
Abstract
Abstract
Background:
Fungal valve endocarditis in children is an uncommon and lethal disease. The risk increases with use of central venous catheters (CVC), total parenteral nutrition (TPN), and use of broad-spectrum antibiotics during the neonatal period. Due to high mortality, a combination of surgery and antifungal therapy is usually recommended for treatment.
Methods:
Case report and review of the literature.
Results:
We present a case of an asymptomatic infant with multiple Candida tricuspid valve mycetomas. Complete cure was achieved by combined tricuspid valve repair and fluconazole therapy. We also review 26 cases of tricuspid valve Candida endocarditis in children published in the literature.
Conclusion:
From being uniformly fatal five decades ago to a current survival rate of 64% to 100%, the prognosis of Candida endocarditis has changed dramatically with the use of antifungal therapy alone or in combination with surgery. Our case re-emphasizes the role of valve-sparing debridement with repair of the native valve using autologous pericardium in combination with long-term antifungal therapy as a feasible option in managing tricuspid valve Candida endocarditis.
F
Case Report
A four-month-old asymptomatic male infant was diagnosed incidentally with a cardiac problem. The baby, born at term by cesarean section, developed fever and seizures on day 5 of life and was admitted in the neonatal intensive care unit for 10 d with a possible diagnosis of sepsis. Blood culture was negative. Patient received 7 d of broad-spectrum antibiotic through a peripheral venous line. There was no history of umbilical vessel catheterization or insertion of a central venous catheter. At 4 mo, the child was evaluated at a local hospital for systolic murmur and an echo was done, which showed an intracardiac mass. The patient was referred to our institute for further evaluation. On clinical examination, the infant was comfortable with no symptoms. Cardiovascular examination revealed a heart rate of 88 beats/min, normal S1 and a split S2 with a soft mid-diastolic murmur. A trans-thoracic 2D echocardiogram (IE33xMATRIX Echocardiography System, Philips, Eindhoven, The Netherlands) showed a mobile, irregular intracardiac mass, 10 mm×9 mm, attached to the anterior tricuspid leaflet (ATL), with excursion and out of the tricuspid valve (TCV) orifice (see online supplementary material Video S1, at http://www.liebertpub.com) There was a mild tricuspid valve inflow gradient of 6/3 mm Hg, no tricuspid regurgitation (TR), and no other structural lesions.
With a provisional diagnosis of cardiac myxoma, surgical excision was advised. After instituting cardiopulmonary bypass, the right atrium was opened and the left atrium was vented. Two grayish-white masses measuring 15×10 mm and 2×2 mm, respectively, were found attached to the ATL. Another mass of 4×4 mm was attached to the septal tricuspid leaflet (STL). All of them were excised and the ATL was repaired with gluteraldehyde-treated pericardium and two artificial chordae gap in the STL was repaired with direct suture closure. One chorda from the STL was translocated to the pericardial patch leaflet. By saline injection, no TR was found. The patient came off bypass on the first attempt with inotropic support.
The excised tissues were sent for histopathology and culture. On gross examination, the tissue was grayish-white, measuring 20×15×12 mm. The external surface was nodular (cauliflower-like) and the cut surface was grayish-white and granular. Microscopic examination of hematoxylin and eosin-stained tissue sections showed collections of a few yeast forms and numerous hyphae that were slender and elongated. Periodic acid Schiff (Fig. 2A), calcofluor white, and Gomori methenamine silver (Fig. 2B) stains also were positive for fungal elements. Neutrophilic infiltration also was observed along with fibrinous material. Culture of the tissue grew Candida albicans sensitive to fluconazole (<1 mcg/mL), amphoterecin B (<0.5 mcg/mL), itraconazole (<0.125 mcg/mL), voriconazole (<0.063 mcg/mL) and flucytosine (1 mcg/mL).
