
Abstract
Abstract
Background:
Our institution had a major outbreak of multi-drug-resistant Acinetobacter (MDRA) in its general surgical and trauma intensive care units (ICUs) in 2011, requiring implementation of an aggressive infection-control response. We hypothesized that poor hand-hygiene compliance (HHC) may have contributed to the outbreak of MDRA. A response to the outbreak including aggressive environmental cleaning, cohorting, and increased hand hygiene compliance monitoring may have led to an increase in HHC after the outbreak and to a consequent decrease in the rates of infection by the nosocomial pathogens methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), and Clostridium difficile.
Methods:
Hand-hygiene compliance, tracked in monthly audits by trained and anonymous observers, was abstracted from an infection control database. The incidences of nosocomial MRSA, VRE, and C. difficile were calculated from a separate prospectively collected data base for 6 mo before and 12 mo after the 2011 outbreak of MDRA in the institution's general surgical and trauma ICUs, and data collected prospectively from two unaffected ICUs (the thoracic surgical ICU and medical intensive care unit [MICU]). We created a composite endpoint of “any resistant pathogen,” defined as MRSA, VRE, or C. difficile, and compared incidence rates over time, using the Wilcoxon signed rank test and Pearson product-moment correlation coefficient to measure the correlations among these rates.
Results:
Rates of HHC before and after the outbreak of MDRA were consistently high in both the general surgical (median rates: 100% before and 97.6% after the outbreak, p=0.93) and trauma ICUs (median rates: 90% before and 96.75% after the outbreak, p=0.14). In none of the ICUs included in the study did the rates of HHC increase in response to the outbreak of MDRA. The incidence of “any resistant pathogen” decreased in the general surgical ICU after the outbreak (from 6.7/1,000 patient-days before the outbreak to 2.7/1,000 patient-days after the outbreak, p=0.04), but this decrease did not correlate with HHC (trauma ICU: Pearson correlation [ρ]=−0.34, p=0.28; general surgical ICU: ρ=0.52, p=0.08).
Conclusions:
The 2011 outbreak of MDRA at our institution occurred despite high rates of HHC. Notwithstanding stable rates of HHC, the rates of infection with MRSA, VRE and C. difficile decreased in the general surgical ICU after the outbreak. This suggests that infection control tactics other than HHC play a crucial role in preventing the transmission of nosocomial pathogens, especially when rates of HHC have been maximized.
B
In 2011, our institution experienced an outbreak in its general surgical and trauma ICUs of multi-drug-resistant Acinetobacter (MDRA), a gram-negative bacterium that chiefly infects patients in surgical intensive care units (ICU). Multi-drug-resistant Acinetobacter, which is transmitted by contact, was reported in one study to increase mortality by 22% in hospitalized patients [8,9], and in another study to be responsible for more than $60,000 in additional patient fees and nearly two weeks of additional hospitalization, excluding costs for infection control, materials for patient isolation, increased use of antibiotics, and other factors [10]. Our institution contained its 2011 outbreak of MDRA through an aggressive, multi-disciplinary infection control response that involved closing down the units in which infection occurred, grouping infected patients into a cohort, discarding all disposable supplies, and deep-cleaning the units in which infection occurred and all of the permanent equipment in these units. Efforts to improve hand hygiene practices were a key component of this institutional response.
We conducted a study of our institution's management of the 2011 outbreak of MDRA to learn how to predict or prevent future outbreaks and inform hospital protocols with the means of accomplishing this. We developed three hypotheses for the study, as follows: (1) Poor hand hygiene compliance (HHC) was related to the incidence of outbreaks of MDRA; (2) an increase in HHC followed the response to the outbreak; (3) the increase in HHC that followed the outbreak was correlated inversely with rates of infection by other nosocomial pathogens that are transmitted by contact after the outbreak response, specifically methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), and Clostridium difficile.
