
Abstract
Abstract
Background:
The clinical role of hyperoxia for preventing surgical site infection (SSI) remains uncertain because randomized controlled trials on this topic have reported disparate results. One of the principal reasons for this outcome may be that prior trials have entered heterogeneous populations of patients and a variety of procedures. The aim of our study was to assess the influence of hyperoxygenation on SSI using a homogeneous study population.
Methods:
From January 2004 to April 2013, we studied, in a randomized trial, 239 patients, who underwent open surgery for perforated peptic ulcer (PPU). The surgical procedure was performed through an upper abdominal midline incision, and closure of PPU was achieved by suture alone or in combination with an omental patch. Patients were assigned randomly to an oxygen/air mixture with a fraction of inspired oxygen (F
Results:
The overall incision infection rate was 38.4% (92 of 239): 61 patients (50.8%) had an infection in the 30% F
Conclusions:
Supplemental 80% F
S
Achieving high oxygen tension at the site of surgery has been proposed as a means of reducing the risk of SSI on the basis of data showing that oxygen can enhance the oxidative processes in white cells, thus facilitating bacterial killing [6]. A number of preclinical studies have demonstrated that a high tissue oxygen concentration promotes local incision healing in animal models [7,8]. Recent studies in human beings have found that administration of supplemental oxygen in the peri-operative period to patients undergoing abdominal surgery may reduce the risk of SSI [9–12]. However, not all studies have found this benefit, and one paradoxically found a greater risk of SSI with peri-operative oxygenation administration [13].
One of the principal reasons for such mixed results may be that prior trials have entered a heterogenous population of patients and used a variety of procedures, which may have precluded the discovery of small but important differences. To overcome this problem, we performed a randomized controlled trial in a patient population with a single diagnosis (perforated peptic ulcer [PPU]), using one standard approach (open closure of PPU with sutures alone or in combination with an omental patch through an upper abdominal midline incision). Hence, the aim of our study was to obtain satisfactory statistical information considering the effects of hyperoxygenation on SSI after this procedure in a relatively homogeneous study population.
Patients and Methods
Patient selection
From January 2004 to April 2013, we analyzed, in a randomized study, 246 consecutive patients, all of whom presented with a clinical and radiologic diagnosis of PPU. The diagnosed was confirmed in 239 cases at surgery (153 men, 86 women; mean age 60.3 y). The exclusion criteria were expected surgery time of less than 30 min, presence of diabetes mellitus (type 1 or 2), known immunologic dysfunction (advanced liver disease, human immunodeficiency virus infection, hepatitis C virus infection), weight loss exceeding 20% in the previous three months, serum albumin concentration of <30 g/L, and a leukocyte count of <2,500/mL. We also excluded patients who were taking corticosteroids or other drugs that may affect the immunologic response.
The medical history was recorded, and a systematic physical examination was performed pre-operatively. Patients were considered to have respiratory disease when they had a history of chronic obstructive pulmonary disease, asthma requiring routine medication, or other clinically important impairment. The patients were classified as grade I, II, or III according to the American Society of Anesthesiologists (ASA) grading system [14] (Table 1).
ASA = American Society of Anethesiologists; NNISS = National Nosocomial Infections Surveillance System; SENIC = Study of the Efficacy of Nosocomial Infection Control.
The severity of sepsis was valued by Acute Physiologic and Chronic Health Evaluation (APACHE) II score and the Mannheim Peritonitis Index (MPI) [15,16].
The risk of infection was assessed with the National Nosocomial Infections Surveillance System (NNISS) and the Study of the Efficacy of Nosocomial Infection Control (SENIC) scales [17,18]. These scores have been validated extensively, and higher scores indicate a greater risk of infection. These scores are illustrated in Table 2.
ASA = American Society of Anesthesiologists; NNISS = National Nosocomial Infections Surveillance System; SENIC = Study of the Efficacy of Nosocomial Infection Control.
Treatment protocol
The initial supportive treatment was the same for both groups of patients. Thus, all patients received intravenous fluid infusion, intravenous antibiotics in the hour prior to the start of surgery (cefotaxime every 8 h and tobramycin every 12 h: Dosage was adjusted for patient weight), proton pump inhibitor (omeprazole 40 mg intravenously every 12 h) and for pain relief: Ketorolac tromethamine (30 mg intravenously every 6 h). Prophylactic subcutaneous heparin was administered daily until discharge from the hospital. There were no indications for blood transfusion. Antibiotic therapy was continued for 6 to 10 d after surgery.