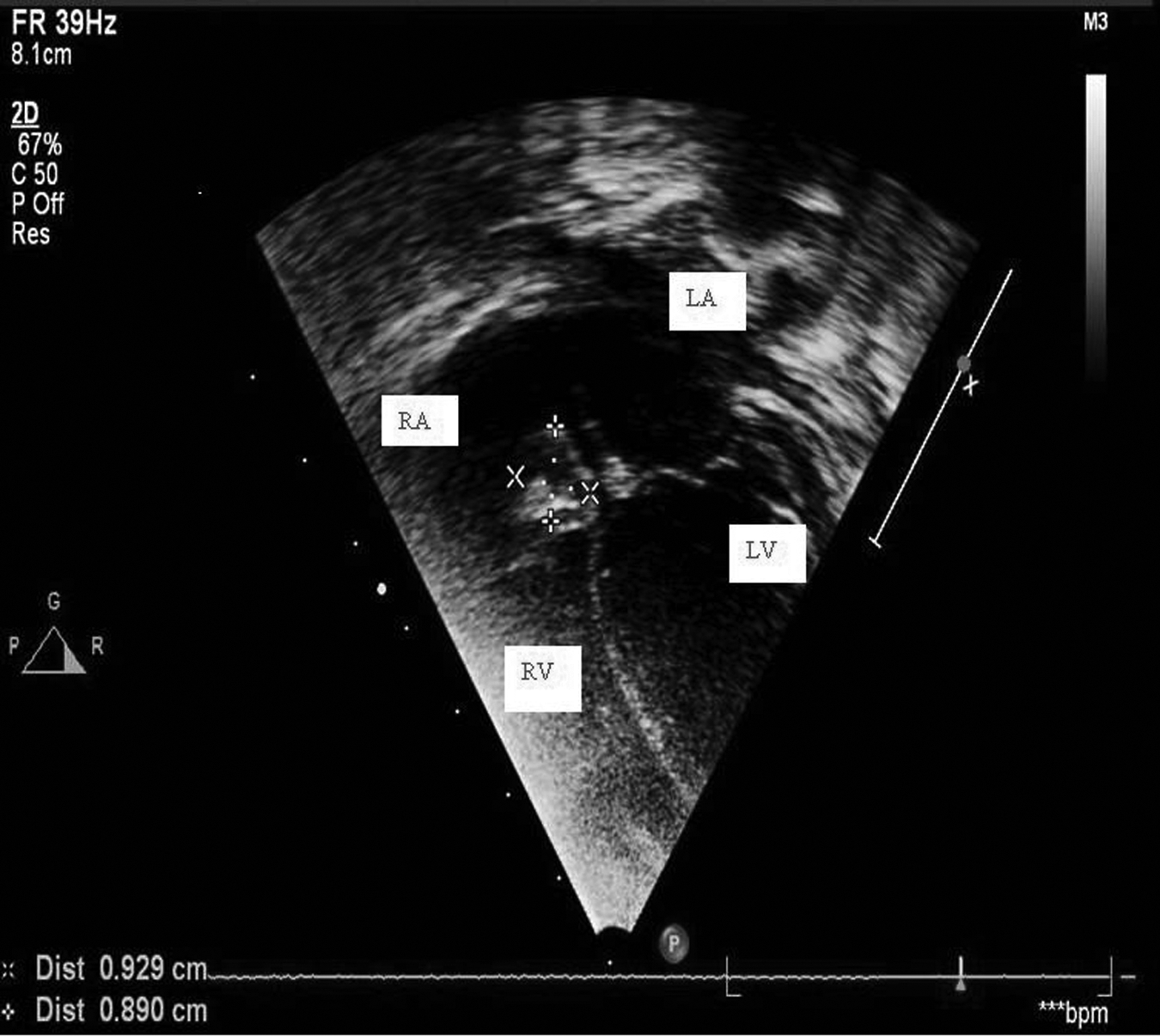
Transthoracic apical four-chamber view revealing a mass adherent to the tricuspid valve and prolapsing into the right ventricular cavity. LA=left atrium; RA=right atrium; LV=left ventricle; RV=right ventricle.www.liebertpub.com/sur

Transthoracic parasternal color Doppler view showing the tricuspid inflow. RV=right ventricle; RA=right atrium.www.liebertpub.com/sur
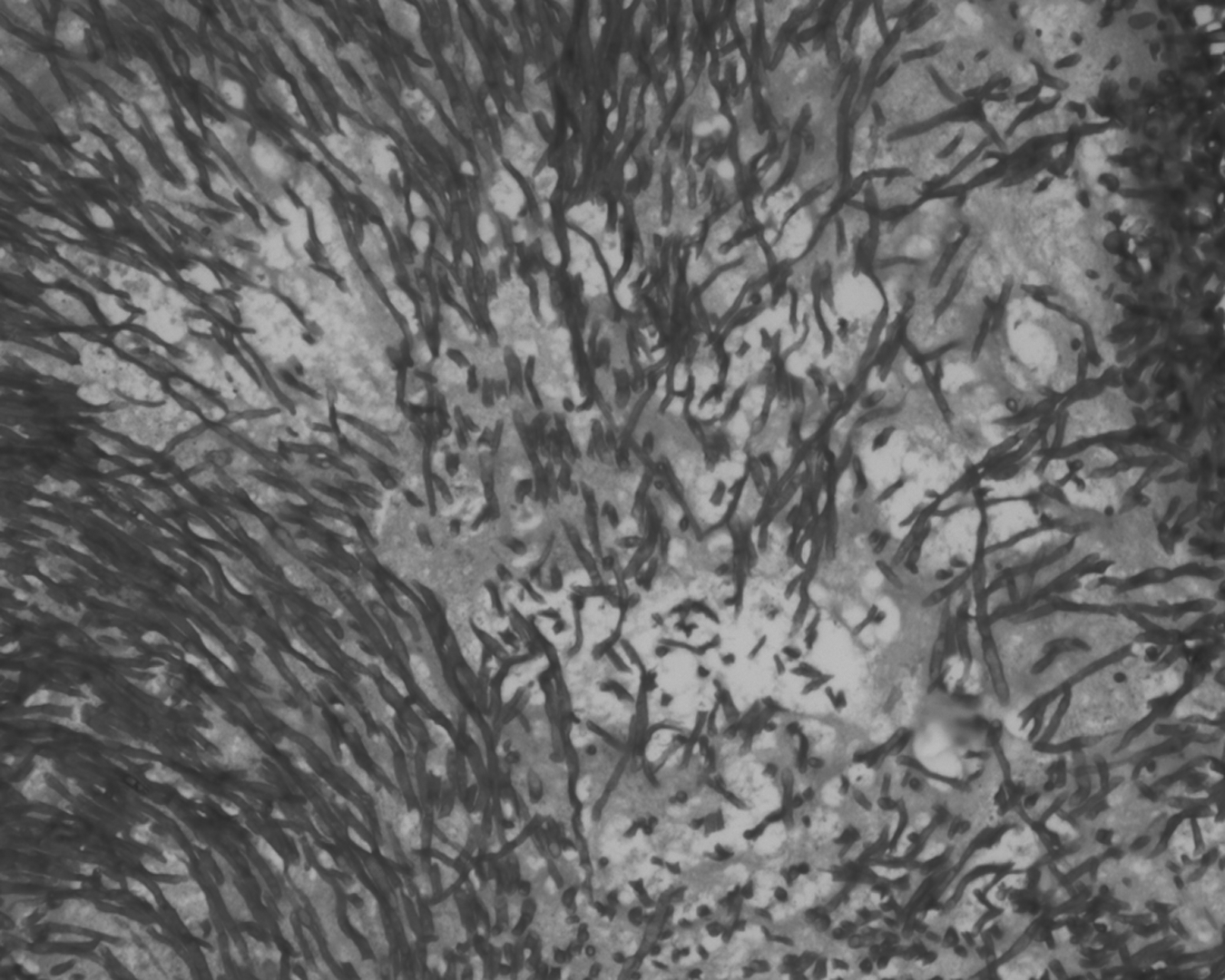
Histologic section of debrided tricuspid valve vegetation showing pseudohyphae and yeast forms (Periodic acid-Schiff;×400).www.liebertpub.com/sur
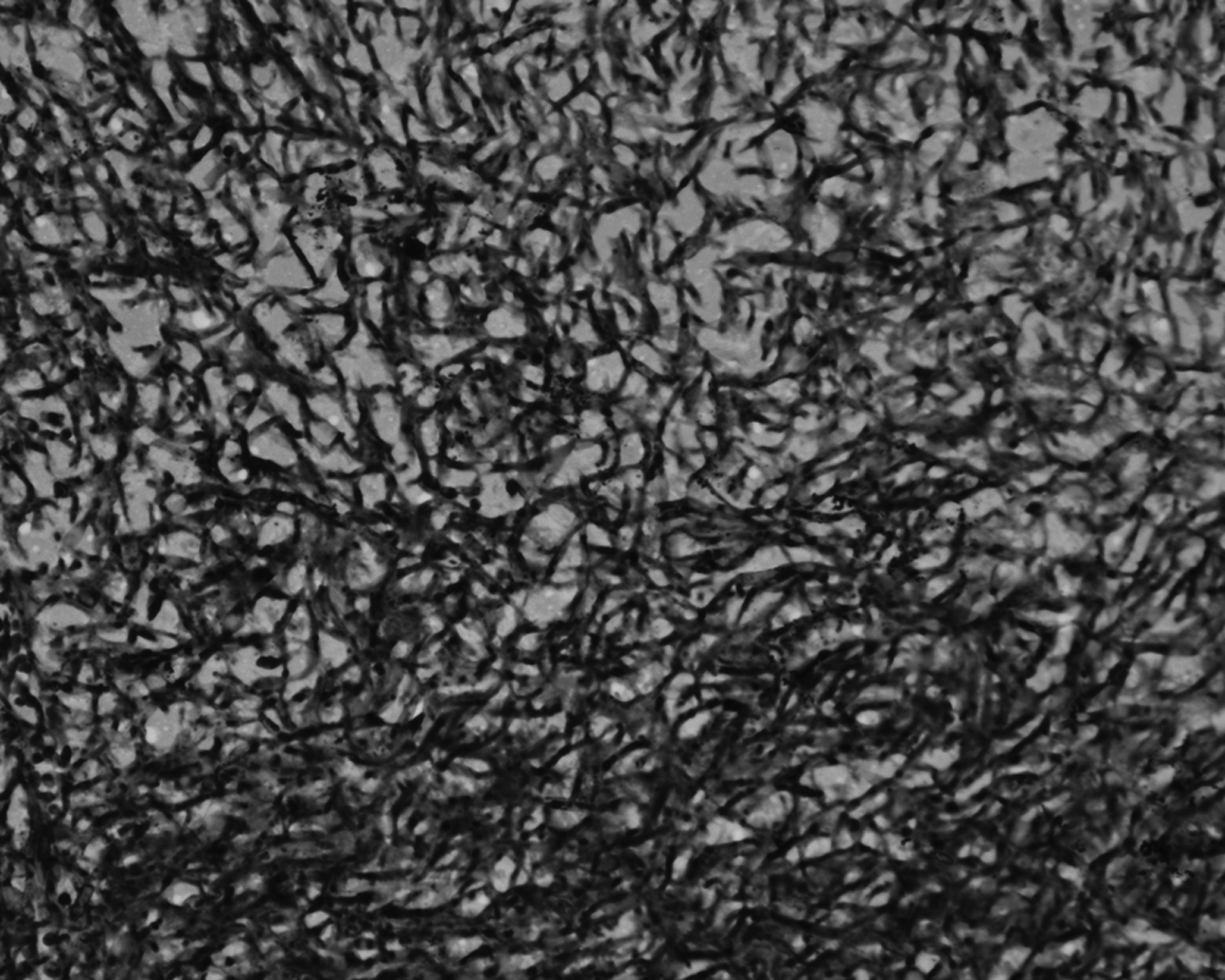
Histologic section of debrided tricuspid valve vegetation showing pseudohyphae (Gomori methenamine silver, x 400).www.liebertpub.com/sur
On the basis of histopathology findings, the diagnosis of Candida endocarditis was made and on the second post-operative day, the patient was started on fluconazole 70 mg intravenous (IV) loading dose followed by 40 mg IV daily. Post-operative echocardiogram showed mild TR, no pulmonary hypertension, and normal ventricular function (Fig. 3). The patient had an asymptomatic recovery and was discharged on oral fluconazole 8 mg/kg, which was increased as the child gained weight, for 6 mo.

Post-operative echo image. Apical four-chamber view showing no residual mass, unobstructed tricuspid inflow and mild tricuspid regurgitation. TV=tricuspid valve; RV=right ventricle; LV=left ventrical; MV=mitral valve.www.liebertpub.com/sur
The child is on regular follow up and was last seen 9 mo after surgery. A series of fungal blood cultures done at the second and third month also were negative. Follow-up transthoracic echocardiography at 9 mo demonstrated mild-to-moderate TR without any vegetations, and it was then decided to stop fluconazole. The patient remains clinically well, free from endocarditis without any medical treatment, at 9 mo follow-up.