Patients and Methods
We conducted a review of the incidence of resistant pathogens and rates of hand hygiene compliance at our institution before and after the 2011 outbreak of MDRA infection. The outbreak consisted of nine cases of such infection that were diagnosed in the trauma and general surgical ICUs of our institution between May and July 2011. The outbreak was controlled through an intensive, multi-faceted infection control effort, the components of which were the closing of the trauma and general surgery ICUs, the isolation from interpersonal contact of patients with MDRA infection, the cohorting of these patients into a single group, one-to-one nursing care for these patients, and the testing and disinfection of all permanent equipment and environmental surfaces that might have come into contact with patients and the deep cleaning of the closed ICUs. Physician traffic was limited: Only two physicians per team were allowed to enter each ICU room and examine the patient in the room. Universal precautions against contaminaton, including mandatory hand hygiene, gloving, and gowning, were enforced when any clinician provided care to a patient with an MDRA infection.
The Brigham and Women's Hospital, at which the study was conducted, is a 793-bed tertiary-care hospital and academic medical center in Boston, Massachusetts, with a dedicated 10-bed trauma ICU and a 10-bed general surgical ICU. The attending physician for each ICU is assigned two-week blocks from a multi-disciplinary team of surgeons, anesthesiologists, pulmonary-critical care physicians, and emergency critical care physicians. Nevertheless, all major decisions about the care of a patient in the trauma or general surgical ICU are shared with the patient's attending surgeon. A separate 20-bed medical ICU and a 10-bed thoracic surgical ICU also exist within the institution. All of the institution's surgical ICUs use a semi-closed ICU model, whereas the medical ICU uses a closed staffing model. Nursing and ancillary staff members are unique to each unit, with no overlap of these personnel with those of other units in patient care. The standard nurse-to-patient ratio in the ICUs tends to vary at 1:1 or 1:2. On all units, nurses collect perirectal swabs for microbiologic testing for VRE and nasal swabs for testing for MRSA on admission and on a weekly basis thereafter in patients not known to be colonized. Screening of patients for multi-drug-resistant gram-negative bacilli or for C. difficile is done at the treating clinician's discretion. Patients identified as being colonized or infected with MRSA, VRE, or Clostridium difficile are put under contact precautions and their charts are flagged in the hospital's electronic medical record system.
The hospital tracks hand-hygiene compliance routinely through a series of random audits by staff members of the infection control department. Observations for these audits are made on a daily basis, including weekends, at any time of the day or night, and without warning. The results are sent immediately to department directors, managers, educators, and supervisors. Monthly data are collected by staff members of the infection control department and uploaded into a hospital-wide, web-based quality-monitoring and reporting database. Observations about hand hygiene are recorded for the following situations, based on the World Health Organization's “five moments of hand hygiene” and recommendations of the U.S. Centers for Disease Control and Prevention (CDC) [11]:
• Immediately before and after contact with a patient or the patient's environment (e.g., stretcher, bedside cart, intravenous [IV] tubing). • Immediately before and after a staff member's glove use. • Before invasive procedures, before the manipulation of invasive devices, before and during wound dressing or other aseptic tasks. • When moving from a contaminated to a non-contaminated body site during the care of a patient. • After exposure or the risk of exposure to blood or other body fluids.
Observations made in the foregoing situations typically involve 20 random hand hygiene opportunities per ICU per month, although the number of observations during the hospital's 2011 outbreak of MDRA was two- to eight-fold greater than before the outbreak. The number of occasions on which a clinician was observed to wash his/her hands with either an alcohol-based hand rub or soap and water, as a fraction of the number of occasions on which this is supposed to be done, is reported as the unit's compliance rate for that month. Hand hygiene stations are available near the doors to patient rooms (for alcohol-based hand rub preparations) and immediately upon entry into the room (for both alcohol-based hand rub preparations and as sinks for washing with soap and water). These observations are entered into a prospective database, which for the purpose of the study was analyzed for rates of compliance over time in the four ICUs involved in the study before and after the 2011 outbreak of MDRA. The study was focused on four ICUs: Two of which experienced MDRA outbreaks (the trauma ICU and general surgical ICU) experienced outbreaks of MDRA and two of which did not (the medical ICU and thoracic surgical ICU).
