
Abstract
Abstract
Background:
We conducted a study to assess the diagnostic accuracy of the C-reactive protein (CRP) assay for periprosthetic joint infection (PJI).
Methods:
For the purpose of the study, we conducted a search of PubMed, selecting only studies that described the diagnosis of PJI through measurement of the serum CRP concentration. The results were meta-analyzed by pooling estimates of sensitivity, specificity, positive likelihood ratio (LR+), negative likelihood ratio (LR−), and diagnostic odds ratio (DOR) and constructing respective summary receiver-operating characteristic (SROC) curves. We also conducted subgroup analyses according to cutoff values of the serum CTP concentration.
Results:
A total of 25 studies met the selection criteria for inclusion in the analysis. The pooled estimates for sensitivity, specificity, and the area under the curve (AUC) for the CRP assay were 0.82 (95% CI 0.80–0.84), 0.77 (95% CI 0.76–0.78), and 0.877±0.016, respectively. In the 10 mg/L cutoff subgroup, the pooled estimates for sensitivity, specificity, and the AUC were 0.881 (95% CI 0.859–0.901), 0.728 (95% CI 0.706–0.749), and 0.8496±0.0248, respectively.
Conclusion:
We found that the serum CRP assay had good diagnostic accuracy for PJI but that its specificity was low. We recommend that when the CRP assay yields a normal result, other tools be used adjunctively with it to reduce the rate of false-negative diagnoses of PJI.
T
Traditionally, microbiologic examination of tissue or fluid samples obtained from an affected prosthetic joint during revision surgery have been considered the gold standard for PJI. However, the diagnosis of PJI in the pre-operative period can be particularly difficult. Some researchers have used the results of culture of joint fluid aspirates for the pre-operative diagnosis of PJI. In the aspiration of joint fluid for microbiologic investigation, correct needle placement must be confirmed, especially in patients who are obese or those with acetabular protrusions or periarticular ossifications. However, Müller et al. reported that the culture of joint aspirates in patients with TJAs without removal of the prosthesis yielded false-negative results in 28% [5]. C-reactive protein (CRP) is an acute-phase serum protein whose concentrations increase in response to inflammation. A meta-analysis has already shown good accuracy for measurement of the serum concentration of CRP in the diagnosis of bacterial infections in hospitalized patients, with a sensitivity of 75% (95% CI 62%–84%) and specificity of 67% (95% CI 56%–77%) [6]. The serum CRP assay is also used widely in the diagnosis of PJI, but its diagnostic accuracy has varied across studies. Dupont et al. reported that the CRP assay had a sensitivity of 58.3% and specificity of 100% at a threshold CRP concentration of 25 mg/L; at a threshold of 18 mg/L the sensitivity and specificity of the assay were 66.7% and 88.9%, respectively [7]. Johnson reported a sensitivity of 95% and specificity of 20% for the CRP assay in PJI [8]. To evaluate adequately the diagnostic accuracy of the CRP assay for PJI, we systematically reviewed and conducted a meta-analysis of studies that investigated serum CRP concentrations as markers for PJI.
Methods
Search strategy
We attempted to identify studies of the diagnostic accuracy of the serum CRP assay for PJI that were published in the PubMed database before February 2013. The terms used in our search of PubMed were: C-Reactive Protein [title/abstract] OR CRP [title/abstract]) AND (periprosthetic [title/abstract] OR arthroplasty [title/abstract] OR replacement [title/abstract]) AND infection* [title/abstract] AND (“Sensitivity and Specificity” [MeSH Terms] OR specificity*[tw] OR accuracy [tw] OR predictive value*[tw] OR ROC[tw] OR likelihood ratio*[tw]). We supplemented our searches by reviewing manually the references of all relevant studies. No language restrictions were applied in these searches.
