
Abstract
Abstract
Background:
The aim of the study was to investigate the value of serum procalcitonin (PCT) as a predictor of early antibiotic treatment response in patients with acute appendicitis. Procalcitonin is a biochemical marker that increases rapidly in cases of bacterial infection and sepsis; however, the benefit of PCT as a diagnostic tool in acute appendicitis has not been confirmed.
Methods:
Observations of PCT dynamics were conducted as part of a prospective clinical trial at Sahlgrenska University Hospital between May 2009 and February 2010 on adult patients with acute appendicitis treated with antibiotics as first-line therapy. Procalcitonin, C-reactive protein (CRP), and white blood cell count (WBC) were measured before administration of antibiotics and subsequently between 4–24 h following treatment.
Results:
Three hundred sixteen patients were included in the study. Almost 80% recovered on antibiotics without the need of surgery. Serum PCT concentrations before initiation of antibiotic therapy and during treatment did not differ significantly between antibiotic responders and non-responders (p<0.94). However, differences were observed for CRP (p<0.04) and WBC (p<0.001), with a trend for body temperature (p<0.06).
Conclusion:
Procalcitonin has limited additional value, compared with standard laboratory tests as CRP, WBC, and body temperature to predict antibiotic treatment response in adult patients with acute appendicitis.
A
Procalcitonin (PCT) is a precursor of calcitonin and a sensitive laboratory indicator of severe bacterial infection and sepsis. However, the role of PCT, in relationship to traditional inflammatory markers such as C-reactive protein (CRP), white blood cell count (WBC), and body temperature is not yet defined. Procalcitonin correlates closely to bacterial infections and may have faster dynamics, compared with CRP and WBC [13], with evidence of benefit in patients with severe sepsis and patients with respiratory tract infections to support decisions regarding initiation and termination of antibiotic therapy [14–19]. The diagnostic role of PCT regarding acute appendicitis is not elucidated fully, although a recently-published meta-analysis concluded that PCT has little value in diagnosing acute appendicitis in general but may be of greater value in identifying advanced appendicitis [20]. In the present study, we investigated whether PCT could predict antibiotic response early on in adult patients with acute appendicitis.
Patients and Methods
Procalcitonin patterns in patients with acute appendicitis were observed prospectively during treatment with antibiotics as sole therapy. The study was conducted as a parallel part of a prospective non-randomized clinical trial of adult patients with acute appendicitis offered antibiotics as first-line therapy instead of traditional appendectomy [9]. The study took place at the surgical clinics of Sahlgrenska University Hospital in Gothenburg, Sweden between May 2009 and February 2010 and was approved by the regional Committee of Ethics in Gothenburg, Sweden (367-08).
Antibiotic treatment
The antibiotic treatment in the study is described in detail elsewhere [9]. In brief, antibiotics were considered the first choice of treatment but surgeons could decide to perform primary surgery when judged necessary for medical reasons (e.g., high fever, sepsis, or generalized peritonitis) or when patients themselves insisted on the procedure. Patients with recurrent appendicitis (following previous treatment with antibiotics) or pregnancy were excluded from the study and had traditional treatment with surgery (Fig. 1). Intravenous antibiotic (piperacillin-tazobactam 4.5 g 8 h) was administered for at least three doses. Improvement of the clinical status within 12–24 h allowed discharge from the hospital with oral antibiotics (ciprofloxacin and metronidazole) for an additional 9 d of treatment. Assessment of the clinical condition was based on abdominal status, pain, body temperature and blood tests (CRP, WBC). Intravenous antibiotic therapy could be prolonged for another 24 h if there was no clear-cut improvement in clinical condition. Rescue appendectomy was performed when the antibiotic therapy was considered a failure due to clinical deterioration or lack of obvious clinical improvement.

Flow chart for inclusion of 316 adult patients and outcome of antibiotic treatment. N=number of patients
Laboratory testing
Blood samples for analyses of PCT, as well as standard laboratory tests (CRP, WBC), and body temperature were taken as baseline registrations before administration of antibiotics. Subsequently, repeated analyses of PCT, CRP, WBC, and body temperature were made between 4–24 h following the start of antibiotic infusion. Analyses of PCT were strictly observational without any influence on clinical decisions. Serum PCT concentrations were analysed by an immunoflourescense assay (Thermo Fischer, Kryptor, Waltham, MA; TRACE-technique). Concentrations of less than 0.05 ng/mL were defined as normal values for adult patients.
Inclusion criteria
Eligible patients in the present study were adults with presumed acute appendicitis treated with antibiotics [9]. These patients were included if PCT measurements had been performed prior to the administration of intravenous antibiotics (Fig. 1).