In addition to monitoring compliance with hand hygiene, we queried the prospective database maintained by the hospital's infection control department of all patients with multi-drug-resistant organisms to identify incident cases of colonization or infection with MRSA, VRE, and C. difficile in the 6 mo preceding and 12 mo following the Acinetobacter outbreaks in our trauma and general surgical ICUs. No attempt was made to distinguish colonization from active infection. The hospital's ICUs conduct active surveillance for MRSA and VRE on all new admissions and weekly thereafter. We focused on four ICUs, consisting of the two that experienced an outbreak of MDRA (trauma ICU and general surgical ICU) and two that did not (medical ICU and thoracic surgical ICU). To account for any differences in the patient populations of these units during the study period, we obtained standard metrics for evaluating the quality of ICU performance, such as demographics, length of stay, and case-mix index.
We used the Pearson product moment coefficient of correlation, ρ, to determine the correlation between rates of hand hygiene compliance and rates of colonization or infection with “any resistant pathogen.” We compared this composite outcome for each of the ICUs included in the study before and after the MDRA outbreak, using the two-sided Wilcoxon signed-rank test. Counts of different pathogens were combined in order to enhance the statistical power of these analyses. A value of p<0.05 was considered statistically significant for the purposes of the study. All statistical analyses were done with SAS version 9.3 (SAS Institute, Cary, NC).
Results
Figure 1 shows the median and interquartile ranges (IQR) for compliance with hand hygiene before and after the 2011 outbreak of MDRA at our institution. The rates of HHC in both the trauma intensive care and general surgical ICUs were consistently high both before and after the outbreaks of MDRA in these units. In the general surgical ICU, the median HHC before the outbreak was 100%. After the outbreak, the HHC in the general surgical ICU decreased to 97.6%, although this was not statistically significant (p=0.93). However, the incidence of resistant pathogens in the general surgical ICU decreased after the response to the MDRA outbreak (from 6.7 to 2.7/1,000 patient-days, p=0.04). In the trauma ICU, the median rate of HHC was 90% before the outbreak and increased to 96.75% after the outbreak, with this change also not statistically significant (p=0.14).
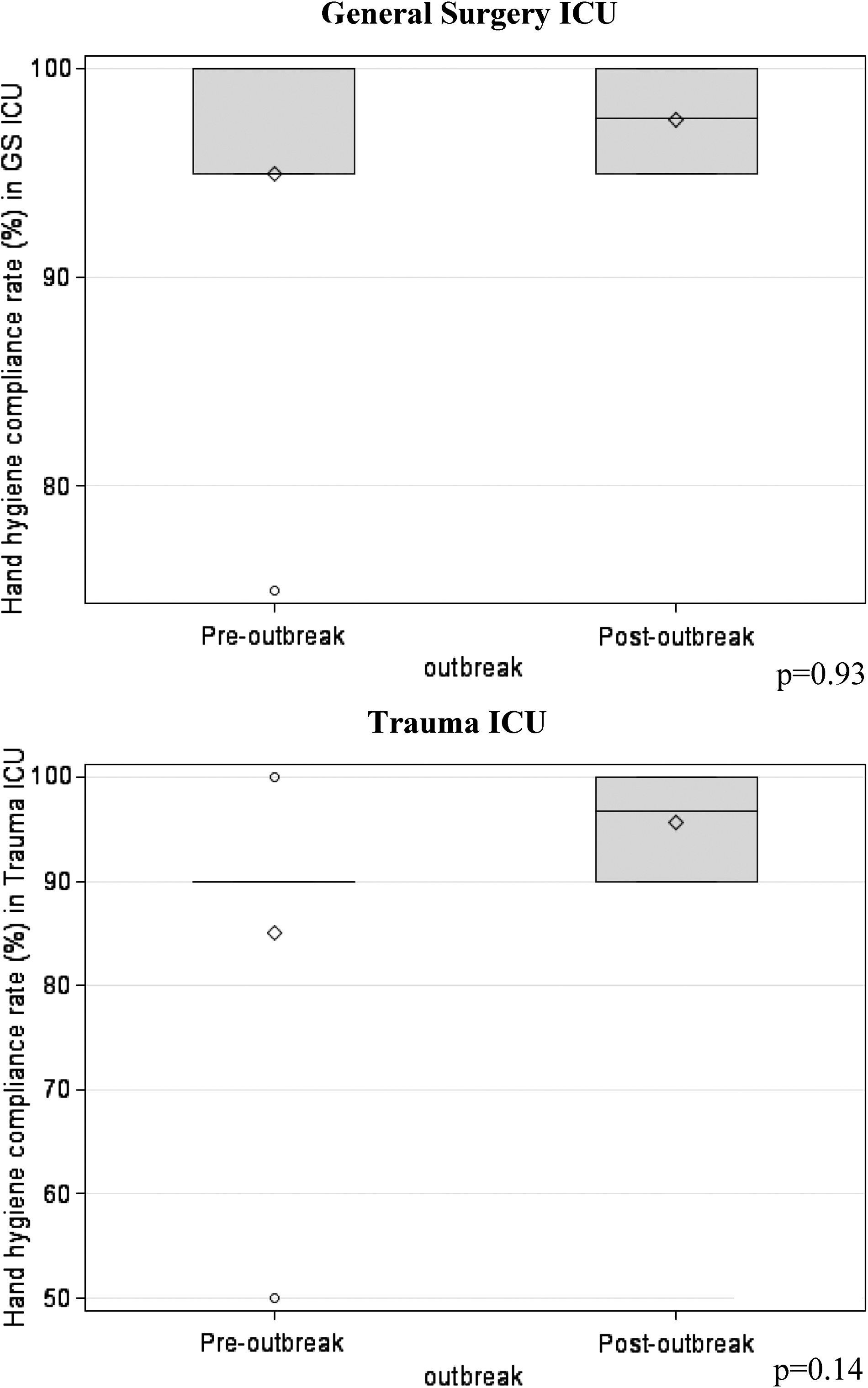
Median and inter-quartile ranges for hand hygiene compliance for 6 mo before and after response to 2011 outbreak of multi-drug resistant Acinetobacter.
