
Abstract
Abstract
Background:
Actinomycosis is a chronic granulomatous infection characterized by variable presentations, including disease states that can mimic neoplastic disease. A case is presented of actinomycosis that resembled metastatic carcinoma of the ovary.
Methods:
Case report and review of pertinent English-language literature.
Case Report:
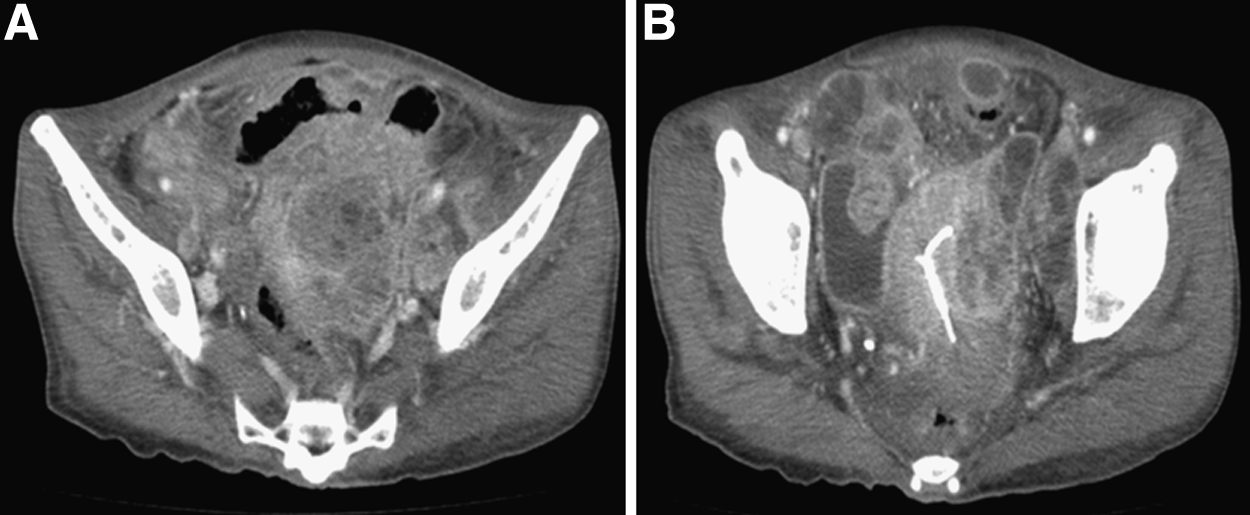
A 52-year-old female presented with a four-month history of abdominal discomfort and general weakness, and a two-month history of weight loss (8 kg). She had no history of medical disease. She had undergone exploratory laparotomy in the past because of ectopic pregnancy and she had used an intra-uterine contraceptive device for many years. Abdominal-pelvic computed tomography (CT) and pelvic magnetic resonance imaging (MRI) revealed a 5.9 × 6.4 cm heterogeneous enhancing pelvic soft tissue mass with central necrosis, probably arising from the left adnexa, and was consistent with ovarian cancer. She also had multiple peripheral enhancing cystic lesions in the pelvis, abdominal wall, both paracolic gutters, the root of the small bowel mesentery, the omentum, and Morison pouch. She had a moderate amount of ascites with diffuse peritoneal thickening consistent with carcinomatosis. An exploratory laparotomy was performed, showing multiple large abscesses with adhesions and a large soft tissue mass in the left pelvic cavity. After resection and drainage, final pathology was reported as actinomycosis. After her operation, she was given intravenous penicillin for six weeks and discharged.
Conclusion:
Surgeons and clinicians should be aware of this infectious disease because of its atypical symptoms and potential to mimic soft tissue tumors or malignant neoplasms.
A
Case Report
A 52-year-old female presented with a four-month history of abdominal discomfort and general weakness, and a two-month history of weight loss (8 kg). She had no medical disease history. She had undergone exploratory laparotomy because of ectopic pregnancy and she had used an IUD contraceptive device for many years. Laboratory testing revealed a white blood cell (WBC) count of 13,870 cells/mm3, C-reactive protein (CRP) 163.59 mg/L (reference range, 0-8 mg/L), hemoglobin concentration of 15.4 g/dL; tumor markers (α-fetoprotein, carcinoembryonic antigen (CEA), CA 125, CA 19-9) were normal. She had fever (39.0°C), abdominal discomfort, and generalized weakness. Abdominal-pelvic computed tomography (CT) and pelvic magnetic resonance imagery (MRI) revealed a 5.9×6.4 cm heterogeneous enhancing pelvic soft tissue mass with central necrosis. There were multiple peripheral enhancing cystic lesions in the pelvis, abdominal wall, both paracolic gutters, the root of the small bowel mesentery, the omentum, and Morison pouch. There was ascites and peritoneal thickening throughout the entire abdomen (Fig. 1–2). Fluorodeoxyglucose-positron emission tomography (FDG-PET) examination revealed intense FDG avidity in the pelvic mass, ascites, omental infiltration, and multiple peritoneal nodules. The impression was ovarian cancer with carcinomatosis.