Inclusion and exclusion criteria
We included all studies that met the criteria of: (1) Assessing the diagnostic accuracy of the CRP assay for PJI; (2) comparing the diagnostic accuracy of the serum CRP assay with a reference standard (gold standard); and (3) providing true-negative (TN), false-positive (FP), true-positive (TP), and false-negative (FN) results, based on the data presented in the study, so that the sensitivity, specificity, positive likelihood ratio (LR+), negative likelihood ratio (LR–), and diagnostic odds ratio (DOR) could be calculated. Two reviewers judged independently the eligibility of studies for inclusion in the meta-analysis while screening the citations of the studies in PubMed. Disagreements of the reviewers were resolved by a third reviewer.
Data extraction and quality assessment
In our search of the PubMed database, we used a standard form to extract data on the first author of a study, its year of publication, the country in which the study was done, the study design, the diagnostic gold standard used in the study, the study population and number of patients, the patients' genders and ages, the prevalence of PJI, and the cutoff value used for the concentration of CPR. We also recorded the number of TN, FP, TP, and FN results, allowing us to construct two-by-two tables. We used the Quality Assessment of Diagnostic Accuracy Studies (QUADAS) tool to assess the quality of our investigations of predictive validity. Each item of the QUADAS tool was answered with a reply of “Yes,” “No,” or “Unclear” [9]. Two reviewers assessed independently the quality of the studies brought up in the search. Disagreements of the reviewers were resolved by a third reviewer.
Statistical analysis
The overall pooled values for sensitivity, specificity, and diagnostic odds ratio (DOR) for PJI of the serum CRP concentration in the studies used in the meta-analysis, with 95% confidence intervals (CIs), were estimated with DerSimonian and Laird's random-effects model [10]. In addition, summary receiver-operating characteristic (SROC) analysis was done to examine the interaction between sensitivity and specificity [11] and to quantify the performance of the CRP assay using the AUC and Q* value [12]. The heterogeneity of the studies used in the meta-analysis was assessed with the Cochran Q test and the I2 statistic. A value of p<0.05 with the Cochran Q test indicated significant heterogeneity; A value of I2 >50% indicated substantial heterogeneity. We conducted threshold analyses using the Spearman rank correlation test for Logit(TPR) and Logit(1–TNP). Subgroup analyses were conducted on the basis of cutoff values of CRP. All analyses were done with Meta DiSc 1.4 software version 0.6 [13] (http://www.hrc.es/investigacion.metadisc.en.htm).
Results
Eligible studies
Our initial search yielded 72 citations, of which 31 were excluded after screening of the abstracts and titles. We retrieved 41 studies for full-text reading, of which 20 met our inclusion criteria. Another five studies were added after a manual review of relevant studies. Ultimately, 25 study papers [5,7–8,14–35] were included for analysis. The flow diagram showing the process of selection of the studies is shown in the Supplementary material (www.liebertpub.com/sur). The 25 included studies were conducted in nine countries between 1989 and 2013, and included 4,088 patients. Twelve of the studies used an appropriate prospective cohort-study design and seven studies used a retrospective cohort or case–control design. All of the studies included in the meta-analysis used clinical criteria to define PJI. The populations of the studies consisted largely of patients undergoing total hip arthroplasty (THA) or TKA. The cutoff value of the serum CRP concentration varied from 0.06–500 mg/L, although a value of 10 mg/L was used in most studies. The details of all 25 studies included in the meta-analysis are shown in Table 1.
CRP=C-reactive protein; ESR=erythrocyte sedimentation rate; NR=not reported; PMN=polymorphonuclear netrophils; THA=total hip arthroplasty; WBC=white blood cell count.
The quality of the included studies was modest. Four studies did not provide a sufficient spectrum of patients for testing and four other studies did not provide a reference standard for the diagnosis of PJI. Moreover, none of the studies included in the meta-analysis reported uninterpretable or indeterminate results, and none provided information about patient withdrawal or dropout. A graph and summary of the methodologic quality of the studies is shown in the appendix.