There was no correlation between the rates of HHC and rates of colonization or infection with “any resistant pathogen” in the ICUs (trauma ICU: ρ=−0.34, p=0.28; general surgical ICU: ρ=0.52, p=0.08) from before to after the 2011 outbreak of MDRA. No changes occurred in the rates of HHC from before to after the outbreak of MDRA in either of the ICUs (medical ICU and thoracic surgical ICU) that were unaffected by the outbreak and were used as controls in the study.
Rates of Incidence of Colonization or Infection
There were 84 cases of colonization or infection with MRSA, VRE, or C. difficile in the four ICUs included in the study during the study period. When we examined the median incidences of colonization or infection with each of these three pathogens before and after the outbreak of MDRA, we found no statistically significant differences (Table 1). When we compared the rates of colonization or infection for the composite endpoint of “any resistant pathogen” in the ICUs included in the study, we found a 48% decrease in the median incidence of this composite measure in the general surgical ICU, from 7.7/1,000 patient-days before the MDRA outbreak to 4.0/1,000 patient-days after the outbreak (p=0.04). However, no statistically significant change in this endpoint was found from the beginning to the end of the study in the trauma ICU, with an incidence of 4.6/1,000 patient-days before the outbreak and 1.9/1,000 patient-days after the outbreak (p=0.41) (Table 2). No change in the incidence of colonization or infection with the composite endpoint was found during the study period in the medical and thoracic surgical ICUs, which were unaffected by the outbreaks of MDRA in the trauma and general surgical ICUs, and there was no evidence of differences in the baseline patient populations of these latter two ICUs that would account for these findings (Table 3). Interestingly, the decreased incidence of colonization or infection with “any resistant pathogen” in the general surgical ICU did not persist. During the period from 6–12 mo after the outbreak, the median incidence of such colonization or infection in the general surgical ICU increased from 4.0 to 6.9 cases/1,000 patient-days, which did not differ significantly from the median incidence before the outbreak (p=0.69).
Statistically significant difference.
MRSA=methicillin-resistant S. aureus; VRE=vancomycin-resistant Enterococcus; MDRA=multi-drug-resistant Acinetobacter; NS=not significant; GS=general surgery.
statistically significant decrease compared to previous period, p=0.044.
GS=general surgery.
CMI=case mix index; ALOS=average length of stay; GS=general surgery; NS=not significant.
