
Abstract
Abstract
Background:
Total parenteral nutrition (TPN) via central venous catheters has improved nutrient delivery to patients unable to receive nutrition enterally, but its administration can be complicated by bacteremia and fungemia.
Methods:
At a large tertiary-care academic medical center, 245 patients with concurrent positive blood cultures, among 1,716 adult patients who received TPN over a period of three consecutive years, were divided into those in whom parenteral nutrition was continued and those in whom it was stopped after the occurrence of a positive blood culture. To determine whether continuation of TPN after a positive blood culture was associated with a statistically significantly longer hospitalization than with its discontinuation after a positive blood culture, we performed a logistic regression analysis with step-wise selection, with parenteral nutrition status as the dependent variable and type of venous access, type of pathogen responsible for a positive blood culture, recurrence of a positive blood culture, respiratory failure, shock, and length of stay as covariates.
Results:
The prevalence of positive blood cultures was 14% among all hospitalized patients given parenteral nutrition. Parenteral nutrition was continued in 60% of the patients. Baseline co-morbid and laboratory parameters were comparable in the group of patients in whom TPN was continued and the group in which it was stopped except that the white blood cell count (WBC) was lower in the former group (9.1±6.6 mm3 vs. 12±12.1 mm3, p=0.015). Both groups received an average of 30 kcal/kg and 1.4 g protein/kg via TPN. There was no difference in the two groups in total calories, lipids, protein, or glutamine-base received before the occurrence of a positive blood culture (p=0.86, p=0.51, p=0.79, and p=0.42, respectively). The hospital stay of the group in which TPN was continued after a positive blood culture was statistically significantly longer than that of the group in which it was discontinued (44.6±32.3 d vs. 28.2±18.5 d, p<0.001). This difference remained significant in the multivariable logistic regression analysis.
Conclusion:
Continuation of TPN after a positive blood culture was associated with statistically significantly longer hospitalization before and after adjustment for co-morbid conditions.
M
Although previous studies have established the adverse outcomes of malnutrition and bacteremia individually, as well as the consequences of TPN with conjoint bacteremia [8,9], none has addressed the management of TPN after a positive BC. The study reported here provides data about the consequences of the continuation or discontinuation of TPN in the highly vulnerable subset of malnourished, acutely ill patients consisting of patients with positive BCs concurrent with TPN.
Patients and Methods
All patients ≥18 y of age who were admitted to the Brigham and Women's Hospital from January 1, 2007 through December 31, 2009 were potentially eligible for the study, which was a retrospective, closed-cohort study approved by the hospital's institutional review board. The study was restricted to those patients with a positive BC for bacteria or fungi after the initiation of TPN and before hospital discharge, who were identified from microbiologic and pharmacy data. Peripheral parenteral nutrition is not administered at our hospital. Patients who met the inclusion criteria for the study were divided into those in whom TPN was continued (TPN-c) and those in whom TPN was discontinued (TPN-dc). Continued TPN (TPN-c) was defined as the administration of TPN at any time beyond 48 h after a positive BC, and TPN-dc was defined as the discontinuation of TPN within 48 h after a positive BC and for the remainder of the patient's hospitalization. It typically takes 48 h for a BC reading to be completed by our laboratory.
Exposures
Exposure to TPN was measured in terms of total and lipid doses in kilocalories and of protein in grams, as well as by the total number of days of infusion (over the entire period of hospitalization, from before a positive BC to after a positive BC). Because of its influence on infection [10], TPN containing glutamine was noted. The pathogen (gram-positive bacterium, gram-negative bacterium, Candida species) responsible for the positive BC was noted. A recurrence of blood stream infection was determined by evaluating microbiologic data subsequent to a patient's first positive BC; a subsequent positive BC was considered a recurrence if the organism found in a first positive BC was cultured after at least 72 h or a different organism was cultured at any time after a first positive BC. Only a first recurrence of an initially positive BC was recorded.