Main meta-analysis
The performance of the serum CRP assay for the diagnosis of PJI in the 25 studies included in the meta-analysis is presented in Table 2. The sensitivities of the CRP assay varied from 0.421–1.000 (a range of 0.579) and its specificities varied from 0.204–1.000 (a range of 0.796). The LR+varied from 1.163–42.692 (a range of 41.529) and the LR– varied from 0.033–0.686 (a range of 0.653). The overall pooled sensitivity of the CRP assay for PJI was 0.817 (95% CI 0.798–0.836; χ2 (34)=238.11, p=0.000; I2=85.7%). The overall specificity of the CRP assay for PJI was 0.771(95% CI 0.757–0.784; χ2(34)=362.54, p=0.000; I2=90.6%). The combined LR+and LR− were 3.659 (95% CI 2.917–4.591; χ2(34)=347.56, p=0.000; I2=90.2%) and 0.262 (95% CI 0.205–0.334; χ2(34)=167.52, p=0.000; I2=79.7%), respectively, yielding a DOR of 17.012 (95% CI 11.378–25.435; χ2 (34)=145.14, p=0.000; I2=76.6%). There was a threshold effect between the studies (r=0.339; p=0.047). The overall weighted AUC of the SROC curve was 0.8736±0.0158, and the overall diagnostic accuracy (Q*) was 0.8040±0.0158. The forest plots for the pooled sensitivity, specificity, LR+, LR−, and DOR are shown in the Appendix, and the SROC curve is shown in Figure 1.

Plot of summary receiver-operating curve for serum C-reactive protein in the diagnosis of periprosthetic joint infection in studies included in the meta-analysis.
CI=confidence interval; FN=false negative; FP=false positive; LR–=negative likelihood ratio; LR+= positive likelihood ratio; NR=not reported; Sen=sensitivity; Spe=specificity; TN=true negative; TP=true positive.
Subgroup analyses
A total of 14 studies provided a CPR cutoff value of 10 mg/L. In this 10 mg/L cutoff subgroup, the overall pooled sensitivity for PJI was 0.881 (95% CI 0.859–0.901; χ2(16)=115.66, p=0.000; I2=86.2%) and the overall specificity was 0.728 (95% CI 0.706, 0.749; χ2(16)=122.90, p=0.000; I2=87.0%). There was a threshold effect among the studies (r=0.505; p=0.039). The overall weighted AUC of the SROC curve was 0.8496±0.0248, and the overall Q* was 0.7809±0.0234. The forest plots for the pooled sensitivity, specificity, LR+, LR−, and DOR are shown in the Appendix and the SROC curve is shown in Figure 2.
