
Abstract
Abstract
Background:
Clostridium difficile (CD) is a common cause of healthcare-associated infectious colitis that complicates about 1% of all hospital stays in the U.S. The impact of CD on outcomes after coronary artery bypass grafting (CABG) and valvular surgery (VS) is not well known.
Methods:
The Nationwide Inpatient Sample (2002–2009) was queried to identify CABG and VS patients utilizing International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes. Rates of CD, post-operative endocarditis and mediastinitis, hospital mortality rate, and resource utilization were evaluated.
Results:
We identified 421,294 and 90,923 patients of age 40 yrs and older who underwent CABG and VS, respectively. The CD infection was more likely to develop in patients undergoing VS than in those having CABG (odds ratio [OR] 1.8; 95% confidence interval [CI] 1.64–1.92) and was more likely after urgent or emergency admission than after elective admission (OR 1.8; 95% CI 1.68–1.94). There was a greater likelihood of mediastinitis in patients with CD after CABG than in non-complicated cases without CD, both by univariable (OR 6.0; 95% CI 3.07–11.62) and multivariable analysis with adjustment for patient age, gender, race, type of admission, and co-morbidities (OR 3.1; 95% CI 1.49–6.51). The infection thus was most likely a result of the antibiotics used to treat mediastinitis, as the patients treated for mediastinitis were most likely to develop CD. There was a significant association in patients with CD and endocarditis who underwent VS but not in patients who did not have CD. The CD infection in these patients thus was most likely a result of the antibiotics used to treat endocarditis. Endocarditis and CD developed 3.2 times (95% CI 2.65–3.97) as often as in patients without CD, a finding that was confirmed by multivariable analysis (OR 2.2; 95% CI 1.70–2.84). At the same time, in patients having VS, there was no significant association of CD and mediastinitis. Clostridium difficile infection affected the hospital mortality rate significantly after both CABG (OR 2.0; 95% CI 1.65–2.35) and VS (OR 1.9; 95% CI 1.51–2.39). Development of CD increased median hospital length of stay and cost dramatically after both CABG (from 7 d to 19 d and from $33,105 to $65,535, respectively; p<0.0001 for both) and VS (from 8 d to 24 d and from $41,876 to $95,699, respectively; p<0.0001 for both).
Conclusions:
The development of CD worsened significantly the outcomes of adult patients undergoing cardiac surgery. There was a greater risk of CD in patients with either mediastinitis or endocarditis. The infection was associated with a higher hospital mortality rate, longer hospital stays, and greater cost after both CABG and VS.
C
The rise in the prevalence of CD colonization in hospitalized patients may have consequences for patients who undergo surgery [3]. The actual effects of CD on adult patients who undergo cardiac surgery are not well known. Currently, the reported incidence of CD-associated diarrhea is 0.2% to 8.4% depending on the surgical population [4,5]. Clostridium difficile has the potential to increase operative mortality and morbidity rates. Furthermore, the presence of infection outside the gastrointestinal tract may be associated with a higher incidence of CD. For example, long-term treatment with antibiotics for mediastinitis or endocarditis may make patients susceptible to CD infection (CDI). The purpose of our study was to determine the association between CDI and outcomes in adults who undergo cardiac surgery. The primary endpoints were in-hospital death and hospital resource utilization: Length of stay (LOS) and cost. The secondary endpoints were identifying any association between post-operative mediastinitis or endocarditis and CDI.
Patients and Methods
Data source
The Nationwide Inpatient Sample (NIS) from the years 2002–2009 was used for this study. This is the largest all-payor database in the U.S. and was developed as part of the Agency for Healthcare Research and Quality (AHRQ) Healthcare Cost and Utilization Project (HCUP). It includes information about 20% of all hospitalizations in approximately 1,000 non-federal short-term hospitals. The most recent NIS contains inpatient stay records from 45 states, accounting for more than 96% of the U.S. population. The sampling strategy of this database provides the opportunity to compute nationwide estimates. Detailed NIS documentation with the description of all data elements is available at www.hcup-us.ahrq.gov/db/nation/nis/nisdbdocumentation.jsp
Study population
All adult patients aged 40 yrs and older who underwent coronary artery bypass grafting (CABG) or valvular surgery (VS) were selected. To identify those with CABG, we used International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) procedure codes 36.1x, 36.2, and 36.3x for principal or any 14 secondary procedures in the database. The ICD-9-CM procedure codes 35.0x, 35.1x, 35.2x, 35.96, and 35.99 were used to recognize patients with VS. Clostridium difficile was detected with the diagnosis code 008.45 in any diagnosis position. The following codes for secondary diagnoses were employed to identify post-operative infectious complications: 480.x, 481, 482.x, 482.3x, 482.4x, 482.8x, 482.9, 483.x, 485, and 486 for pneumonia; 038.xx, 785.52, 995.91, 995.92, 996.61, 996.62, 998.0, 999.31, and 999.39 for sepsis and blood stream infection; 599.0 and 996.64 for urinary tract infection (UTI); 998.51 and 998.59 for surgical site infection (SSI); 421.0 for endocarditis; and 519.2 for mediastinitis. Co-morbidities in the study patients were evaluated with the AHRQ co-morbidity measures that are elements of the NIS data.