Anesthesia was obtained using the same procedure for all patients. Pre-anesthesia was accomplished using atropine (0.01 mg/kg) plus promethazine (0.5 mg/kg), induction was using sodium thiopental (5 mg/kg) and atracurium (0.5 mg/kg), with tracheal intubation and assisted ventilation using nitrogen dioxide/oxygen 2:1. After intubation, anesthesia was maintained with oxygen in air, sevoflurane, and remifentanil (0.25 mcg/min).
Randomization to intervention was stratified by study center, and the patients were randomized in blocks. Computer-generated codes were maintained in sequentially numbered opaque envelopes. The randomization envelopes were opened in the operating department after induction of anesthesia by the anesthesiologist. On the basis of the contents, patients were assigned to an oxygen/air mixture with a fraction of inspired oxygen (F
The Ethical Committee of the Department of Surgery at the University of L'Aquila approved the study protocol. All patients gave informed written consent.
Open surgical procedures were performed through an upper abdominal midline incision within 3 to 6 h of admission (mean 4.8 h; range 3.0–6 h) in patients assigned to 30% oxygen and 5.1 h (range 3.4–6 h) in those assigned to 80% oxygen,. Closure of the PPU was achieved by suture alone or in combination with an omental patch.
Peritoneal lavage was performed with at least 4 L of warm physiologic saline or until the aspirate was clear. In all patients, the surgical incision was irrigated and sutured meticulously with absorbable sutures. The skin was closed using nonabsorbable silk sutures.
The electrocardiogram, heart rate, noninvasive blood pressure, F
When the operation was finished, the inhaled anesthetic was stopped, and the F
Follow-up
In the post-operative anesthesia care unit (PACU), vital signs (blood pressure, pulse, ventilation, pulse oximetry, and answering of questions) were monitored every 15 min. Patients were discharged from the PACU when vital signs were normalized.
We used a prophylactic multimodal analgesic technique for treatment of post-operative pain. Thus, patients received incisional local anesthetics with a total of 20 mL (100 mg) of 0.5% bupivacaine. Intravenous ketorolac tromethamine (30 mg) was given every 6 h on the two days after the operation and afterward on demand.
Surgical incisions were assessed daily for infection by surgeons who were unaware of the patients' treatment groups. Infections were graded using a classification described elsewhere [19]. Incisional infections were considered grade 1 in the presence of erythema, induration, and pain; grade 2, same as grade 1 but with serous fluid; grade 3, the presence of contaminated fluid in less than half the site; and grade 4, same as grade 3 but contaminated fluid in more than half the incision. Incisional dehiscence was considered to be present when surgical closure of the cutaneous or subcutaneous tissue (superficial) or the fascia and muscular plane (deep) was necessary in the early post-operative period.
Incisions were considered infected when they met U.S. Centers for Disease Control and Prevention definitions [20]. Purulent exudates were cultured and, when they were positive for pathogenic bacteria, appropriate antibiotic treatment was initiated. Only those infections diagnosed during the first 14 d post-operatively were included.
Incision healing characteristics were evaluated using the Additional treatment, Serous discharge, Erythema, Purulent exudate, Separation of deep tissues, Isolation of bacteria, and duration of inpatient Stay (ASEPSIS) score [21]. This is an established and validated system that is derived from the weighted sum of points assigned for the following factors: Duration of antibiotic administration; drainage of pus with the patient under local anesthesia; debridement of the site with the patient under general anesthesia; serous discharge; erythema; purulent exudate; separation of deep tissues; and hospitalization exceeding 14 d. A daily score of 20 or more was considered evidence of infection [22]. Discharged patients were observed in the out-patient surgical clinic on day 15 to assess incision status.
Statistical analysis
Independent medians were compared with the Mann-Whitney U test and paired medians with the Wilcoxon test or Friedman test for more than two variables. Proportions were compared with the Fisher exact test, the likelihood ratio test, or the Pearson χ2 test as indicated. All p values are two tailed. Statistical analysis was performed using SPSS® version 13.0 for Windows (SPSS; Chicago, Illinois, USA).