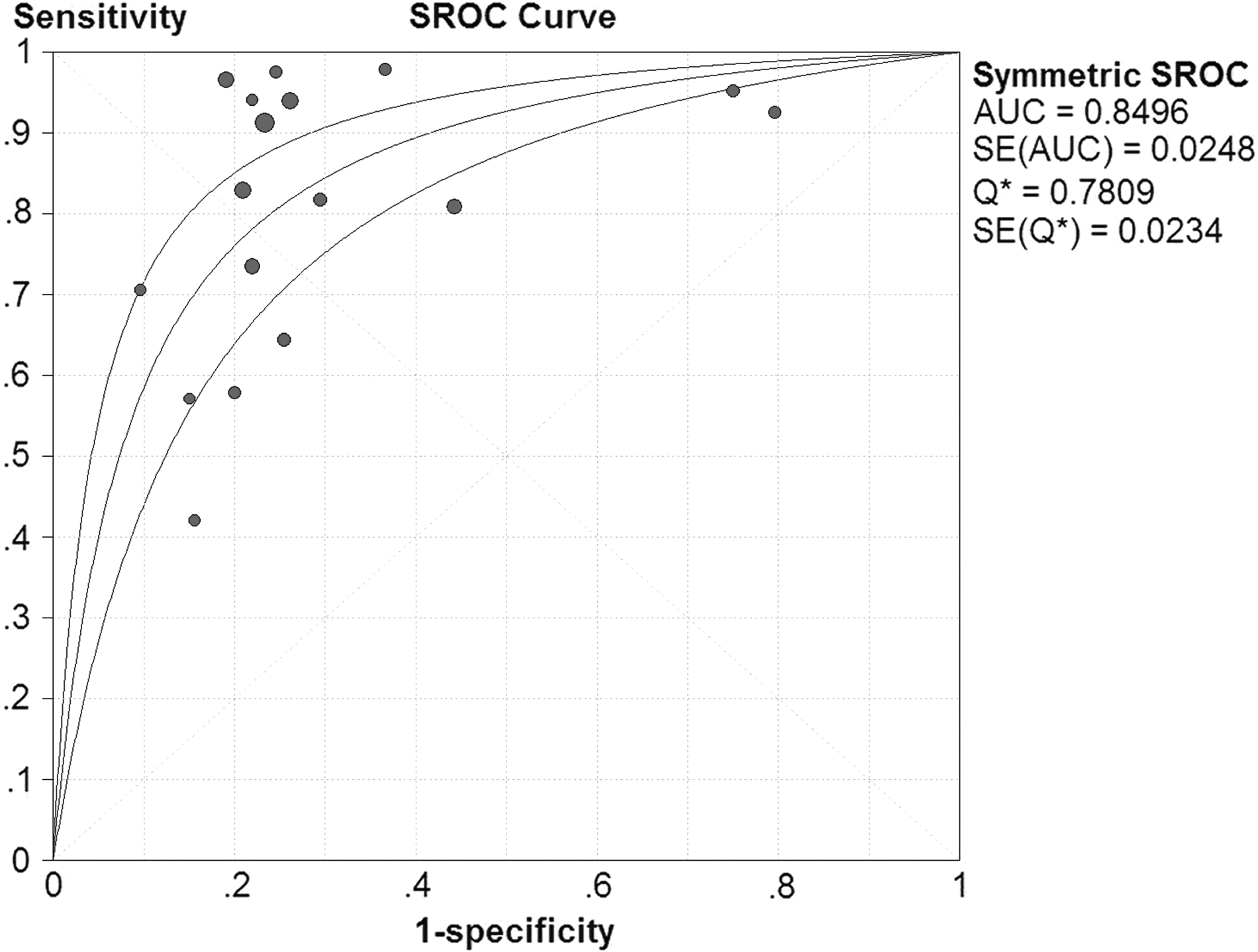
Plot of summary receiver-operating curve for serum C-reactive protein in diagnosing periprosthetic joint infection in the 10 mg/L cutoff subgroup.
Discussion
In 2011, the workgroup of the Musculoskeletal Infection Society (MSIS) proposed a new definition for PJI, specifying that: (1) It must exhibit a sinus tract communicating with the prosthesis; or (2) a pathogen isolated by culture from two separate tissue or fluid samples from the affected joint; or (3) the existence of four of the following six criteria: (a) An elevated erythrocyte sedimentation rate (ESR) and CRP concentration; (2) an elevated synovial leukocyte count; (3) an elevated percentage of synovial neutrophils; (4) purulence in the affected joint; (5) isolation of a microorganism; or (6) greater than five neutrophils per high-power field in five high-power fields observed from histologic analysis of periprosthetic tissue at X400 magnification [36]. The American Academy of Orthopedic Surgeons (AAOS) recommended strongly in 2010 that CRP testing be done for patients being assessed for PJI [37]. The importance of the serum CRP assay has been well accepted for the diagnosis of PJI. Our investigation assessed the accuracy of the serum CRP assay when used alone for the diagnosis of PJI. Pooled data from the 25 studies included in our meta-analysis yielded an overall weighted AUC for the SROC curve of 0.8736±0.0158. An AUC of 0.5 indicates that a test has no discriminatory ability, whereas an AUC of 1.0 indicates perfect diagnostic capability [38]. Although the AUC should be in the region of 0.97 or greater to demonstrate excellent accuracy, an AUC of 0.93 to 0.96 is very good and an AUC of 0.75 to 0.92 is good, but an AUC of less than 0.75 indicates obvious deficiencies in the diagnostic accuracy of an assay [39]. The overall AUC and 95% CI for SROC curve were 0.8736 and 0.8426–0.9046, respectively. This result showed that the diagnostic accuracy of the serum CRP assay for PJI was good. The overall diagnostic accuracy (Q*) of the assay was 0.8040±0.0158, with a 95% CI of 0.7730–0.8450, which also indicated good diagnostic accuracy.