Discussion
Hand hygiene is considered the most important factor in limiting the transmission of infections within hospitals [6], and institutions work aggressively to ensure high compliance with such hygiene. An outbreak of MDRA occurred in the general surgical and trauma ICUs at our institution despite consistently high rates of compliance with measures for hand hygiene. Containment of the outbreak required a multi-faceted and multi-disciplinary infection control strategy, and rates of HHC remained high after the institution responded to the outbreak. However, when rates of HHC were plotted against the incidence of colonization or infection with MRSA, VRE, or C. difficile, no correlation was noticed in either of the units in which the outbreak of MDRA had occurred, despite a significant decrease in the incidence of such colonization or infection in the general surgical ICU. In 2011, when the outbreak of MDRA occurred, the median incidence of colonization or infection with the composite measure designated as “any resistant pathogen” decreased by 48% in the general surgical ICU, from 7.7 /1,000 patient-days before the outbreak to 4.0/1,000 patient-days after the outbreak. Furthermore, the rates of colonization or infection with resistant pathogens in the trauma ICU, which served as one of two control units in our study, were unaffected by the response to the MDRA outbreak or by a high rate of HHC.
The findings in our study may have many explanations. One of them is that the intermittent capture of HHC does not accurately represent general hand hygiene, and that the rate of HHC is typically substantially lower than the recorded rate, or that rates of compliance with HHC are high in general but that missed opportunities for hand hygiene that were not captured and recorded were the critical infractions that allowed the outbreaks of MDRA in our trauma and general surgical ICUs to occur. Furthermore, when rates of HHC are high consistently, variations in compliance may simply be an effect of chance, and may not have an effect on the transmission of nosocomial pathogens. Thus, for example, one may ask whether a 97% rate of compliance with HHC has a greater restrictive effect on infection transmission than does a 95% rate of compliance. Lastly, it is possible that when the rate of HHC is high, factors such as environmental cleaning assume greater relative roles in reducing the transmission of resistant pathogens than they have in the presence of a lower rate of HHC. Perhaps the traditional focus of infection control on hand hygiene and HHC has been successful, but it is time to expand the degree of complexity of hospital infection control to include aggressive environmental management, antibiotic stewardship, and patient decontamination as key components of an institutional protocol for such control.
In published rates of HHC, the rates among institutions have been reported as being below 50% [7]. Yet the measured rates of HHC at our institution are quite high. Of the different methods of measuring HHC, direct observation is considered the gold standard because it is the only method that can provide information about details of HHC, such as hand hygiene technique, types of hand hygiene opportunities, and rates of HHC for different healthcare workers [12]. However, the direct observation of HHC among healthcare workers is costly, and potentially overestimates compliance because it captures only a small percentage of hand hygiene opportunities, and can be influenced by the Hawthorne effect in which compliance improves when workers know that they are being observed [13–15]. Thus it is possible that the rates of HHC identified in our study, although measured through the gold-standard technique of direct observation, do not truly represent the actual rate of HHC in the ICUs in which they were determined. It is also possible that we may be systematically missing periods when levels of HHC decline, because the direct observation of HHC is done only on a periodic basis. Furthermore, comparing rates of compliance based on observation is challenging because of the lack of standardized criteria for compliance and observation techniques [16]. Other methods than direct observation for assessing compliance, such as electronic sensors or tags, have been shown to be effective monitoring tools for hand hygiene [17–19]. These methods could be used as periodic comparators with direct observation to determine the accuracy of our rates of HHC. Thus, a limiting factor in our study may have been the accuracy of our institution's measured rate of HHC.
