
Abstract
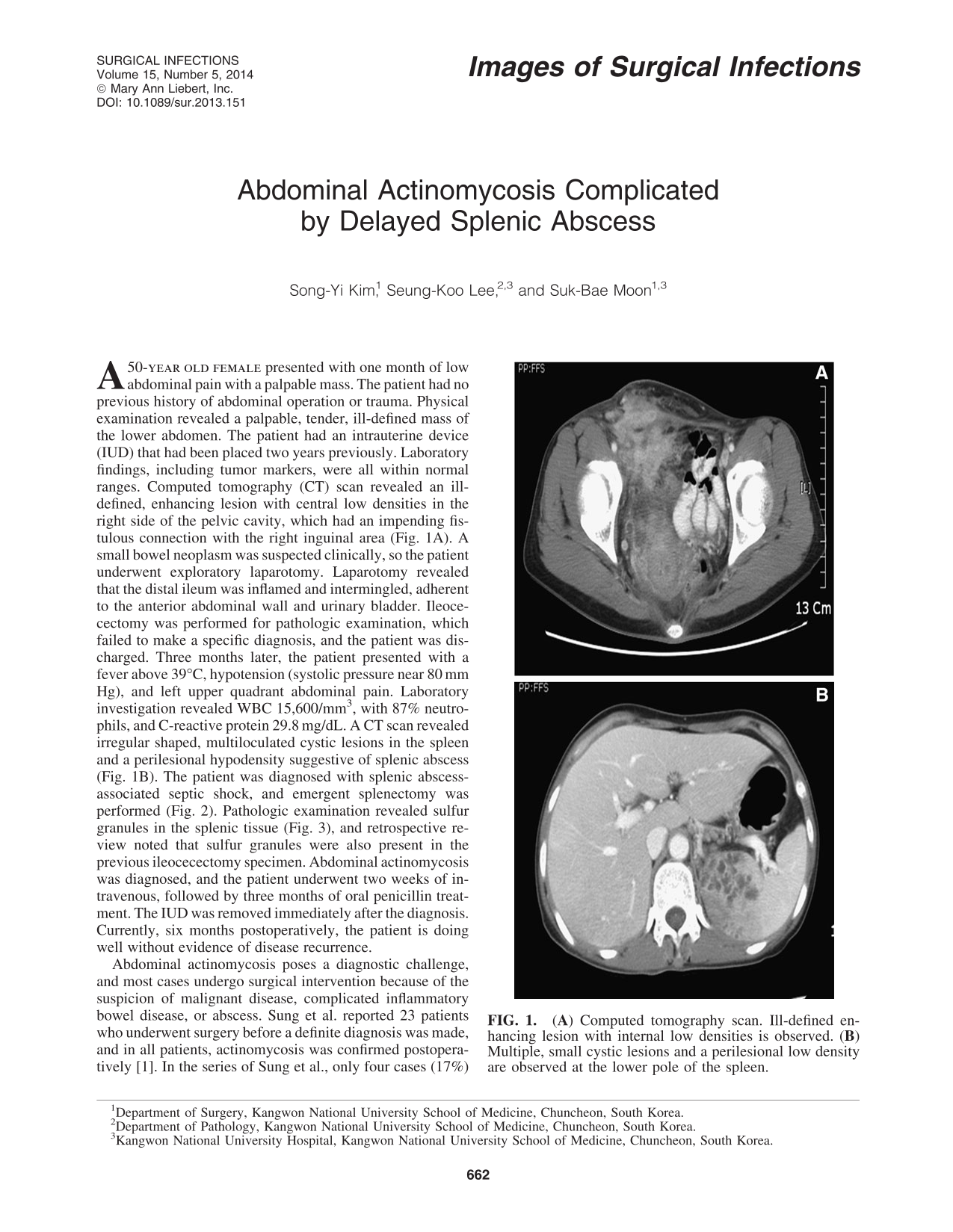
A 50-

(

Surgical specimen. Multiple abscess cavities are noted on section.