Co-variates
Medical records were reviewed to determine patients' demographic data at the time of admission, including age and sex. Parameters of malnutrition at admission were assessed, including body mass index (BMI), albumin, and classification (at risk for malnutrition, degrees of protein–calorie malnutrition, or marasmus). Information was collected on pre-existing and acquired co-morbidities, including diabetes mellitus, respiratory failure, chronic kidney disease, and shock, as well as on incident surgery. Surgical procedures were classified anatomically as intracranial, cardiothoracic, or abdominal. Laboratory values were noted for white blood cell (WBC) count, hemoglobin, and glucose at the time of admission. Glucose was generally maintained ≤180 mg/dL during hospitalization between the years of 2007 and 2009 [11,12]. Information was also collected about patients' creatinine, aspartate aminotransferase and alanine aminotransferase concentrations at the initiation of TPN. Addditionally, the type of CVC used for delivering TPN, whether central or peripheral (peripherally inserted central catheter [PICC]), was recorded, and if a central catheter was used, determination was made of whether it was tunneled or non-tunneled at the time of a first positive BC, by reviewing chest radiographs.
Statistical analysis
Statistical analyses were done with SAS version 9.3 (SAS Institute, Cary, NC). A non-parametric method (the Mann–Whitney U test) was used for continuous variables and the χ2 test was used for categorical variables, with the two types of variables reported as mean±standard deviation (SD) and percentage, respectively. Univariate analysis was done for known co-variates. Logistic regression analysis with step-wise selection was done with TPN status as the dependent variable and type of catheter access, type of pathogen, recurrence of a positive BC, respiratory failure, presence of shock, and LOS as co-variates. Specifically, we began with a saturated model that had TPN status as the dependent variable and respiratory failure, presence of shock, type of catheter access, type of pathogen, recurrence of a positive blood culture, and LOS as co-variates, according to the results of univariate analyses and clinical objectives. A model reduction was then done through step-wise selection to assess the overall fit for the multi-variable logistic regression models. There was no evidence of lack of fit in the reduced model (Hosmer–Lemeshow test, p=0.82). Further analysis was also done by propensity score. Odds ratios (OR) and their 95% confidence intervals (CI) were reported for both the full model and the reduced model, with the 95% CI excluding 1. A two-tailed value of p<0.05 was considered statistically significant.
Results
Prevalence and demographics
The number of admissions over the three years of the study was 137,212. Of the 1,716 (1%) patients who received TPN, 245 (14%) developed a positive BC. Of these 345 patients, 146 (60%) were in the TPN-c group and 99 were in the TPN-dc group. Baseline characteristics of the two groups are shown in Table 1. The demographics, co-morbid conditions, surgical status, and baseline laboratory parameters of the two groups were comparable except for admission WBC count, which was lower in the TPN-c group (9.1±6.6 vs. 12±12.1 mm3, respectively; p=0.015).
BMI=body mass index; TPN-c=total parenteral nutrition continued; TPN-dc=total parenteral nutrition discontinued.
Nutritional and microbiologic characteristics
The TPN-d and TPN-dc groups showed no differences in total calories, lipid, protein, or total dosage of glutamine base received before the occurrence of a positive BC (p=0.86, p=0.51, p=0.79, and p=0.42, respectively) (Table 2). Both groups received an average of 30 kcal/kg and 1.4 g protein/kg. As expected, total calories, lipid, and protein received after a positive BC were significantly greater in the TPN-c than in the TPN-dc group (p<0.001). The characteristics of the pathogens identified on BC also did not differ in the two groups (p=0.11). However, a statistically significant difference in the two groups was found in the type of CVC for TPN access at the time of a first positive BC (p<0.001), with patients in the TPN-dc group being more likely to have had a PICC for TPN access than those in the TPN-c group (70% vs. 42%, respectively).
BC=blood culture; CVC=central venous catheter; PICC=peripherally-inserted central catheter; TPN-c=total parenteral nutrition continued; TPN-dc=total parenteral nutrition discontinued.
Outcomes
Tables 3 and 4 and Figure 1 show the outcomes in the TPN-c and TPN-dc groups in the study. The principal findings were a significantly longer LOS (44.6±32.3 d, p<0.001) and significantly greater number of patients with recurrent bacteremia (n=53 [36%], p=0.007) in the TPN-c than in the TPN-dc group. The median (minimum, maximum) values for LOS were 36 d (95% CI 4,223) and 25 d (95% CI 2,136) for the TPN-c and TPN-dc groups, respectively. By univariate analysis done with the Mann–Whitney U test, the OR for the difference in LOS remained statistically significant after adjustment for other confounders (Table 4). Odds ratios for continuous variables may be close to 1 and yet be significant. There was no difference in mortality in the TPN-c and TPN-dc groups.
