
Abstract

M
A 66-year-old male presented to the emergency department with a 5-d history of generalized fatigue, subjective fever and chills, shortness of breath, and diffuse abdominal pain. He had undergone deceased donor heterotopic kidney transplantation previously and was on tacrolimus and mycophenolate immunosuppresion for graft preservation, with the last drug being discontinued for recent-onset neutropenia. A computed tomography (CT) scan of the abdomen and pelvis revealed thickening of the terminal ileum and colon extending from the cecum to the hepatic flexure, associated with pericolic fat stranding and fluid in the pericolic gutter. There was no evidence of pneumoperitoneum, pneumotosis, obstruction, or abscess (Fig. 1). He was kept nil per os, on parenteral nutrition, and on broad-spectrum antibiotics including piperacillin-tazobactem, metronidazole, azithromycin, and fluconazole.
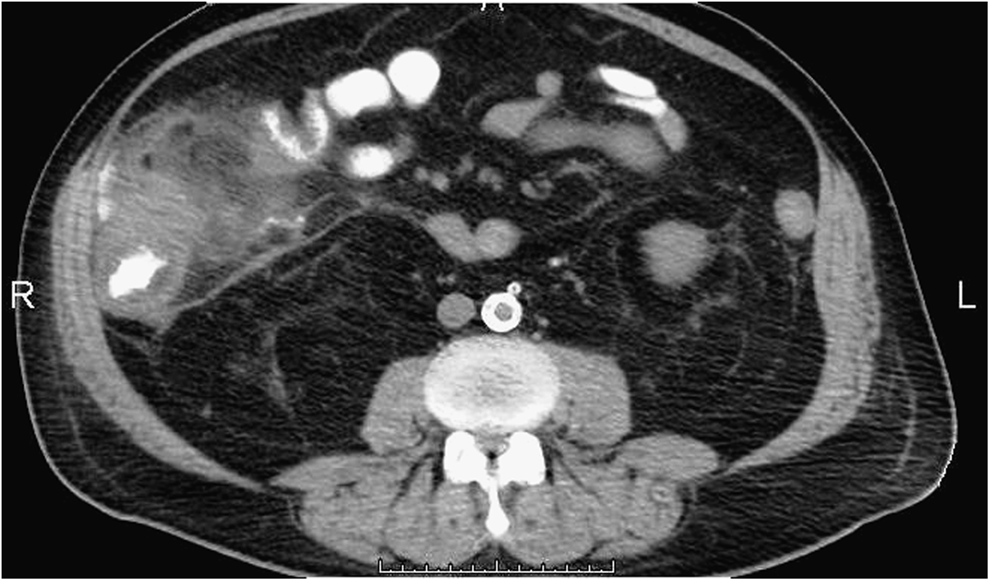
Computed tomography scan showing inflammation and thickening of the ascending colon and terminal ileum with pericolic fat stranding.
After 8 d, a repeat CT scan revealed localized perforation of the cecum. Resection of the terminal ileum and a right hemicolectomy was performed, with an end-ileostomy and mucous fistula. Pathologic examination of the surgical specimen revealed non-septated hyphal elements with associated ulceration, mucosal necrosis, and poorly formed granulomata (Fig. 2 and Fig. 3). He had a complicated post-operative course including respiratory failure with prolonged endotracheal intubation, acute-on-chronic renal failure requiring hemodialysis, and fungal growth at the laparotomy incision (treated with topical Dakin solution). Despite aggressive medical management, the patient's family decided to withdraw care and on post-operative day 48, the patient died.