Statistical analysis
The study was approved by the Institutional Review Board of the University of Medicine and Dentistry of New Jersey–Robert Wood Johnson Medical School.
Data and all statistical analyses were performed with SAS 9.2 software (SAS Institute, Cary, NC). In-hospital death was defined as any-cause death during hospitalization and was calculated as a percentage for each group as the number of patients who died divided by the total number of patients in this group. To calculate hospital cost, we used the HCUP Cost-to-Charge Ratio Files that allow conversion of hospital charges in the database to actual hospital reimbursement. The difference between the two groups for categorical variables was tested by χ2 bivariable analysis by calculating the odds ratio (OR) and 95% confidence interval (CI). Controlling for confounding effects was performed with multivariable logistic regression analysis with adjustment for age, gender, race, co-morbidities, and other possible confounders. Because the numeric variables hospital length of stay (LOS) and cost were highly skewed to the right, we calculated the medians in various groups and compared inter-group differences using the non-parametric Wilcoxon rank sum test. A value of p<0.05 was considered statistically significant.
Results
We identified 421,294 and 90,923 patients aged 40 years and older who underwent CABG or VS, respectively (Table 1). Patients with VS were a little older than those with CABG (p<0.0001) with a greater proportion of octogenarians (p<0.0001). In both groups, males predominated over females, but this predomination was significantly greater among CABG patients (p<0.0001). There were some racial differences between the two surgical groups. Proportions of whites in both groups were similar, but in the VS group, there were relatively more blacks (p<0.0002) and fewer Hispanics (p=0.009) than in the CABG group. In the whole study group, patients who were hospitalized urgently or as an emergency were 1.8 times (95% CI 1.68–1.94) as likely to have CDI as were patients having elective admission. The patients who underwent CABG or VS and subsequently developed infections complications such as pneumonia (OR 6.5; 95% CI 6.00–7.10), UTI (OR 4.4; 95% CI 4.00–4.82), SSI (OR 5.8; 95% CI 5.00–6.76), sepsis (OR 8.6; 95% CI 7.89–9.35), endocarditis (OR 4.7; 95% CI 3.91–5.72), and mediastinitis (OR 5.1; 95% CI 2.78–9.25) (Fig. 1) were more likely to have CDI. The association between these additional infections and CDI most likely has to do with the prolonged use of antibiotics. The greater probability of the association between the additional infectious complications and CDI was confirmed by logistic regression analysis controlling for patient age, gender, race, co-morbidities, type of hospital admission, and surgical procedure (OR 5.1; 95% CI 4.68–5.59).

Association of Clostridium difficile infection and post-operative infections.
Percentages represent frequency distribution among patients for whom data were given.
CABG=coronary artery bypass graft; VS=valvular surgery.
Interestingly, the patients undergoing VS were more likely to have CDI than were those having CABG (OR 1.8; 95% CI 1.64–1.92). We analyzed the association between the presence of CDI and the presence of such heart-related infectious complications as mediastinitis and endocarditis separately for each surgical group. The likelihood of mediastinitis after CABG complicated by CDI was greater than in non-complicated cases both in bivariable χ2 (OR 6.0; 95% CI 3.07–11.62) and multivariable logistic regression analysis with adjustment for patient age, gender, race, type of admission, and co-morbidities (OR 3.1; 95% CI 1.49–6.51). After CABG, there was an association between mediastinitis and the presence of CDI that was not seen in the patients who did not have CDI. In other words, the patients who underwent CABG and were found to have mediastinitis also were more likely to have CDI. This is because the patients with mediastinitis were treated with antibiotics that ultimately contributed to the development of CDI. The association was seen both in bivariable χ2 (OR 6.0; 95% CI 3.07–11.62) and multivariable logistic regression analysis with adjustment for patient age, gender, race, type of admission, and co-morbidities (OR 3.1; 95% CI 1.49–6.51). The relation was not observed when patients had mediastinitis but not CDI.