The risk of SSI associated with a given factor was determined by calculating the cumulative incidence. To evaluate the relation between the F
The goodness-of-fit of the model was evaluated with the Hosmer-Lemeshow method.
Results
We collected data from 239 patients who were enrolled and randomized: 120 received 30% peri-operative oxygen, and 119 received 80% peri-operative oxygen. In Fig. 1, the CONSORT analysis is described in detail [23]. The projected sample size was about 260 patients. The decision to conclude the study at 239 patients was made because of the impression that statistically significant results had been obtained already.
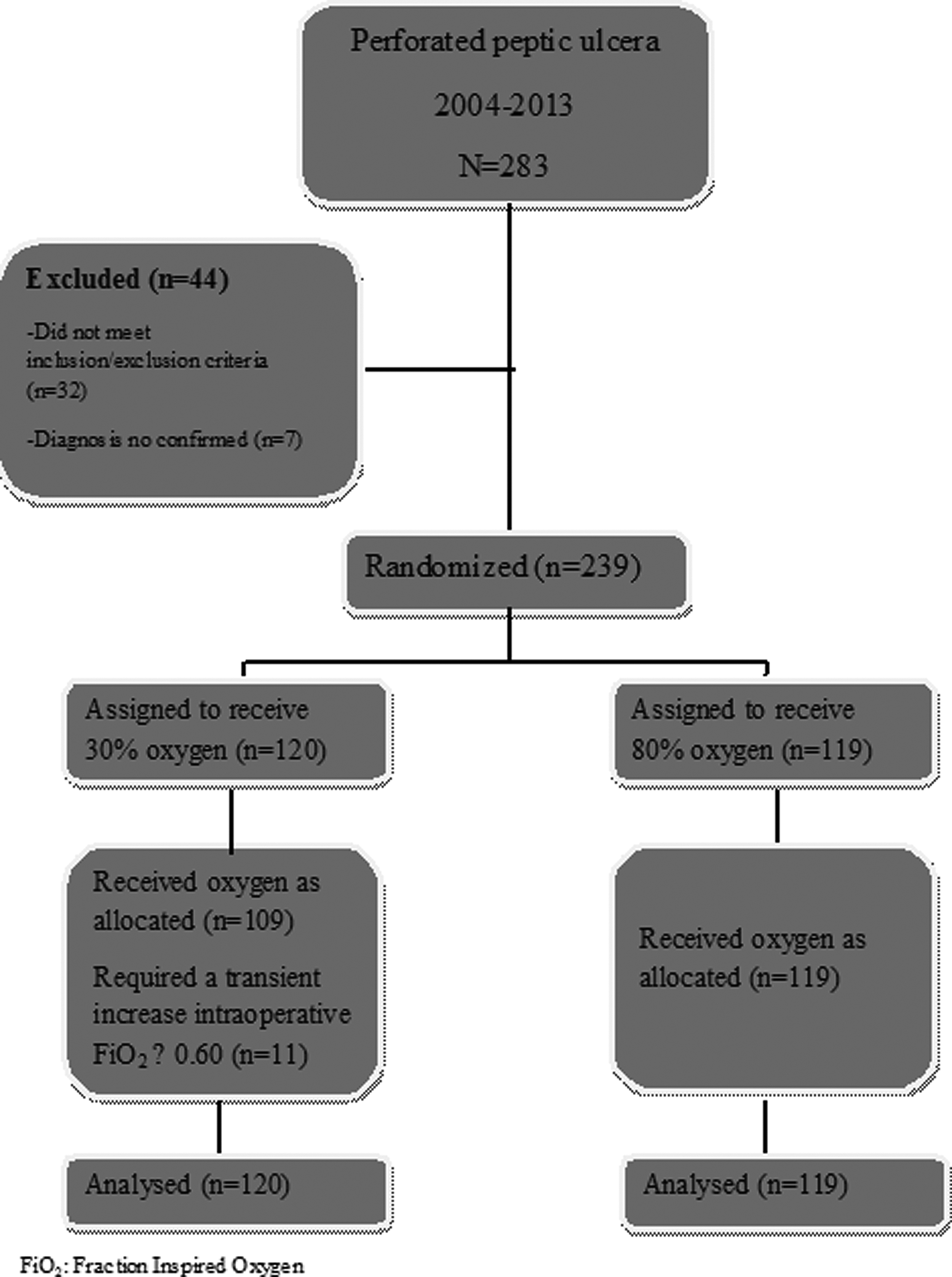
Trial design.