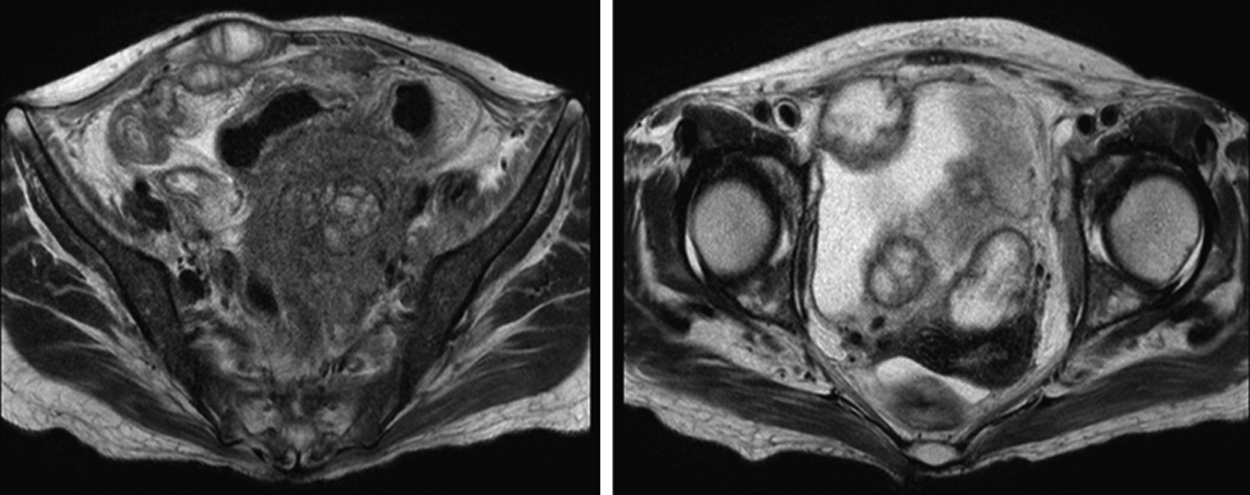
Magnetic resonance image showing multiple peripheral enhancing cystic lesions in the pelvis, abdominal wall, both paracolic gutters, root of the small bowel mesentery, omentum, and Morison pouch; moderate ascites with peritoneal thickening of the entire abdomen.
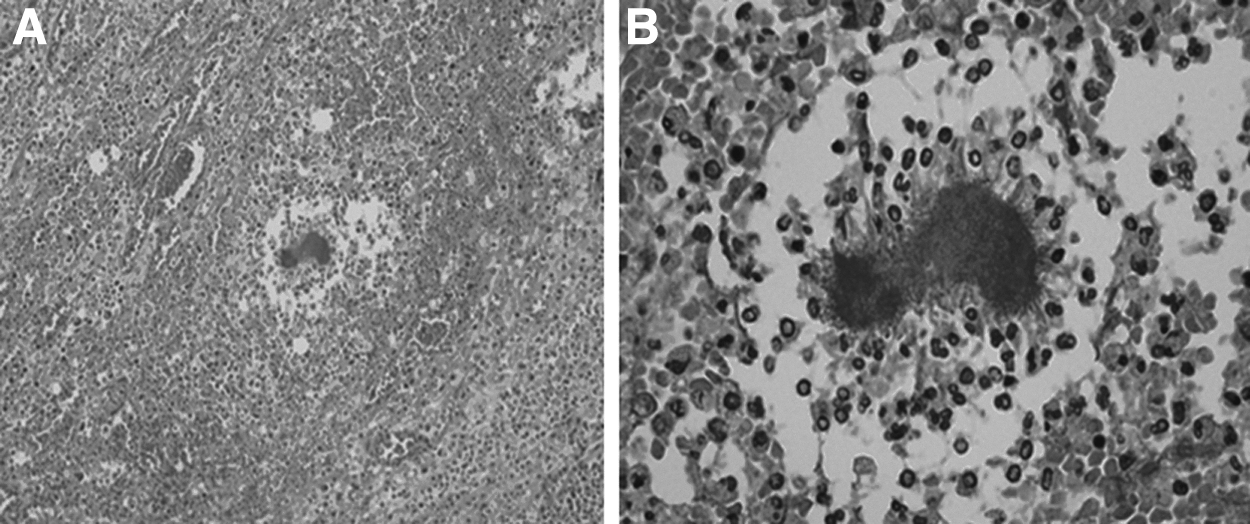
Exploratory laparotomy was performed for palliative debulking. Intraoperative inspection revealed multiple large abscesses with adhesions to small bowel, mesentery, omentum, and abdominal wall. Adhesiolysis was performed with abscess drainage and resection of the pelvic mass, segmental resection of the small bowel, final histopathology of the specimen removed actinomycosis (Figs. 3 and 4), with revealed extensive acute and chronic inflammation with macrophage aggregates in subserosa and serosa. After her operation, she received penicillin IV for six weeks, and was discharged.