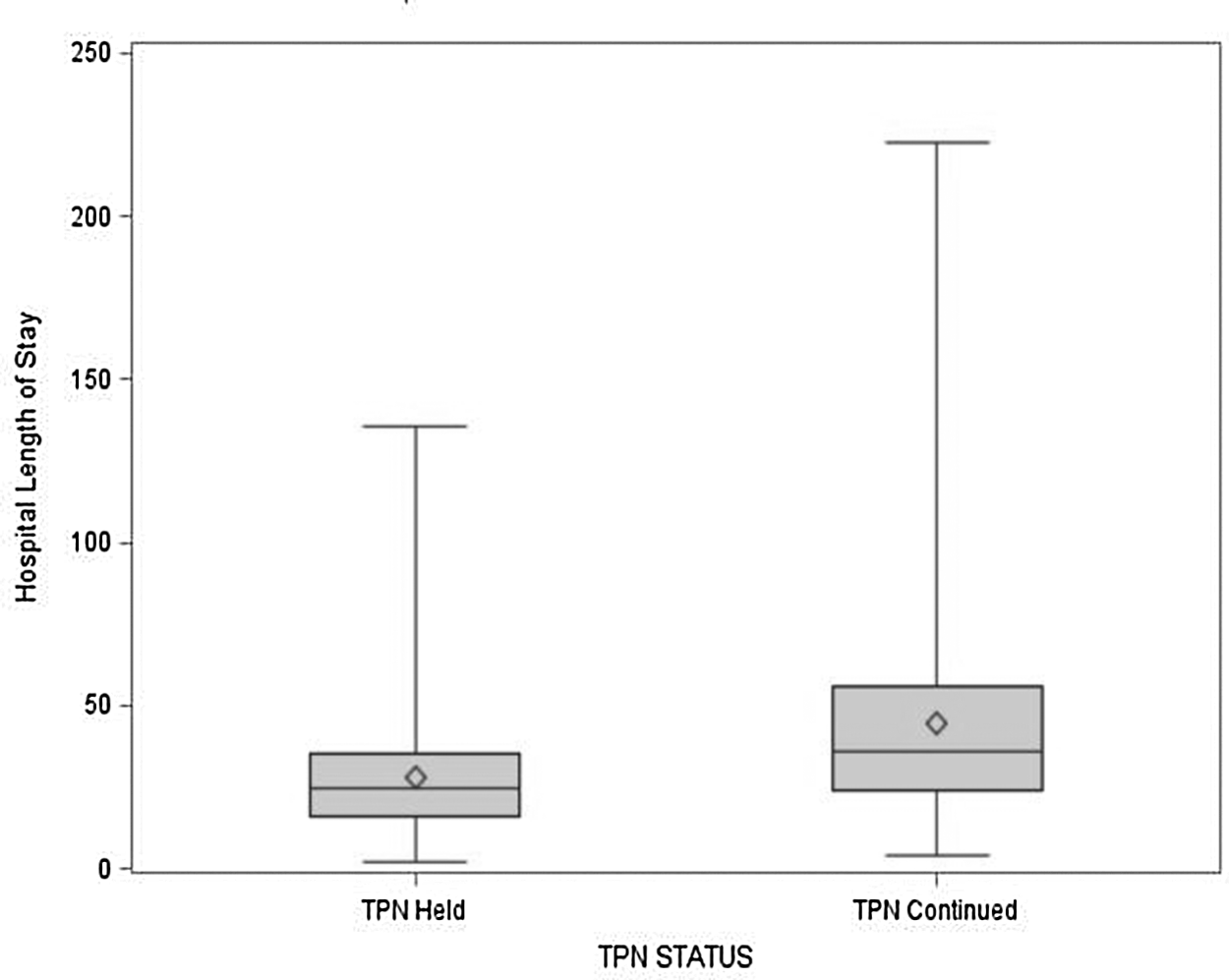
Box plot demonstrating significantly longer hospital length of stay (in days) of patient in whom total parenteral nutrition (TPN) was continued than in those in whom it was discontinued.