Statistical analysis
Chi-square Testing was used to check for differences between proportions. Independent sample student t-test was used for comparison of continuous variables between groups, as well as paired sample student t-test when appropriate. Non-parametric tests were used for PCT, because of a lack of normal distribution. A p value of less than 0.05 was considered significant in two-tailed tests. The statistical calculations were performed with SPSS® version 19.0 (SPSS, Inc., Chicago, IL). Analysis of variance for repeated measures were used to compare differences before and during antibiotic treatment among responders and non-responders.
Results
During the study period, 558 consecutive adult patients were diagnosed with presumed acute appendicitis (Fig. 1). Subsequently, 442 patients actually received antibiotic therapy as primary therapy, whereas 111 patients had primary surgery according to their own choice or the decisions of surgeons. Procalcitonin analyses were performed in 316 of the 442 patients on antibiotic treatment, and these 316 patients were thus included in the present study.
A total of 249 patients (79%) recovered on antibiotics (“responders”) and 67 (21%) did not improve and therefore had subsequent rescue appendectomy (“non-responders”; Fig. 1). The outcome of antibiotic treatment for included patients was similar to outcomes of 442 patients as reported elsewhere [9].
Baseline characteristics
Clinical and laboratory parameters at diagnosis of acute appendicitis before administration of antibiotics are shown in Table 1. Pre-treatment mean concentration of PCT did not differ significantly between responders and non-responders (p<0.52), whereas WCC and body temperature showed lower mean concentrations among responders (p<0.01).
Mean±standard error of the mean
Values within parentheses are percentages
M=male; F=female; CRP=C-reactive protein; WBC=white blood cell count; PCT=procalcitonin.
Inflammatory parameters before and after administration of antibiotics
Table 2 shows laboratory parameters and body temperature assessed before the administration of intravenous antibiotic and subsequently across 4–24 h after the start of therapy. Procalcitonin serum concentrations did not differ among responders and non-responders during 4–24 h on antibiotic treatment (p<0.94; Table. 2). Mean concentrations of CRP (p<0.01), WBC (p<0.01), and body temperature (p<0.01) were significantly higher during antibiotic therapy in non-responders, compared with responders (Table 2; Fig. 2A and 2B). However, only CRP (p<0.04) and WBC (p<0.001) were different between responders and non-responders when considering all serum parameters over time (“before treatment” and “during treatment”), and with a trend for body temperature (p<0.06; Table 2).
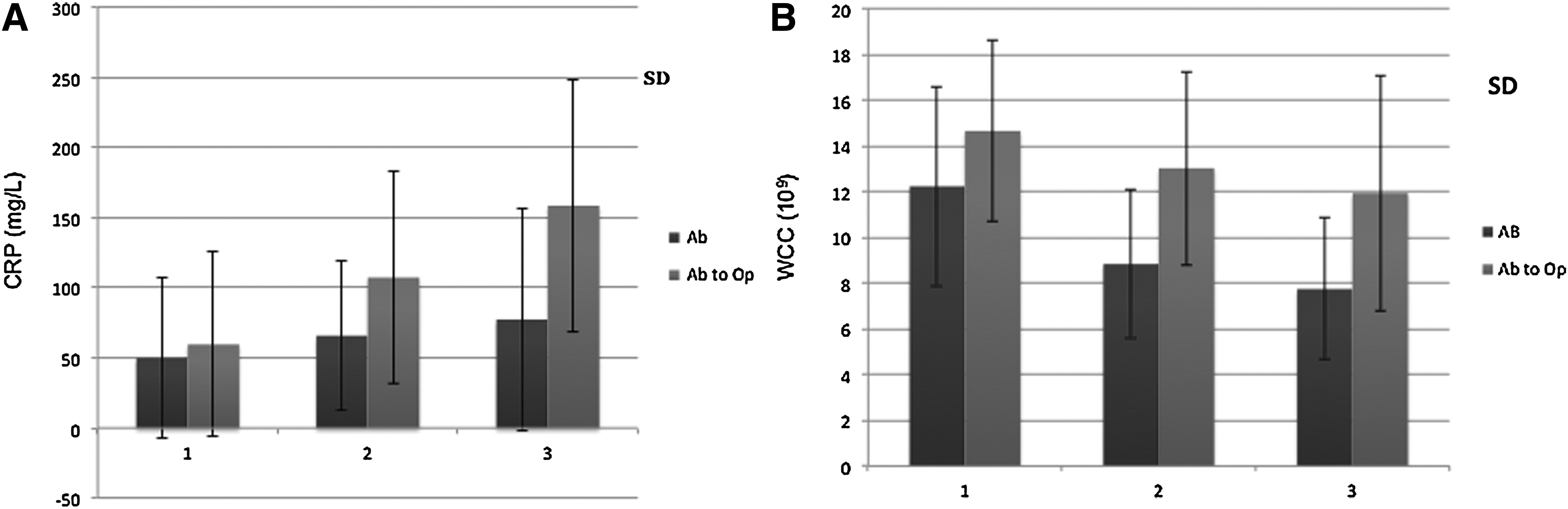
Time course changes of C-reactive protein in antibiotic responders (Ab) versus non-responders (Ab to Op). 1 is before administration of antibiotics and 2 and 3 are values at subsequent occasions after 4−24 h of therapy. Time course of changes of white blood cell count as described in the legend to Figure 2A. (Mean; SD=standard deviation.)