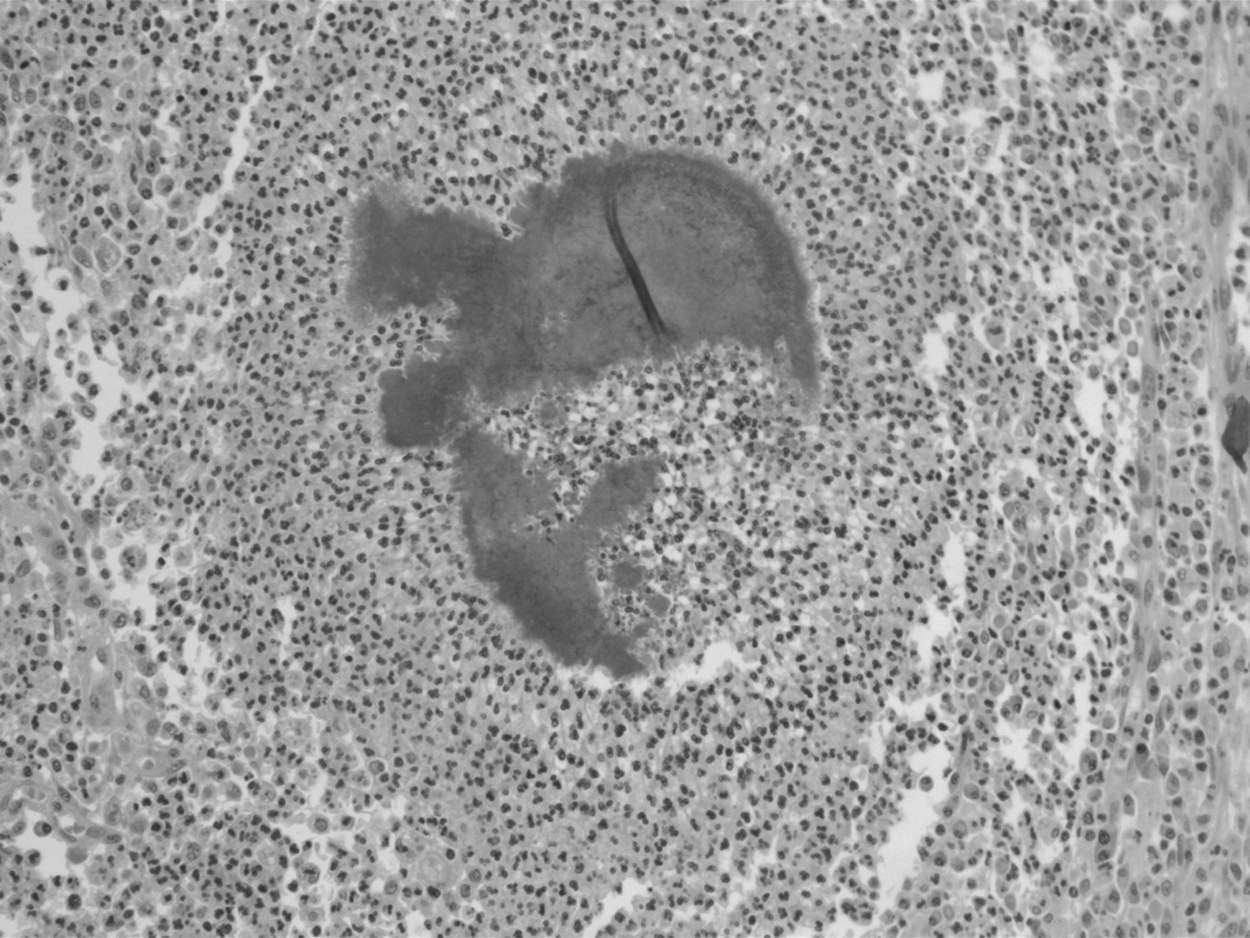
Sulfur granule (H&E, x200). Branched, filamentous bacteria in sulfur granules and surrounding inflammatory cells are observed in the abscess.
Abdominal actinomycosis poses a diagnostic challenge, and most cases undergo surgical intervention because of the suspicion of malignant disease, complicated inflammatory bowel disease, or abscess. Sung et al. reported 23 patients who underwent surgery before a definite diagnosis was made, and in all patients, actinomycosis was confirmed postoperatively [1]. In the series of Sung et al., only four cases (17%) were presumed to be actinomycosis before surgery, and the literature also shows that the diagnosis is made preoperatively in fewer than 10% of patients [1,2]. Because medical therapy alone or surgical drainage and antibiotic treatment is often curative [3], one should suspect actinomycosis in relevant clinical settings and diagnose it via the least invasive method to avoid unnecessary surgery. Splenic actinomycosis has been known to occur more often in immunocompromised patients, and the hematogenous seeding of actinomyces is believed to be a possible mechanism of microorganism inoculation to the spleen. By contrast, the lung and liver are two of the organs affected most commonly from hematogenous dissemination of actinomycosis in immunocompetent patients [4]. In this patient, although she was not immunocompromised, prolonged exposure to untreated abdominal actinomycosis might have facilitated blood stream infection and the resultant splenic abscess. However, we could not find any relevant explanation for splenic actinomycosis rather than lung or liver involvement. Timely diagnosis and prompt initiation of medical treatment would have prevented this late complication.
Surgery is a valuable tool for the definitive diagnosis and treatment of actinomycosis, and combined medical-surgical therapy has been advocated. However, an increasing body of literature supports the approach of attempting initial cure with medical therapy alone and reserving surgery for refractory cases [5]. All of the cases of splenic actinomycosis in the English literature (except one) were treated with splenectomy after failure of a short course of medical treatment. There have been debates on post-splenectomy therapeutic regimens, but a course of intravenous penicillin for two to six weeks followed by oral penicillin for 6–12 mos is accepted generally [5].