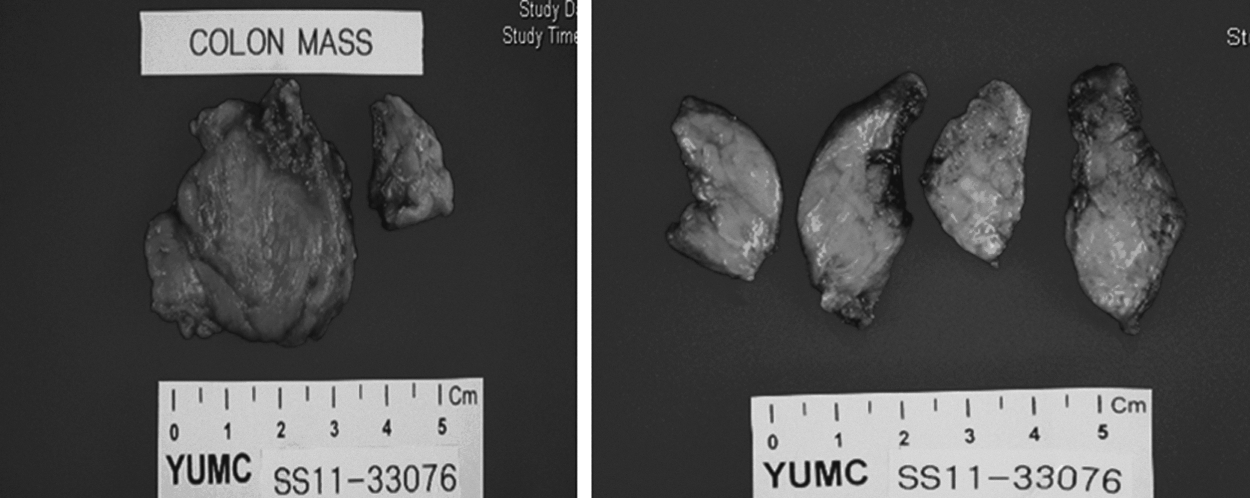
Resected soft tissue from the left pelvis, labeled “colon mass,” was in fact consistent with actinomycosis.
Discussion
Actinomyces is considered to be saprophytic in the oral cavity, gastrointestinal tract, and female genital tract. Some surgical triggers such as traumatic wounds, operation, placement of an IUD, and tooth extraction may disrupt mucosal barrier function, resulting in facilitation of invasion of the pathogen into deeper tissue from its original habitat. The organism is unable to cross normal mucosal barriers, therefore, opportunistic infections can occur only in the context of underlying local disease. Disruption of the mucosal barrier, or a history of perforated viscus are recognized as predisposing factors [4]. Abdominal actinomycosis usually occurs following a bowel perforation, especially perforated appendicitis, or following endometriosis from the use of an IUD. Pelvic actinomycosis has become more prevalent and is associated almost exclusively with use of an IUD, which may increase the risk of infection through injury to endometrium [5]. Actinomycosis israelii infects 1.65%–11.5% of IUD users, and infection is more common in women who have had an IUD in longer than four years. In females, actinomycosis may be initiated by oro-genital contact [6].
The definitive diagnosis is made by identification of the pathogen from a clinical specimen or from sulfur granules. However, microscopic identification is usually important because the recovery rate in culture is less than 30% [7], the diagnosis is made preoperatively in fewer than 10% of patients because of the low index of suspicion, unusual symptoms, and difficulty in confirming Actinomyces [8]. Variable clinical presentations for IUD-related Actinomyces have been described, which include abdominal pain, weight loss, and vaginal discharge. Patients sometimes present with fever associated with anemia and leucocytosis [8]. Actinomyces infection has also been misdiagnosed as pelvic neuplasm [9]. The initial pre-operative diagnosis of the present case was ovarian cancer with carcinomatosis. Recently, Katsuya et al. reported a high pre-operative detection rate of Actinomyces in IUD-bearing patients by cervical and endometrial cytology [12]. Pap smears might be considered for pre-operative diagnosis test [13].
Generally, treatment for actinomycosis involves high-dose intravenous penicillin G (24 million U/d) over two to six weeks, followed by oral penicillin V 2–4 g/d for six to 12 mon [10]. Also, treatment for IUD-induced abdominopelvic actinomycosis involves removal of the IUD [11].
In conclusion, abdominopelvic actinomycosis should be considered in patients with a cancer-like pelvic mass with possible carcinomatosis. Abdominal or pelvic actinomycosis must be considered for women with a history of IUD use. Surgeons should be aware of this entity because of its atypical presentation and potential to mimic soft tissue tumors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.