The trial extended over a period of 10 years. At the time of the planned interim analysis (January 2009), 108 patients had been randomized: 55 received 30% peri-operative oxygen, and 53 received 80% peri-operative oxygen. The relative risk reduction of SSI was in favor of the 80% oxygen group, but the difference was not statistically significant. During these 10 years, there were no changes in patient care, either operatively or peri-operatively. Morphometric, demographic, and other pre-operative characteristics were similar in the two treatment groups (Table 1). There was no significant difference in the two groups in the nutritional status, as assessed by Nutrition Risk Screening 2002 (NRS), or Kondrup Score based on age, recent weight loss, body mass index (BMI), severity of disease, or planned surgical intervention [24]. Other than the percentage of inspired F
The mean duration of surgery was 58.7 min (range 33–102 min) in patients assigned to 30% oxygen and 63.2 min (range 38–104 min) in those assigned to 80% oxygen (p = 0.80). The overall SSI rate was 38.4% (92/239); of these, 83 patients had cultures positive for pathogenic bacteria. A total of 61 patients (50.8%) in the 30% F
ASEPSIS: Additional treatment, Serous discharge, Erythema, Purulent exudate, Separation of deep tissues, Isolation of bacteria, and duration of inpatient Stay.
No wound dehiscence (deep/organ-space SSI) was observed in any patient. No patient required surgical revision or re-operation for this complication, and all incision infections were managed successfully with secondary closure. The risk of SSI was 39% lower in the 80% F
Categorical variables were F
CI = Confidence interval; F
Eleven of 120 patients (9.1%) in the 30% oxygen group required an F
Patients with infection had mean (standard deviation [SD]) ASEPSIS scores on the first six post-operative days of 9.2 ± 0.84 (standard deviation), whereas those without infection had a mean score of 5.1 ± 0.56 (p = 0.002). Patients with infection took longer to ambulate (mean 4.7 ± 3.8 vs. 2.8 ± 2.6 d; p = 0.007), had their staples removed later (11.4 ±2.8 vs. 9.8 ± 3.4 d; p = 0.006), and had longer hospital stays (14.8 ± 6.4 vs. 11.3 ± 4.1 d; p = 0.001).
In unadjusted analyses, men and those with respiratory disease were at greater risk of SSI (RR 1.93; 95% CI 1.04–3.24 and RR 2.18; 95% CI, 1.08–4.52, respectively) (Table 4). After multivariable adjustment, only the percentage of inspired oxygen and respiratory disease were associated significantly with the risk of infection. After adjustment for all covariables, the risk of SSI was reduced 48% in patients assigned to 80% oxygen (RR 0.51; 95% CI 0.28–1.08; p < 0.05). Patients with respiratory disease had a 3.16-fold (95% CI 2.06–8.70) greater probability of SSI (Table 4).
Fifteen patients had to be admitted to the intensive care unit immediately after the operation because of post-operative complications. Six patients (2.5%) died during the study period. The mortality rate associated with sepsis was 50% (three of six). Two of these patients were assigned to the 30% oxygen group and one to the 80% oxygen group. Three patients (50%) died of cardiovascular disease (myocardial infarction and pulmonary embolism). Two of these patients were assigned to the 30% oxygen group (myocardial infarction) and one to the 80% oxygen group (pulmonary embolism).
Discussion
Surgical site infection constitutes a substantial problem after elective and emergency operations and is the most common nosocomial infection in the surgical patient [20]. These infections are associated with significant attributable morbidity and mortality rates, prolonged hospital stays [1], and a high cost to the patient and institution. In clean-contaminated and contaminated surgery, such as elective major colorectal surgery and peritonitis, the reported risk of SSI is high [3].
Prevention of SSI is essential. Oxidative killing by neutrophils represents a major defense against SSI [25]. Such killing is enhanced by high oxygen tension in the tissue, which reduces the risk of SSI [6]. Perioperative supplemental oxygenation to increase oxygen partial pressure in tissues has been studied as a means to reduce SSI.