Total parentral nutrition (TPN) continued status was the dependent variable, and access type, pathogen type, positive blood culture recurrence, respiratory failure, presence of shock, and length of stay were covariates based on univariate analysis. The regression model shows a statistically significantly longer hospital length of stay and TPN access type in patients in whom TPN was continued.
TPN=total parenteral nutrition.
Then model reduction (step-wise selection) was performed to assess the overall fit for the multivariate logistic regression model. Hospital length of stay as well as total parenteral nutrition (TPN) and blood culture recurrence was significantly higher in patients with TPN continued.
Additionally, to determine the effect of TPN status on LOS, we created a propensity score by estimating a logistic regression using age, access type, pathogen type, respiratory failure, positive BC recurrence, and shock to address potential selection bias. A propensity score-weighted regression model was then fitted to compare LOS between the TPN-c and TPN-dc. After the adjustment, the TPN-c still had a much longer LOS (p=0.0003) (Fig. 2).
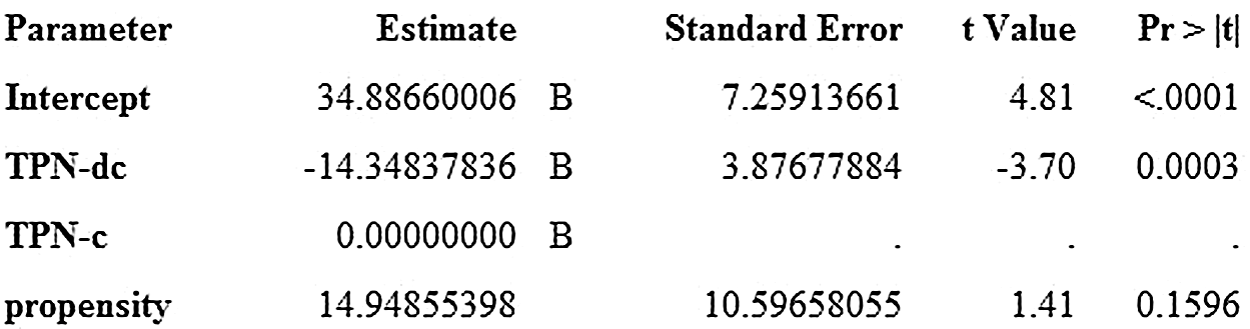
Propensity model output showing statistically significantly longer hospital length of stay for patients in whom total parenteral nutrition was discontinued (TPN-c) than for those in whom it was discontinued (TPN-dc).
Discussion
The present study reports previously unreported findings of adverse outcome associated with the use of TPN after a positive BC irrespective of its cause. In patients receiving TPN with a concurrently positive BC, the continuation of TPN was associated with a statistically significant increase in LOS. This finding remained statistically significant after adjustment for various factors. No significant difference was seen in the LOS before development of a positive BC in patients who did and those who did not subsequently develop a positive BC.
The incidence of positive BC associated with TPN in our study was 14%. This was slightly lower than reported elsewhere [13]. Although the patients in the two cohorts in our study were not randomized to ensure homogeneity of the cohorts, they were remarkably similar in nearly all respects. They did not differ in baseline demographic features, including age and sex, nor did they differ in terms of nutrition status (BMI, serum albumin). Medical and surgical conditions were equally distributed in the two groups, making even more notable the finding that TPN status alone during the occurrence of blood stream infection was associated with an increased hospital LOS. The reasons for a possible prolongation of hospitalization with the continuation of TPN during septicemia are myriad, and may include but are not limited to distant infections and metabolic dyscrasia. The retrospective design of the present study, which generated this hypothesis, makes it possible only to confirm the association, and not the causality, of the observed difference in LOS the TPN-c and TPN-dc groups in the study. Discontinuation of TPN was not associated with increased mortality, suggesting that either the resultant parenteral caloric deficit was not important in altering the endpoint of LOS or that patients in whom TPN was discontinued could be successfully transitioned to an enteral mode of nutritional support. If the latter was the case, it is arguable that TPN might have been replaced by enteral feeding sooner than it was in those patients in whom this transition was made. The unintended benefit of a positive BC seems to be the prompting of the medical treatment team to consider alternative strategies of nutritional support earlier than might otherwise have been the case, and further research is needed to explore the components of the process by which this decision is reached.
