
Abstract
Abstract
Objectives:
We sought to examine whether vacuum-assisted closure (VAC) is associated with fewer surgical site infections (SSIs) or infections of chronic wounds than other management procedures for surgical wounds.
Methods:
The PubMed and Scopus databases were searched systematically. Randomized controlled trials (RCTs) comparing the development of SSIs or infections of chronic wounds between patients treated with VAC for acute or chronic wounds and those whose wounds were treated without VAC were considered eligible for inclusion in the study.
Results:
Eight RCTs met the inclusion criteria for the study. Four of the studies included chronic or diabetic lower extremity wounds and four included fractures. In three of four studies reporting on fractures, the wounds were not closed post-operatively, whereas in one study primary closure of the wound was performed. With regard to wounds left open after the stabilization of fractures, patients whose wounds were treated with VAC developed fewer SSIs than those whose wounds were treated without VAC ([367 patients (196 with VAC; 171 without VAC) relative risk [RR], 0.47; 95% CI 0.28–0.81]). On the contrary, no difference in the development of SSIs occurred among patients with chronic or diabetic lower-extremity wounds treated with VAC and those whose wounds were treated without VAC ([638 patients (320 with VAC; 318 without VAC) RR 1.67; 95% CI: 0.71–3.94]).
Conclusion:
The available evidence suggests that the development of infections in wounds treated with VAC depends on the type of wound being treated.
S
However, wound healing can occasionally be delayed by diabetes mellitus, impaired perfusion, or increased age, and can be complicated by local infections [5–8]. Animal studies have shown that VAC optimizes blood perfusion, decreases local edema by removing excess interstitial fluid, and reduces the bacterial load [9,10]. More specifically, the increased blood flow and, subsequently, increased local tissue oxygenation achieved with VAC reduces the growth of anaerobic bacteria and makes greater amounts of oxygen available to neutrophils for the oxidative bursts that kill bacteria [10].
In this context, we sought to review systematically and synthesize, through meta-analysis, the available evidence, to determine whether wound therapy with VAC was superior to other wound therapies in terms of the development of surgical site infections (SSIs) or infections of chronic wounds.
Materials and Methods
Literature search
We conducted a systematic search in the PubMed and Scopus databases in September 2012, using, in the PubMed, the search terms “negative pressure” or “VAC” or “vacuum assisted” and “wound” and “infection.” The search of Scopus was limited to randomized studies, with use of the terms “negative pressure” or “VAC” or “vacuum assisted” and “wound” and “infection” and “randomized.” To identify further relevant studies, we also conducted a manual search of the bibliographies of all eligible or potentially eligible articles in the PubMed and Scopus databases. Articles written in a language other than English, French, German, Spanish, Italian, or Greek were not evaluated.
Study selection
Randomized controlled trials (RCTs) on the development of superficial and deep incisional SSIs or infections of chronic wounds in patients treated with or without VAC for acute or chronic wounds were considered eligible for inclusion in the meta-analysis. Studies were excluded if more than 10% of the patients in the study had SSIs or infections of chronic wounds at enrollment and data for this specific subpopulation were not provided.
Data extraction
The data extracted from the studies included in the meta analysis consisted of their main characteristics (first author, country, period of the study, study design), number of patients, types of wounds, types of infections developing after wound therapy, and funding. Evaluation of the quality of the included studies was done with a modified Jadad scale [11].
Definitions and outcomes
Surgical site infections, defined according to the criteria of the U.S. Centers for Disease Control and Prevention (CDC) [12], consisted of both superficial and deep incisional infections. Chronic ulcers of the lower extremity or wounds associated with severe chronic diseases were defined as chronic wounds and their infections as “infections of chronic wounds.” The outcome measure of the meta-analysis was the development of SSIs or infections of chronic wounds among patients treated with VAC or therapies other than VAC for the healing of acute or chronic uninfected wounds.
Statistical analysis
The meta-analysis conducted in the study was done with Review Manager for Windows, version 5.1 (Nordic Cochrane Centre of the Cochrane Collaboration, Copenhagen, Denmark). A random effects model (REM) was used to estimate pooled risk ratios (RR) and 95% confidence intervals (CIs). Statistical heterogeneity among the studies on which the meta-analysis was based was assessed with the χ2 test (with a value of p<0.10 defined as indicating heterogeneity) and the I2 statistic for assessing the degree of heterogeneity.
Results
A total of 854 articles were retrieved during the search process (754 PubMed, 81 Scopus, 19 manual searching). The study selection process is shown in Figure 1. Seven articles, involving a total of 1,049 patients, met the inclusion criteria for the present study [13–19]. One retrieved article included two studies [19]. Table 1 presents the characteristics of the included studies.