Other components of infection control, such as environmental cleaning, may have contributed to the significant decrease in rates of colonization or infection with “any resistant pathogen” in our general surgical ICU. Aggressive environmental cleaning was undertaken to contain the 2011 outbreak of MDRA in our hospital's trauma and general surgical ICUs, and may therefore have had a greater effect than HHC on subsequent rates of colonization or infection with resistant pathogens. The environment, patients, and clinicians are known to be key inter-related sources of resistant organisms in the ICU. Environmental contamination was a major factor in the transmission of multi-drug-resistant bacteria to healthcare workers in a study that tested the role of environmental contamination in the transmission of these organisms to healthcare workers' clothing, and which found that healthcare workers had a four-fold greater than average likelihood of acquiring resistant organisms when environmental cultures of these organisms were positive [20]. Huang et al. found that the risk of contamination with multi-drug-resistant organisms was higher when a room had been used by a colonized/infected patient, and that improving cleaning decreases this rate, especially for methicillin-resistant Staphylococcus aureus (MRSA) [21,22]. Additionally, one analysis of six prospective cohort studies found that 70% of nosocomial infections in those studies were considered to be hospital-acquired because they occurred within 48 h after admission of a patient to an ICU. However, of these infections, only 40% were the direct result of transmission from a contaminated carrier; 60% were caused by organisms endogenous to the patient, making a strong argument for screening for pathogens at the time of ICU admission. Thus, even under ideal circumstances, hand washing can only affect as many as 40% of healthcare-associated infections in the ICU [23]. Rigorous cleaning with close monitoring can substantially reduce the likelihood of an environmental culture positive for MRSA or VRE [24,25]. Techniques such as bioluminescence assays have been shown to be effective options for evaluating the quality of cleaning programs [26]. Recently, Climo and Yokoe, in a randomized controlled trial of daily bathing with chlorhexidine-impregnated washcloths, confirmed that interventions that reduce the density of colonization of body sites are important adjuncts to effective hand hygiene. The bathing with chlorhexidine-impregnated washcloths used in their trial reduced substantially, by 23%, the rate of multi-drug-resistant organisms and likewise reduced, by 28%, the development of hospital-acquired blood-stream infections [27]. Thus, the complex relationship between the patient, the environment, and healthcare workers cannot simply be summed up in the traditional mantra of “wash your hands!” A more thoughtful and coordinated approach to infection control may be the way forward.
Our study has many limitations that need to be taken into account when analyzing its results. It was a single-institution study, and because of this, generalizing its results to other hospitals or ICUs may not be possible. Furthermore, our data for HHC may not be accurate enough to demonstrate changes in compliance because our measurement of such compliance was not a continuous process but was based on periodic observations by trained staff members. Additionally, during the outbreak of MDRA at our institution, the institution's ICUs implemented strict universal precautions, which may have also, if inadvertently, limited the effect of hand hygiene on the rates of colonization or infection with resistant pathogens. Lastly, for our statistical analysis, we used averages of rates of HHC across 6-mo periods before and after the outbreak of MDRA in the affected ICUs. However, this time frame may be too long to permit accurate assessment of the correlation between promotion of hand hygiene and rates of colonization or infection with resistant pathogens. It also may not account for possible secular trends toward higher or lower HHC rates that may have preceded our period of observation, or may not take into account the effect of poor HHC for short periods that were not covered by our periodic assessments.
In conclusion, the 2011 outbreak of MDRA at our institution occurred despite recorded high rates of HHC, and these rates remained high after the outbreak. However, despite consistently high rates of HHC, the incidence of “any resistant pathogen” decreased in the general surgical ICU after the response to the outbreak. This suggests that when rates of HHC have been maximized, other components of the multi-faceted approach to infection control, such as environmental decontamination and cohorting of patients, play increasingly crucial roles in preventing the transmission of nosocomial pathogens. Unexpectedly, the trauma ICU that was part of our study did not have any changes in its rates of colonization or infection with “any resistant pathogen,” and rates of HHC in this unit remained high throughout the period of the study, again suggesting that infection control programs need to consider additional interventions beyond hand hygiene alone to control the nosocomial spread of pathogens.
Footnotes
Acknowledgments and Author Disclosure Statement
We thank Dr. Stanley Ashley, Dr. Allen Kachalia, and the Partners Center for Clinical Excellence for their support. Preliminary data in our study was presented as a poster at the Society for Critical Care Medicine Conference in San Juan, Puerto Rico, in January 2013. Final results were given as an oral presentation at the Thirty-third Annual Meeting of the Surgical Infection Society Conference in Las Vegas, Nevada in April 2013. We thank both societies for the opportunities to discuss this work. Financial Support for this study was provided by the Partners Centers of Expertise Quality and Patient Safety Program and Partners Graduate Medical Education for conference travel.
Lastly, we are grateful to all of our patients for the opportunity to care for them, and to PK, in particular, whose illness spurred us to ask these questions. The authors have no competing financial interests in the work described here.