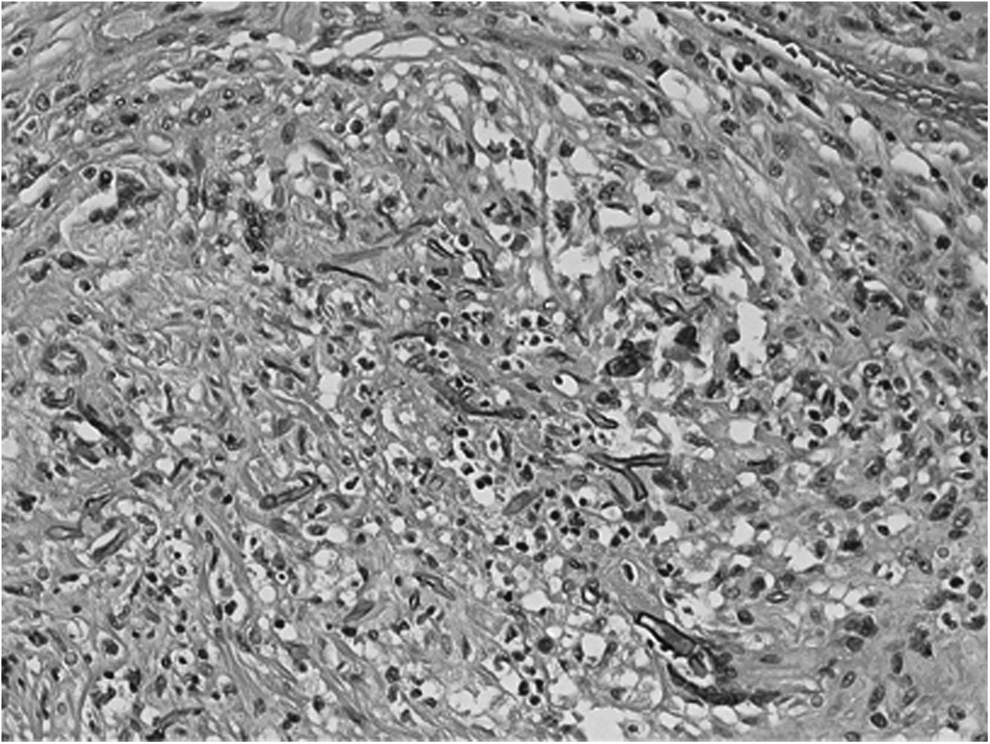
Poorly formed granuloma with giant cells and fungal elements.
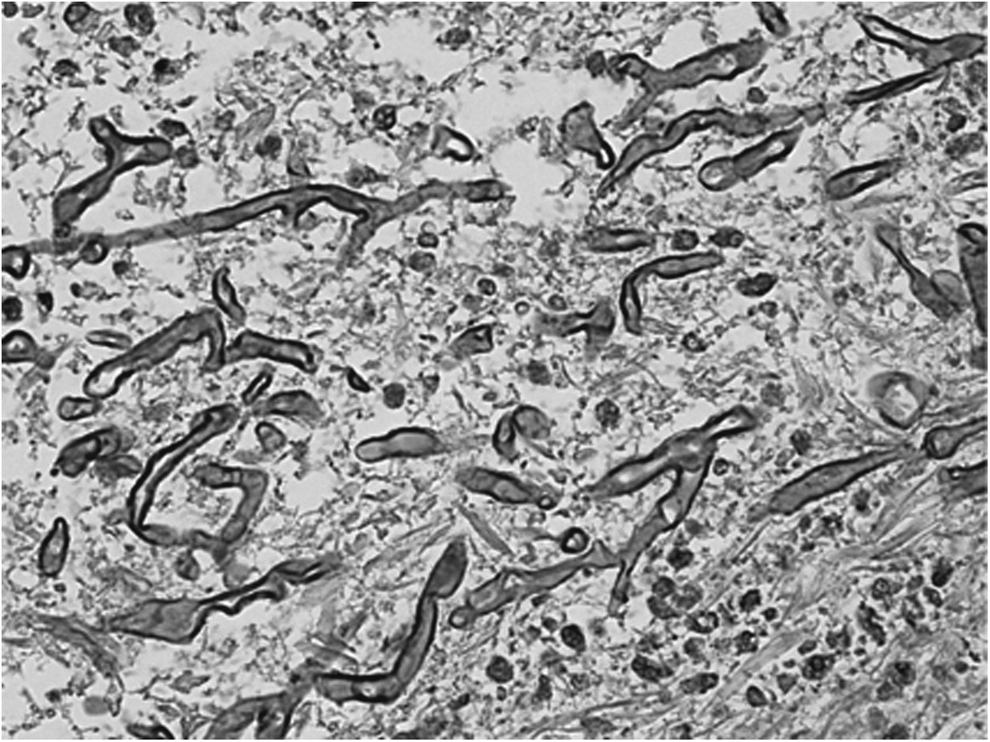
High-power Gomori methenamine silver stain showing non-septated hyphae.
Colonic mucormycosis is a serious and often fatal infection characteristic of immunocompromised states. Combined early surgical and medical treatment is essential to increase the probability of a favorable outcome. With a high clinical suspicion, colonoscopy may be a viable option to facilitate early diagnosis and treatment [4,5]. Visceral perforation often leads to disseminated infection and multiple organ dysfunction syndrome despite disease directed therapy, and often results in poor outcomes.