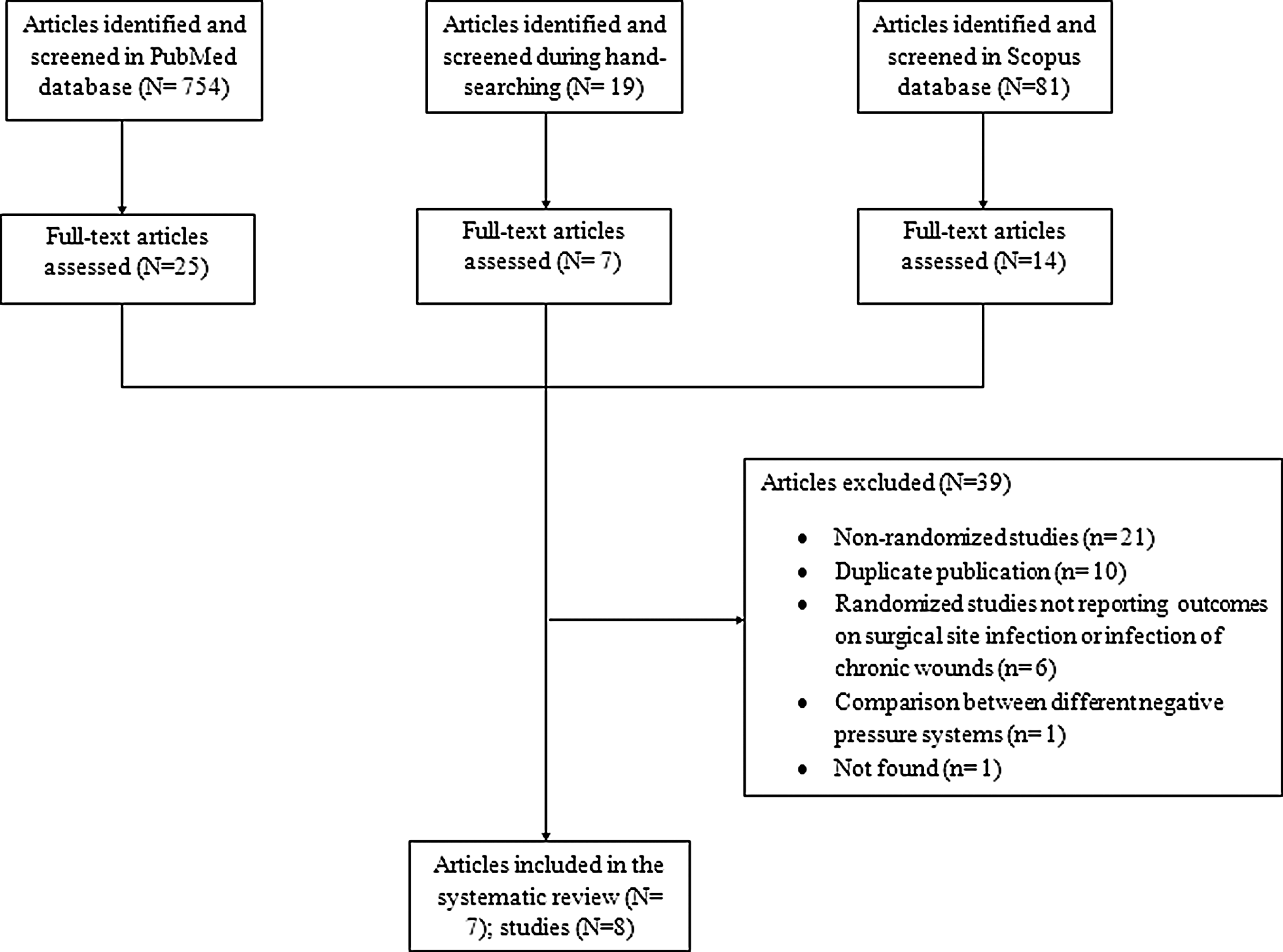
Flow diagram of systematic search and study selection process.
No funding was reported in the study.
In this study, 3.8% of fractures were open.
The wounds were left open after the stabilization of the fractures in these studies.
These fractures were primarily closed post-operatively.
In these studies, the authors did not specify whether the fractures were open or closed.
MC=multi-center; SC=single-center; RCT=randomized controlled trial; SSI=surgical site infection; NR=not reported; fxs=fractures.