We did not find a similar association with regard to endocarditis. However, this association was discovered after VS, where endocarditis developed in patients with CDI, being 3.2 times (96% CI 2.65–3.97) as likely as after cases without CDI, a finding that was confirmed by the multivariable analysis (OR 2.2; 95% CI 1.70–2.84). However, this association was discovered after VS, where patients were more likely to have both endocarditis and CDI, being exactly 3.2 times (96% CI 2.65–3.97) as likely as after cases without CDI. This relation of CD to endocarditis after VS probably was a result of the antibiotics used to treat endocarditis. At the same time, in patients having VS, there was no significant association of CDI with mediastinitis.
The CDI was one of the factors that increased the hospital mortality rate significantly after both CABG (OR 2.0; 95% CI 1.65–2.35) and VS (OR 1.9; 95% CI 1.51–2.39). The other risk factors for poor outcome after both surgical procedures were advanced age, female gender, black race, non-elective hospitalization, congestive heart failure, and chronic kidney disease (Fig. 2). Existence of CDI dramatically increased the median hospital LOS and cost after both CABG (from 7 d to 19 d and from $33,105 to $65,535; p<0.0001 for both) and VS (from 8 d to 24 d and from $41,876 to $95,699; p<0.0001 for both) (Fig. 3).

Risk factors for in-hospital death. (
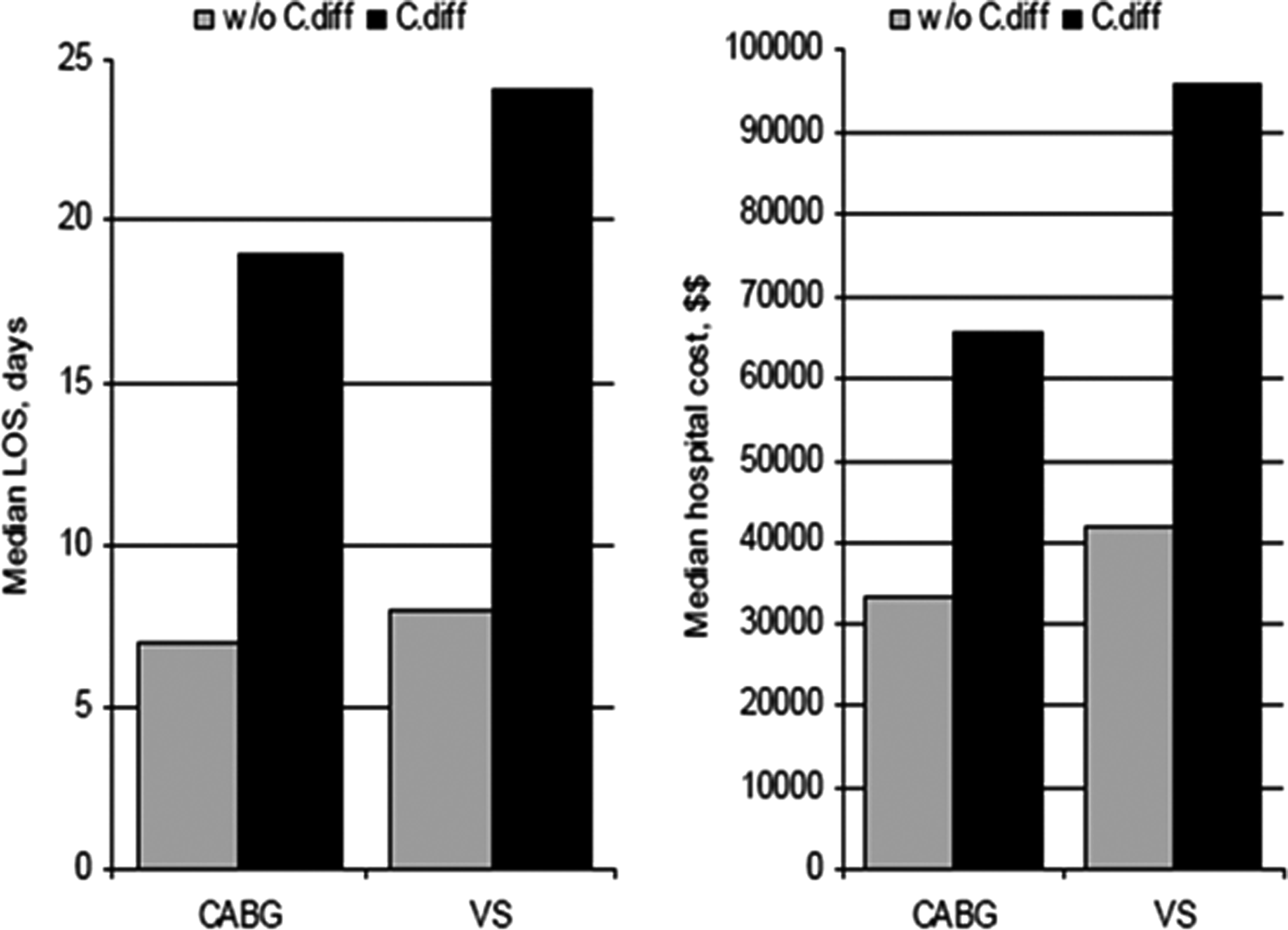
Effect of Clostridium difficile infection on length of stay (LOS) and hospital costs.
