, the clinical management, and outcome.
Methods: A 62-year-old woman, with a history of diabetes, high blood pressure, chronic kidney disease, thrombotic CVA, arthritis, gout, and gastric bypass, presented with recurrent cholangitis. She had previously undergone cholecystectomy and choledochoduodenostomy. She now presented stenosis of the latter, residual choledocholithiasis, and a ventral hernia. An elective operation was performed: Laparotomy, extraction of residual calculi, hepaticojejunostomy, and eventroplasty. After surgery she presented acute renal failure, polyarthritis, and surgical wound infection. Cultures were positive for P. aeruginosa, only susceptible to Amikacin.
Results: Despite renal failure, intravenous treatment with Amikacin was started with a strict dose adjustment and blood-level controls. The presence of a mesh made the situation more challenging. Exhaustive cleansing and dressing of the wound, avoiding exposure of the mesh, was performed twice a day. Eventually, the infection was controlled, and the patient was discharged on the 47th postoperative day.
Conclusions: Management of patients with infections by multiresistant pathogens can be challenging for the surgeon: They can complicate the postoperative course and increase hospital stay and costs. An early diagnosis and targeted antibiotic therapy are essential, and can avoid mesh removal in some patients.
Department of General Surgery, La Princesa University Hospital, Madrid
Department of Clinical Microbiology, La Princesa University Hospital, Madrid, Spain
NECROTIZING FASCIITIS OF THE ABDOMINAL WALL: WHAT'S THE KEY TO A SUCCESSFUL TREATMENT?
Background: Necrotizing fasciitis is an uncommon but severe condition, which causes a rapid infection of the subcutaneous tissue and fascia, resulting in necrosis, sepsis, and death if not treated promptly and aggressively.
Aim: We present the case of a patient with necrotizing fasciitis of the abdominal wall after an emergency Hartmann's procedure.
Methods: An obese, 75-year-old woman, with history of breast cancer and previous diverticulitis, presented with an acute large bowel obstruction. CT images showed a strictured segment of sigmoid colon, with concentric wall thickening, described as inflammatory versus a possible malignancy. After a failed attempt of conservative treatment and colonic stenting she underwent emergency sigmoidectomy and colostomy.
Results: Two days after surgery she developed extensive erythema and cellulitis of the left flank, with an increase in sepsis markers and severe pain. CT imaging showed subcutaneous and fascial thickening, with liquid collections. The patient underwent emergency surgery with fasciotomy and debridement, intensive resuscitation therapy, and intravenous broad-spectrum antibiotics (Daptomycin, Meropenem, and Metronidazole). Cultures were positive for E. coli, Ampicillin-resistant E. faecium and Streptococci. A second intervention was performed for new debridement. The outcome was satisfactory. She was discharged 59 days after admission.
Conclusions: Necrotizing fasciitis demands early and aggressive surgery, intensive therapy, and antibiotics. Despite the poor prognosis, in some cases this treatment can be successful and achieve survival.
First Department of Surgery, Tzaneion General Hospital, Piraeus
Department of Radiology, Tzaneion General Hospital, Piraeus, Greece
INFECTED PANCREATIC NECROSIS SUCCESSFULLY MANAGED NON-OPERATIVELY IN AN ELDERLY PATIENT: A CASE REPORT
Background: Infected pancreatic necrosis in the context of severe pancreatitis is associated with high morbidity and mortality and is considered as a straightforward indication for debridement.
Aim: To present an elderly patient with infected pancreatic necrosis and abscess successfully managed non-operatively.
Methods: A 76-year-old male patient was admitted for acute gallstones pancreatitis. An abdominal computed tomography (CT) demonstrated pancreatic swelling, necrosis of the neck of the pancreas approximately 1.5 cm and peripancreatic fluid collections (Balthazar grade E and <30% necrosis, resulting in a CT severity index of 6 points). Laboratory tests showed an increased creatinine 1.8 mg% and C-reactive protein 316 mg%. An APACHE-II score of 8 points and Marshall score of 2 points were calculated. A second abdominal CT after four weeks demonstrated Balthazar grade E and >60% necrosis, with the presence of air in the lesser sac. Due to relapse of high-grade fevers a minimally invasive approach was decided on.
Results: Under local anesthesia and CT guidance a 7-Fr pigtail catheter was inserted in the pancreatic abscess. In the subsequent 10 days a total of approximately 1200 cc of pus was drained via the catheter and the patient recovered. After three weeks a second pigtail catheter was inserted in an adjacent area of the pancreatic abscess and the patient had an uneventful course and recovered completely. After 12 weeks from initial attack the patient was discharged.
Conclusions: Minimally invasive approaches may have a successful outcome without the need for debridement of necrotic material.
Toribio-GarcíaJ1Casas RoderaP2Casas RubioC2
University Hospital of León, Ophthalmology Service
University Hospital of León, Otolaryngoloy Service, Spain
ACUTE DACRYOCYSTITIS AFTER DACRYOCYSTECTOMY IN PATIENT WITH CHRONIC NASOSINUSAL POLYPOSIS
Background: Dacryocystectomy (DCT) is the best possible procedure in patients with dacryocystitis and dry eye or underlying medical conditions that might predispose to nasal scarring after standard dacryocystorhinostomy. Although DCT has a high rate of success removing the infection, a recurrence can develop in some cases.
Methods: A 73-year-old female patient underwent simultaneously endoscopic sinus surgery for naso-sinusal polyps and left DCT for acute dacryocystytis. Her past medical history included morbid obesity, diabetes mellitus type 2, arterial hypertension, bronchial asthma, angina pectoris, and chronic nasal polyposis that required several endoscopic operations. The patient had an important facial deformity caused by spreading of her nasal cavity by polyps. A big lacrimal sac that spread the lacrimal fossa bones was observed during dacryocystectomy. Lacrimal sac mucous was removed and superior and inferior lacrimal puncta were coagulated. Despite the initial success, the patient developed a new dacryocystitis in the left side 12 months after the first lacrimal surgery, so she underwent a new DCT. After 20 months of followup she did not develop a recurrence.
Results:
Conclusions: The authors report on a patient with several risk factors to suffer an infection. The initial DCT failed as a new dacryocystitis was developed. Although successful rate of DCT is very high, close to 95%, her general condition (obesity and diabetes) and her local conditions (enlarge lacrimal fossa and chronic nasal polyposis) promoted the formation of a new lacrimal sac and a new infection.