Four studies reported on wounds after fractures [16–18] and four studies reported on chronic wounds [13–15,19]. In three of the studies that reported on wounds after fractures, wounds were left open after stabilization of the fractures [16–18], whereas in the fourth study primary closure of the wound was performed postoperatively [16]. Among the studies reporting on chronic wounds, two of the studies reported on diabetic foot amputation and diabetic foot ulcers, respectively [13,14]; one study reported on a variety of wounds (91% of them in the lower extremity) [15]; and one study reported on chronic (>6 mo duration) leg ulcers [19]. Six out of seven articles were funded by the manufacturer of the VAC system used in the study [13,14,16–19]. In the remaining article, the source of financial support was not reported, but two of the authors served as consultants to the manufacturer of the VAC system used in the study [15]. Four of seven articles had a low Jadad score [15–18].
Pooling of the outcomes of the included studies was done according to the type of wound treated in each study. Among patients with wounds that were left open after the stabilization of a fracture, those treated with VAC therapy had fewer SSIs than those whose treatment did not include VAC (Fig. 2) ([367 patients (196 with VAC; 171 without VAC) RR, 0.47; 95% CI 0.28–0.81]). In one study that reported on closed wounds closed primarily after the stabilization of the fractures, no difference in the development of SSIs was observed in patients treated with VAC and those treated without VAC (Fig. 2) ([44 patients (13 with VAC; 31 without VAC) RR, 0.48; 95% CI 0.06–3.69]). Among patients with chronic wounds, no difference in the development of infections of the wound bed was found in patients treated with VAC therapy and those treated without VAC (Fig. 2); [638 patients (320 with VAC; 318 without VAC) RR, 1.67; 95% CI 0.71,3.94]). Moderate heterogeneity among studies was detected in the analysis of patients with chronic wounds (I2=39%), whereas no heterogeneity was detected in the analysis of patients with fractures.

Forest plot depicting risk ratios for development of surgical site infections among patients treated for acute or chronic wounds. (Vertical line represent point of no difference between vacuum-assisted closure (VAC) and non-VAC regimens. Squares=risk ratios; diamonds=pooled risk ratios for all studies. Horizontal lines=95% CIs).
Discussion
The main finding of the meta-analysis of RCTs was that among patients with wounds that were left open after the stabilization of fractures, significantly fewer SSIs developed in those treated with VAC than in those treated without VAC. In contrast, among patients whose wounds were primarily chronic foot ulcers, no difference was found in the development of infections of the wound bed between those treated with VAC and those who were given other treatment.
Meta-analyses have suggested that VAC achieves faster wound healing than treatment without VAC [3,4]. Theoretically, faster healing should be accompanied by fewer infections of the wound bed. According to the findings of the present meta-analysis, based on data so far available, VAC does not prevent infections in chronic open wounds but does so in acute wounds caused by fractures. Therefore, the superiority of VAC over treatment without VAC, as found in the present analysis of SSIs in patients with fractures, could be attributed to the more rapid wound healing achieved with VAC than treatment without VAC. However, this cannot be verified by the findings of the present study for patients with chronic foot ulcers, among whom VAC was not associated with fewer infections than was treatment without VAC. A possible explanation for this discrepancy could be the greater microbial inoculum present in chronic wounds than in acute wounds at the time of application of VAC. In addition, patients with diabetes mellitus, who constituted the majority of patients with chronic ulcers in the present study, have impaired wound healing that delays the formation of mature granulation tissue [20]. Delay in wound healing may lead to the development of local complications such as infections. However, in three of four randomized studies on diabetic foot ulcer that were included in the present study, more patients healed and the rate of wound closure was more rapid with VAC than without VAC [13,14,19]. In one of these studies, no comparative data were provided [15]. In all four studies, the patients in the compared groups had similar characteristics.
The findings of the current study should be interpreted in light of several limitations. All but one RCT was funded by the manufacturer of the VAC system used in the RCT. Thus, the role of the funding source could not be evaluated as a source of potential bias in the results of these studies, because studies funded by other organizations (i.e., universities) besides manufacturers of VAC systems were not available. In addition, one study in which 91% of the patients had ulcers of the lower extremity and 9% ulcers at other sites (abdomen, back, and groin) was included in the group of studies reporting on chronic wounds of the lower extremity. Lastly, a separate presentation of the results according to the type of wound (superficial or deep) that was treated could not be done because the individual studies did not present relevant results.
The currently available evidence derived from randomized studies suggests that the development of SSIs is less common among patients with open fractures treated with VAC than among patients with open fractures treated without VAC. On the other hand, the available evidence from randomized studies also suggests that there is no difference in the development of infections of the wound bed in patients with chronic or diabetic wounds of the lower extremity treated with and without VAC. Further randomized studies, designed specifically to clarify this issue, are needed to confirm the findings of the present study for individual wounds.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest in the work described here.