Two trials have suggested that high (80%) F
To date, there are five meta-analysis published that collate the effect of supplemental peri-operative oxygen on SSI after colorectal surgery [28–32]. Chura et al. [28], Al-Niaimi et al. [30], and Qadan et al. [32] affirmed that a high concentration of supplemental oxygen peri-operatively is associated with a lower risk of SSI in patients undergoing colorectal surgery, whereas Brar et al. [29] concluded that a high peri-operative oxygen fraction does not significantly reduce SSI in colorectal surgery. In a recent meta-analysis, Togioka et al. [31] affirmed that high inspired oxygen therapy peri-operatively was not beneficial for preventing SSI, whereas the positive results of two subgroup analyses (general anesthesia and colorectal surgery) suggested a benefit for hyperoxia in decreasing SSIs.
The reasons for such controversial data most likely are multifactorial. The use of different SSI definitions may be responsible for such discrepancy to some extent [33]. Another aspect is the interplay of different factors needed for site healing, such as normothermia and adequate fluid supply. Without strict adherence to the optimal peri-operative protocol, vasoconstriction may ensue and reduce the effect of tissue oxygenation [34]. Standard methods of post-operative care also are important [28]. Statistical considerations such as power calculation for sample size also can affect the data interpretation [32].
In our opinion, the most important factor in the disparate results is the heterogeneity of the study populations [13], including mixed types of diseases and operative procedures (gastrointestinal, gynecologic, and even colorectal surgery), which are associated with various types of peri-operative anesthesia care [27]. Our study population was relatively homogeneous in contrast to the recently published randomized, controlled studies dealing with supplemental oxygen and SSI, as it included a single diagnosis (PPU), one type of operation (open closure of perforated ulcer with sutures alone or in combination with an omental patch), uniformity of the surgical incision (upper abdominal midline), and age, gender, BMI, American Society of Anesthesiologists grade, and risk of infection (NNISS and SENIC scales) (see Table 1).
The trial required 10 years to accrue sufficient patients, but during this period, there were no changes in patient care, either peri-operatively (supportive treatment was the same for all patients) or operatively (closure of the ulcers was achieved by suture alone or in combination with an omental patch). Moreover, the patients were randomized in blocks. Therefore, we believe our results are devoid of patient bias.
In our randomized trial of 80% vs. 30% inspired supplemental oxygen in the intra-operative and post-operative period (6 h after surgery), we found that 80% supplemental oxygen reduced the risk of SSI by 39%. When controlling for multiple contributing factors, the reduction in SSI risk associated with 80% F
All surgical incisions become contaminated to some degree. The primary determinant of whether contamination becomes a clinical infection is host defenses. Such defenses are most critical during a decisive period lasting a few hours after contamination. For example, antibiotics ameliorate infections, and hypoperfusion aggravates infections, only during the first few hours after contamination [36]. The decisive period for oxygen remains unknown but may be for longer than for antibiotics. There were various reasons for administering oxygen for 6 h after surgery in this study. It was known from previous studies that the relative anastomotic ischemia is transitory [37,38], being limited to the first 24 h after surgery. Patients may tolerate a mask that delivers a high oxygen concentration for a few hours after surgery, but such a concentration would be difficult to maintain for longer periods owing to patient discomfort; for this reason, the supplemental oxygen therapy was restricted to 6 h after surgery [39–41]. García-Botello et al. [41] have demonstrated that there are substantial differences in anastomotic pH between the 30-min and six-h readings but not between the 6- and 24-h readings, confirming that there is a relatively transitory post-operative anastomotic hypoperfusion within the first 6 h. Clinically reversible manifestations and physiological changes to breathing 100% oxygen appear after at least 6 to 24 h [42–45], with more severe changes after 30 h. Our patients were maintained at the designated oxygen concentration during surgery and for 6 h post-operatively. There were no complications observed in our study that could be attributed to the administration of 80% oxygen for 6 h after operation. In contrast, Greif et al. [9] provided supplemental oxygen for only 2 h post-operatively. However, the results were nearly identical, which suggests that 2 h may be sufficient. Only a direct comparison in a single study will identify the optimal post-operative duration of supplemental oxygen therapy. Moreover, oxygen improves immune function [46] and is an important factor for eradication of infection. Studies using experimental incision models have demonstrated that Pseudomonas aeruginosa, Staphylococcus aureus, and Escherichia coli injected into surgical incisions can be eradicated at rates proportional to the F
Conclusions
Supplemental 80% F
Author Disclosure Statement
No competing financial interests exist.