We also found that the overall pooled sensitivity of the serum CRP assay for PJI was 0.817 (95% CI 0.798–0.836) and that its overall pooled specificity was 0.771 (95% CI 0.757–0.784). The sensitivity of a diagnostic test, also called the true positive rate, measures the proportion of truly positive results that are correctly identified as such (in the present context, the percentage of patients with PJIs who are correctly identified as having PJIs), whereas the specificity of a test, also called the true negative rate, measures the proportion of truly negative results of the test that are correctly identified as such (the percentage of people without a PJI who are correctly identified as not having a PJI). In the meta-analysis done in our study, the overall pooled specificity of the CAP assay was low. This means there were many patients with true PJIs for whom the CRP assay yielded normal results. The reason for this may have been that some patients failed to mount a sufficient immune response to the pathogen responsible for their PJI. In a prospective cohort study, Johnson et al. reported that the serum CRP assay had a specificity of only 20% (95% CI 6%–50%) at a cutoff value of 10 mg/L [8]. Therefore, when the serum CRP concentration is normal, additional means for making a diagnosis of PJI should be used adjunctively to reduce the rate of false-negative results.
We also did subgroup analyses as part of the present study. Because a CRP cutoff value of 10 mg/L was used in most of the studies, we analyzed the subgroup for which this cutoff value was used. The overall weighted AUC of the SROC curve in this analysis was 0.8496±0.0248, and the overall Q* was 0.7809±0.0234; the overall pooled sensitivity was 0.881 (95% CI 0.859–0.901) and the overall specificity was 0.728 (95% CI 0.706–0.749). The diagnostic accuracy of the CRP assay for PJI was also good, but the specificity was low, as it had been in the original meta-analysis. We were unable to conduct subgroup analyses for THA or TKA subgroups because of insufficient data. The serum CRP assay may have different diagnostic accuracies for THA and TKA. Piper et al., using the 10 mg/L cutoff value for CRP, reported a sensitivity of 83% for the CRP assay in the TKA subgroup as compared with a sensitivity of 74% in the THA subgroup. The specificity with a 14.5 mg/L may be the best cutoff in the TKA subgroup; and 10.3 mg/L was the best cutoff in the THA subgroup. With an optimized CRP cutoff value, the sensitivity of the assay was 79% in the TKA subgroup vs. 88% in the THA subgroup, and the specificity was 79% in the TKA subgroup as compared with 78% in the THA subgroup [17]. Some prospective cohort studies remain necessary for comparing the diagnostic accuracy of the serum CRP assay for PJI in the subgroups of patients with TKA and THA.
Our meta-analysis has some limitations. First, there is currently no agreement about a gold standard for the diagnosis of PJI. Different reference standards were used in the studies included in the meta-analysis, and four studies did not report a reference standard. Second, most of the studies included in the meta-analysis enrolled patients because of suspected PJI. The incidence of PJI ranged from 11.6%–92.9%, which was higher than the 1% incidence of PJI in all patients who had total joint arthroplasty in the studies included in the meta-analysis. The different reference standards and higher incidence of PJI also lead to bias in assessing the diagnostic accuracy of the CRP assay. Third, there was an obvious threshold effect in the meta-analyses. These limitations need to be borne in mind when evaluating the conclusions that can be drawn from the results of the present study.
In conclusion, our meta-analysis indicates that the serum CRP assay for PJI has good diagnostic accuracy but a low specificity. We recommend that a normal result of the serum CTP assay be accompanied by adjunctive other diagnostic methods for reducing the rate of false-negative results.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.