Discussion
The incidence of endocarditis in pediatrics is 0.8 to 3.3%/1000 admission—especially in children with congenital heart diseases, of which 0.1% to 10% are of fungal origin [4]. Clinical signs of Candida endocarditis are a changing or new heart murmur, fever, repeated episodes of embolization, and heart failure [2]. Due to mortality rates as high as 40% to 80%, a combination of surgery with antifungal therapy (high-dose) is used uniformly for treatment [4,5]. Surgery helps in reducing the infectious focus, thereby reducing the fungal load and decreasing the destruction of cardiac structures and reducing complications [5]. The tricuspid valve is more commonly involved in intravenous drug abuse while the aortic and mitral valves are more frequently involved in prosthetic valve endocarditis [6]. Tricuspid valve endocarditis in patients with a normal heart is rare, making their diagnosis difficult. The widespread use of echocardiography has improved the diagnostic acumen for TVCE. The pathogenesis of TVCE may be due to formation of a fibrin/platelet bed subsequent to a malformed TCV, trauma to endothelium, mechanical stress, or turbulent blood flow, providing a nidus for Candida during transient candidemias [7]. It is also postulated that Candida adheres to non-bacterial thrombotic endocarditis on the TCV caused by an underlying medical condition, resulting in TVCE [8]. The diagnosis of fungal endocarditis requires a high index of suspicion as the children are not very sick and clinical manifestations are subtle [6]. Among all fungal species, Candida is the most prevalent. About 3% of all cases of endocarditis are caused by Candida spp. [9]. Previous studies have reported that in Candida endocarditis, the isolated microorganism is more likely to be non-albicans if the duration of illness is longer [8]. The diagnostic criteria for fungal endocarditis include the presence of an intra-atrial mass in a background of candidemia and negative bacterial blood cultures. The problem is compounded further by the fact that fungal blood cultures are negative in one-third of cases and molecular diagnostics are not usually available readily. The general consensus for treating Candida endocarditis involves surgical correction followed by long-term antifungal therapy. Surgery is deferred only in critically ill patients who cannot tolerate the procedure. Amphoterecin B with or without flucytocine is given for eight weeks followed by fluconazole for 2–4 y [6]. However, complete cure without surgery using combinations of amphoterecin B with either fluconazole or itraconazole, or with fluconazole alone for 6–8 mo have been reported [10]. The success of antifungal therapy depends on the size of the vegetations and the minimum inhibitory concentration of the isolate. Vegetations <10 mm in diameter respond well to antibiotic therapy, whereas with large vegetations (>20 mm) penetration of antifungals is poor and there is an increased risk of embolization, especially in right-sided endocarditis [11]. Surgical excision of TCV in young infants has been unsuccessful due to lower right ventricular compliance and high pulmonary vascular resistance [11]. Due to thrombotic complications and ingrowth of tissue, use of mechanical prostheses also has lost favor with surgeons [5]. Simple excision of vegetations—also known as “vegetectomy,” or complex tricuspid valve repair involving excision of involved valve tissue with pericardial repair, chordal translocation, and bicuspidalization of the valve—is being used increasingly rather than complete valvular excision [11]. Limitations of routine surgical techniques, such as antigenicity of new implanted tissue, complications related to permanent anti-coagulation, thrombotic complications secondary to synthetic valves, and mismatch in configuration of prosthetic valve substitutes can be avoided with the use of autologous pericardium to reconstruct a valve [12].
Due to the rarity of TVCE in infants, we did a computer-based search (MEDLINE; years, 1977–2012) and identified 26 additional cases reported previously (Table 1 [13–30]). In total there were nine male, eight female, and nine in which gender was unspecified. Isolated TCV involvement was seen in 57.6% (15/26) cases. Various risk factors prior to antibiotic therapy were documented in 53.8% (14/26) of cases, prematurity in 27% (7/26) of cases, CVC in 50% (13/26 of cases), TPN in 23% (6/26) of cases, and CHD in 15.3% (4/26) of cases. Candida albicans (57.6%; 15/26) was isolated most commonly followed by C. tropicalis in (15.3%; 4/26), C. parapsilosis in (7.6%; 2/26), and one case each of C. glabrata, C. krusei, and Khodamea ohemri. In 7.6% (2/26) of cases, Candida isolates were not speciated. Details of treatment were available for 21 cases, of which the majority (90.4%; 19/21) were treated with amphoterecin B alone or in combination with flucytocine or fluconazole. Fluconazole in combination with surgery was used in two cases, including the present one. Caspofungin was used in one case with a favorable outcome. Combination of surgical correction with antifungal therapy was used in 66.6% (14/21) of cases, of which 85.7% (12/14) survived. Of the 38% (8/21) of cases treated only with an antifungal agent, 75% (6/8) survived.
AmpB=amphotericin B; CVC=central venous catheter; 5FC=flucytosine; IC=indwelling catheter; ICD=intercostal drainage; IUGR=intrauterine growth retardation; Lip=liposomal; MV=mitral valve; NA=not available; PA=pulmonary artery; PDA=patent ductus arteriosus; PV=pulmonary valve; RA=right atrium; RV=right ventricle; spp=species; SVC=superior vena cava; TCV=tricuspid valve; TEF=tetralogy of Fallot; TPN=total parenteral nutrition; VSD=ventricular septal defect; wk=weeks.
From being uniformly fatal five decades ago to a survival rate of 64% to 100%, the prognosis of Candida endocarditis has changed dramatically with the use of antifungal therapy alone or in combination with surgery [2]. Our case re-emphasizes the role of valve-sparing debridement with repair of the native valve using autologous pericardium in combination with long term antifungal therapy as a feasible option in managing TVCE.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.