Discussion
The results from our study show the impact on post-operative mortality and morbidity of CDI in adult patients who undergo cardiac surgery. The presence of CDI increased the rates of hospital mortality after both CABG and VS, as well as causing a longer LOS and higher hospital costs. The development of post-operative infectious complications was associated with the presence of CDI. An explanation for this finding may be that the patients who developed post-operative infections required more long-term antibiotics, and as a result, they were more susceptible to CDI. For example, post-operative infection such as pneumonia required treatment with antibiotics that increased the risk of CDI.
The development of mediastinitis and endocarditis, two serious post-operative complications, was associated with CDI. The data set was not able to determine the sequence of events, and therefore, it is not clear which infectious complication occurred first. However, it is likely that the patients were treated for mediastinitis or endocarditis and consequently developed CDI.
The importance of a higher risk of mediastinitis or endocarditis should not be minimized. Although the incidence of mediastinitis is 1% to 3% [6,7], the associated mortality is 10%–35% [6,8,9]. Similarly, endocarditis has an incidence of 3–10 patients/100,000 person-years and a mortality rate of 9%–26% [10]. Moreover, the current in-hospital mortality rate for infective endocarditis is 15%–20% [11,12], with a one-year mortality rate of 40% [12,13]. As a result, an aggressive approach to preventing and treating both endocarditis and mediastinitis is of critical importance.
The microbial etiology of sternal incision infections varies and includes both gram-negative and gram-positive bacteria. However, the most common causative pathogens are Staphylococcus epidermidis (coagulase-negative staphylococci; CoNS) and S. aureus [14]. Similarly, the most common micro-organism leading to endocarditis that is isolated from blood cultures is gram-positive organisms, with S. aureus accounting for 31.2% of all infections. Staphylococcus aureus also is the most common organism in most major risk groups, including intravenous drug users and those with intracardiac devices [15]. The pathogens that lead to sternal incision infections and endocarditis therefore are distinct from CDI. As mentioned, the true relationship needs to be explored further.
One of the limitations to this study is that the relation between CDI and the other infections is not clear. The time sequence of the development of various infectious complications was not available. We hypothesize that patients who developed mediastinitis, endocarditis, and pneumonia would have been treated with long-term antibiotics and therefore be more susceptible to CDI. However, it is not known which infection developed first, the CDI or the additional infections such as pneumonia. At this time, it is clear that there is an association between CDI and the other infections, but that is all that can be concluded. A prospective study with post-operative followup would identify the time of development of CDI and other complications and determine causality.
One of the medical concerns regarding CDI is the progression of disease in some patients to fulminant colitis, a severe and complicated form of the disease that can be refractory to medical management, frequently necessitating extensive surgical intervention. Fulminant colitis occurs in 3%–8% of patients infected with CD and can progress quickly to shock and death even with appropriate initial medical treatment. The patients who do undergo surgical intervention are at high risk for operative death. It is estimated that surgical intervention is needed in 0.17%–3.50% of patients with CD-associated diarrhea [16]. The current standard of care for fulminant CDI is total abdominal colectomy with end-ileostomy. The mortality rate after colectomy for fulminant CDI is an astounding 34%–57% [17,18], a statistic that has improved only marginally since the first recognition of CDI. As a result, an aggressive approach to avoiding and, if this fails, treating CDI must be undertaken because surgical intervention carries a high risk.
Finally, the bacterium Clostridium difficile has become a common cause of healthcare-associated infection. It now is responsible for nearly all cases of pseudomembranous colitis and as many as 20% of cases of antibiotic-associated diarrhea without colitis. In 2001, the number of CDI cases reported in U.S. hospitals increased from 30–40 cases/100,000 to nearly 50/100,000. The number continued to increase at an alarming rate, subsequently reaching more than 84/100,000 cases in 2005 [19]. Patients are at greater risk for CDI with antibiotic exposure, gastrointestinal surgery or manipulation, and prolonged LOS in a healthcare facility. The rise in CDI has consequences for all patients, especially those who undergo surgical intervention and may be in a compromised state post-operatively.
Taken together, our study showed that CDI significantly worsened the outcomes after cardiac surgery in adult patients. It increased the rate of in-hospital death, LOS and cost after both procedures. It also was associated with post-operative infections such as mediastinitis and endocarditis. The implications of our study are compelling, and an aggressive approach must be undertaken to prevent and treat CDI.
Footnotes
Author Disclosure Statement
No competing financial interests exist.