In our study, glutamine-base TPN did not influence outcome, but this has to be interpreted within the context of the study design [14]. This is surprising given previous studies in which the intravenous administration of L-alanyl-L-glutamine was associated with a reduced rate of infectious complications as well as reduced ICU mortality [15,16]. As expected, patients who continued to receive TPN received significantly more total calories and protein during their hospitalization. However, and in contrast to the finding in other studies, caloric intake before the incidence of a positive BC was no different in the patients in our TPN-d and TPN-dc groups, suggesting that caloric burden alone does not explain the differences in LOS in the two groups [17].
Additionally, studies have shown that catheter type and site may influence the risk of bacteremia in patients receiving TPN [18]. Our study supports the evidence that the type of a CVC (tunneled CVC, non-tunneled CVC, PICC) carried differing risks of infection in the study cohort that had TPN-c [19]. We also observed that patients in whom TPN was discontinued after the development of a blood stream infection were more likely to have a PICC as access for their TPN. It can be argued that the ease with which the access through a PICC can be discontinued (PICCs do not have cuffs that need to be dissected free, nor do they require surgical intervention for the extraction of an implanted reservoir) may be a greater determinant of whether TPN is continued or discontinued rather than the patient's nutritional risk. We would recommend caution to medical teams in deciding to continue or discontinue nutritional support solely on the basis of ease of venous access. Certainly our data suggest that discontinuing TPN after an incident BSI reduces LOS without any attendant increase in morbidity or mortality, but that decision might better be made on the merits of the continued provision of nutrition rather than ease of catheter access for TPN. With increasing literature showing a narrowing of the cohort of patients who benefit from TPN, our study suggests that there is a subset of patients with blood stream infections who do not benefit from continuing TPN beyond the development of such infections. It does not appear that withholding TPN after a positive BC harmed the patients in our TPN-dc group, as evidenced by the lack of a difference in mortality in the TPN-dc and TPN-c groups. However, it is important to note that our study was not powered to detect significant differences in mortality in the two groups.
A major advantage of this study is that it preserves the sequence of events in terms of the timing of administration of TPN in relation to incident and recurrent positive BC, LOS, and death. Another advantage of the study, based on its design, is its avoidance of the ethical dilemma posed by an interventional clinical trial that might randomize some malnourished patients with an absolute contraindication to any type of nutritional support other than parenteral nutrition to receive minimal or no nutritional support. Other advantages of the study include its relatively large sample size and robust statistical analysis.
Despite the existence of an electronic medical and drug ordering record at our institution, potentially incomplete record keeping of actual medication administration in the large patients cohort of the study made it nearly impossible to quantitate other, competing sources of nutrition, including carbohydrate (e.g., dextrose-containing intravenous fluids), lipid (e.g., sedative drips containing propofol), or enteral sources of calories. Nevertheless, the purpose of the study was not to investigate the risks as opposed to the benefits of TPN in all patients, or the management of catheter-related blood stream infection, but rather to describe medical practice decisions with regard to the continuation of TPN as opposed to its dicontinuation in the very specific setting of a concurrently positive BC. Interestingly, a study published in this journal reported that delaying lipid-emulsion TPN was not associated with a reduced incidence of infection [20]. Our finding in the present, larger study is consistent with that finding. Calculation of the rate of recurrence of a positive BC was limited by the lack of a repeat BC after the incident positive BC in some patients.
Lastly, we utilized a multivariable regression model with propensity scoring to address the inherent vulnerability of our retrospective study design to confounding by indication. That is, because the allocation of treatment (from the decision to initiate TPN to the decision to either continue or discontinue it after a positive BC) was not randomized, and the indication for treatment (malnutrition and sepsis) may be related to the risk of health outcome (worsening malnutrition or septic shock and death), the resulting imbalance in the underlying risk profile of the treated and comparison groups may generate biased results.
In summary, we report a significantly increased LOS associated with the continuation of TPN in patients with a concurrent positive BC. Larger prospective studies are needed to confirm that the failure to discontinue TPN after a positive BC, particularly after meticulous catheter management, adversely affects LOS.
Footnotes
Acknowledgment
We thank the Surgical ICU (STAR) Research Center for its statistical support.
Author Disclosure Statement
No competing financial interests exist.