
Abstract

A 65-
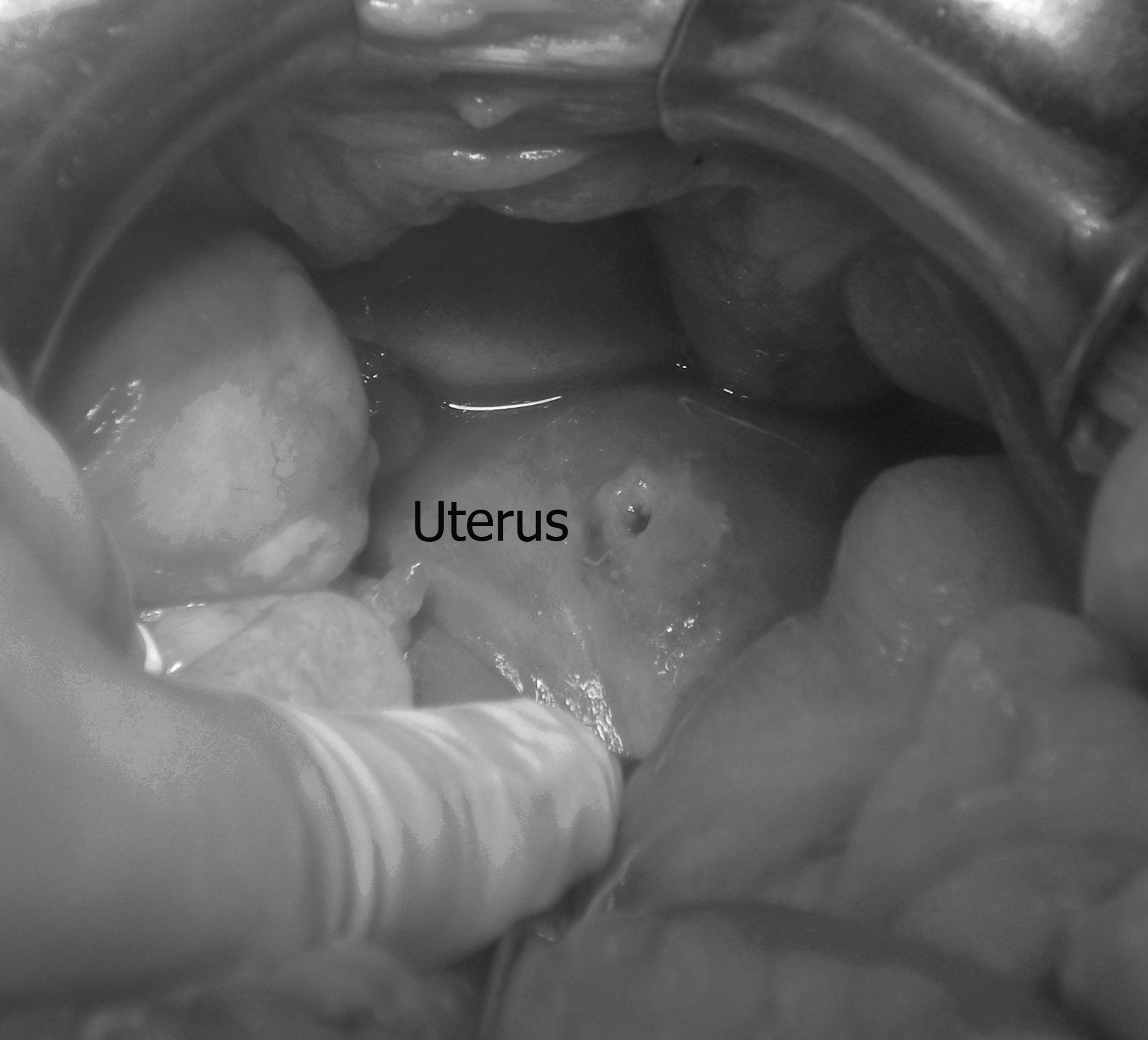
Intraoperative photograph showing perforation in the fundus of the uterus.
Pyometra is defined as collection of pus within the uterine cavity and occurs usually in elderly post-menopausal women. The classic triad of symptoms in patients with pyometra consists of purulent vaginal discharge, post-menopausal bleeding, and lower abdominal pain. However, more than 50% of all patients with pyometra are asymptomatic [1]. Spontaneous perforation of pyometra is a rare complication that may masquerade clinically as acute bowel perforation. In a review of 18 cases of spontaneous perforation of pyometra, Nakao et al. reported that intra-abdominal gas was reported in 56% of patients, and concluded that spontaneous pyometra perforation should be considered in the differential diagnosis of peritonitis in elderly women [2]. Early diagnosis is important in initiating immediate treatment, thus reducing morbidity and mortality.
The common pathology resulting in pyometra is compromised natural drainage of the uterine cavity through a stenosed cervix. The cervical occlusion may be caused by malignant or benign tumors, radiation cervicitis, atrophic cervicitis, infection, or congenital anomalies [3,4]. The compromised drainage causes accumulation of secretions that may become infected and result in pyometra. Spontaneous perforation of the uterus may occur at a site of degenerative or necrotic change following development of pyometra and can cause generalized peritonitis [3].