Mean±standard error of the mean
a) 249 patients
b) 67 patients
c) Number of observations during the first 24 h following the administration of antibiotic infusion
d) Interaction over time between responders and non-responders
ANOVA=analysis of variance; PCT=procalcitonin; CRP=C-reactive protein; WBC=white blood cell count; temp=temperature.
Procalcitonin in pre-treatment prediction of antibiotic response
The ability of PCT to predict antibiotic response before the start of therapy is shown in Table 3A. For low cut-off values the sensitivity was poor, and vice versa. The specificity was especially low for high cut-off values. Hence, the positive predictive value (PPV; probability for antibiotic response if the test is positive) were approximately 80% and the negative predictive values (NPV; probability for non-response if the test is negative) were only 20–25%. These predictive values were the same as the proportions of response and non-response for the whole group, and therefore did not contribute at all in the prediction of antibiotic response.
PCT=procalcitonin [ng/mL]; PPV=positive predictive value; NPV=negative predictive value.
PCT in prediction of antibiotic response after initiation of therapy
The ability of PCT to predict antibiotic response, when analyzed 4–24 h after initiation of therapy, is shown in Table 3B. For low cut-off values, the PPV of PCT was over 85%, which was slightly higher than for the whole patient group (antibiotic response, 79%). For high cut-off values, the NPV of PCT was above 30%, somewhat higher than for the whole patient group (non-response, 21%).
PCT=procalcitonin [ng/mL]; PPV=positive predictive value; NPV=negative predictive value.
Inflammatory parameters in prediction of antibiotic response
The ability to predict antibiotic response by relative changes in levels of PCT, CRP, and WCC (instead of absolute values) after initiation of therapy is shown in Table 3C. Patients with decreased or unchanged PCT after 4–24 h of antibiotic therapy had an antibiotic response rate of 91%, compared with 79% for the whole group. The PPV for decreased or unchanged CRP was even higher (94%). However, the NPV remained low for both PCT and CRP.
PCT=procalcitonin; CRP=C-reactive protein; WBC=white blood cell count; PPV=positive predictive value; NPV=negative predictive value.
Discussion
During the past decade, there has been a great deal of interest for PCT as a diagnostic and prognostic biomarker of bacterial infection and antibiotic therapy. There is good evidence to use PCT algorithms to make decisions about appropriate and effective antibiotic therapy in patients with severe sepsis in critical care settings, as well as in patients with respiratory tract infections [13,15–19]. Sequential measurements of PCT in particular may reflect the efficiency of various antibiotic therapies. The mortality for patients with severe sepsis has been reported to improve when serum PCT concentrations decrease more than 50% within 72 h after institution of therapy [21], whereas a decline in PCT values was more important than the absolute values. Furthermore, PCT cut-off concentrations within 24 h of the onset in sepsis could reflect outcome and mortality [22]. Procalcitonin also has proved to be substantially elevated among adult patients with perforated or gangrenous appendix, but with poor sensitivity that limits its routine use in diagnosis of acute appendicitis [20,23]. In children with acute appendicitis, PCT concentrations of more than 0.5 ng/mL have been associated with perforation or gangrene of the appendix [24].
Our present analyses showed no significant difference in pre-treatment PCT between antibiotic responders and non-responders with acute appendicitis (Table 2). Pre-treatment predictions of antibiotic response, based on serum PCT concentrations, did not exceed treatment prediction by chance (Table 3A), and PCT concentrations across the entire initial treatment period did not differ between responders and non-responders (Table 2). The predictive values of PCT also were too low to be used to identify antibiotic non-responders at an early stage of treatment (Table 3B). The probability of recovery on antibiotics was 91% in analyses of results based on relative changes in serum PCT concentrations, instead of absolute concentrations, when PCT remained unchanged or decreased (Table 3C); however, CRP showed a numerically higher degree of prediction. Thus, for patients with acute appendicitis treated with antibiotics as their first-line therapy, our analyses demonstrate that PCT has limited value, compared with traditional laboratory tests and clinical assessments in prediction of antibiotic efficiency, either before provision of antibiotics or early on following the start of antibiotic therapy [25]. In conclusion, PCT is of little value in use of antibiotic selection and prediction of response to antibiotics, compared to CRP, WCC, and body temperature, during acute appendicitis based on analyses of more than 300 treated patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.