
Abstract
Abstract
Background:
Haemophilus species bacteria (HSB) are known pathogens responsible for early pneumonia in intubated trauma patients. The primary goal of this study was to examine the incidence and extent of hypoxemia in intubated trauma patients who develop early ventilator-associated pneumonia (VAP) secondary to HSB. On the basis of our clinical experiences, we hypothesized that patients with Haemophilus species bacteria pneumonia (HSBP) would have a high rate of hypoxemia but that the effect would be transient.
Methods:
Retrospective review of intubated trauma patients from an urban level I trauma center with HSBP diagnosed by deep tracheal aspirate or bronchoalveolar lavage from April 2007 to November 2012. Collected variables included day of HSBP diagnosis; PaO2 to FIO2 ratio (P:F) at HSBP diagnosis as well as HSBP day three and HSBP day seven; injury severity score (ISS) and its component parts; admission Glasgow Coma Scale (GCS) score; and mortality. Hypoxemia was defined as P:F <200. χ2 Tests were utilized to assess factors that differed between hypoxemic and non-hypoxemic patients; data are presented as median (interquartile range, IQR).
Conclusion:
Haemophilus species bacteria pneumonia in trauma patients is associated with high rates of transient hypoxemia and a high tracheostomy rate, although subsequent outcomes are not affected. Patients with head injuries had a lower incidence of hypoxemia from pneumonia.
H
Haemophilus species bacteria have also been described as potential pathogens in early pneumonia in trauma patients [8,9]. Although these pathogens are usually eradicated easily with antibiotic therapy, our group has observed that the associated pneumonia often manifests with severe hypoxemia. The primary goal of this study was to examine the incidence and extent of hypoxemia in intubated trauma patients who develop early ventilator-associated pneumonia secondary to HSB. Second, we describe the evolution of hypoxemia over time among this patient population, identify potential risk factors, and describe secondary outcomes such as tracheostomy rates, development of secondary nosocomial pneumonias, ventilator days, and mortality. On the basis of our clinical experiences, we hypothesized that patients with Haemophilus species bacteria pneumonia (HSBP) would have a high rate of hypoxemia but that the effect would be transient.
Patients and Methods
We identified patients admitted to the surgical-trauma intensive care unit in an urban level I trauma center, utilizing a database maintained prospectively at the University Hospital in Newark, New Jersey. We selected all intubated trauma patients with pneumonia due to Haemophilus spp. bacteria from April 2007 to November 2012. Patients were included in the study if they were older than 18 y of age. Additional patient demographics and trauma data including injury severity scale (ISS) and the associated body region Abbreviated Injury Scales (AIS), location of intubation (field versus hospital), admission Glascow Coma Scale (GCS) score, antibiotic administration, and blood transfusions were collected via chart review as well as by extraction from the institutional trauma registry database. Intensive care unit and hospital length of stay, tracheostomy, development of secondary pneumonia, and mortality were extracted as clinical outcomes of interest.
Pneumonia was diagnosed with quantitative cultures obtained via bronchoscopic bronchoalveolar lavage. A small subset of patients was unable to undergo bronchoscopy secondary to elevated intra-cranial pressure, small-diameter endotracheal tubes, or severe hypoxemia; these patients underwent blind bronchoalveolar lavage or endotracheal aspirate for specimen collection. Qualitative cultures were performed on endotracheal aspirates. Bronchoalveolar lavage specimens with more than 104 colony-forming units per milliliter or moderate growth of HSB with few epithelial cells on qualitative cultures were considered to be HSBP. In order to describe the extent of respiratory dysfunction, data from arterial blood gases and fraction of inspired oxygen were collected from the patient chart. The ratio of arterial oxygen concentration to the fraction of inspired oxygen (P:F) were recorded from the day of HSBP diagnosis, 3 d post-HSBP diagnosis, and 7 d post-HSBP diagnosis. A P:F<200 was classified as hypoxemia.
Data are presented as median (interquartile range, IQR) for ordinal variables and percentages for categorical variables. Analysis was performed to determine if any factors were associated with the development of hypoxemia; additional analysis was performed to determine if the development of hypoxemia had an association with adverse outcomes. Because of non-normal distribution of data, non-parametric rank tests (Mann-Whitney U, Wilcoxon rank-sum) were utilized to assess differences between groups. Chi-square tests were used to assess categorical variables; this was replaced by a Fisher exact test if any group was expected to number less than five subjects; p<0.05 was considered significant. All data were analyzed using STATA/IC, version 11.0 (StataCorp, College Station, TX).
Results
Sixty-nine intubated trauma patients with HSBP were identified; 80% of these patients were male, with a median age of 36 y (IQR 24–49). This included 60 cases of H. influenzae, 8 cases of H. parainfluenzae, and one case of H. parahaemolyticus. Thirty-two percent of the pneumonias were polymicrobial. The median day of HSBP diagnosis was hospital day 4 (IQR 3–5), with the latest diagnosis occurring on hospital day 13. All HSBPs occurred as a patient's first episode of pneumonia; no cases of HSBP were identified in patients who had been previously treated for pneumonia.
Additional descriptive data characterizing our patient population are given in Table 1. The majority of these patients had sustained a blunt mechanism trauma (73%) and 12 patients (21%) were intubated prior to arrival at the hospital; the other intubations occurred in the emergency department, operating room, or intensive care unit. Our patients had a median ISS of 27 points (IQR 9–59). The most common body systems injured were the head and chest.
Values are presented as median (IQR), unless noted.
IQR=interquartile range; VAP=ventilator-associated pneumonia; P:F=PaO2 to FIO2 ratio; AIS=Abbreviated Injury Scales.
The median P:F ratio at the time of pneumonia diagnosis was 214 (IQR 156–300); 43% of patients had a P:F <200, meeting the criteria for hypoxemia. By 3 d after HSBP diagnosis, the median P:F was 245 (IQR 198–352), with 26% of patients meeting criteria for hypoxemia. At day three, patients who had hypoxemia at presentation of pneumonia had similar P:F as the patients who did not have hypoxemia at presentation (p>0.05, Fig. 1). Seven days after HSBP diagnosis, the median P:F was 243 (IQR 186–297), and 30% of patients met criteria for hypoxemia. Forty patients (77%) eventually required a tracheostomy.
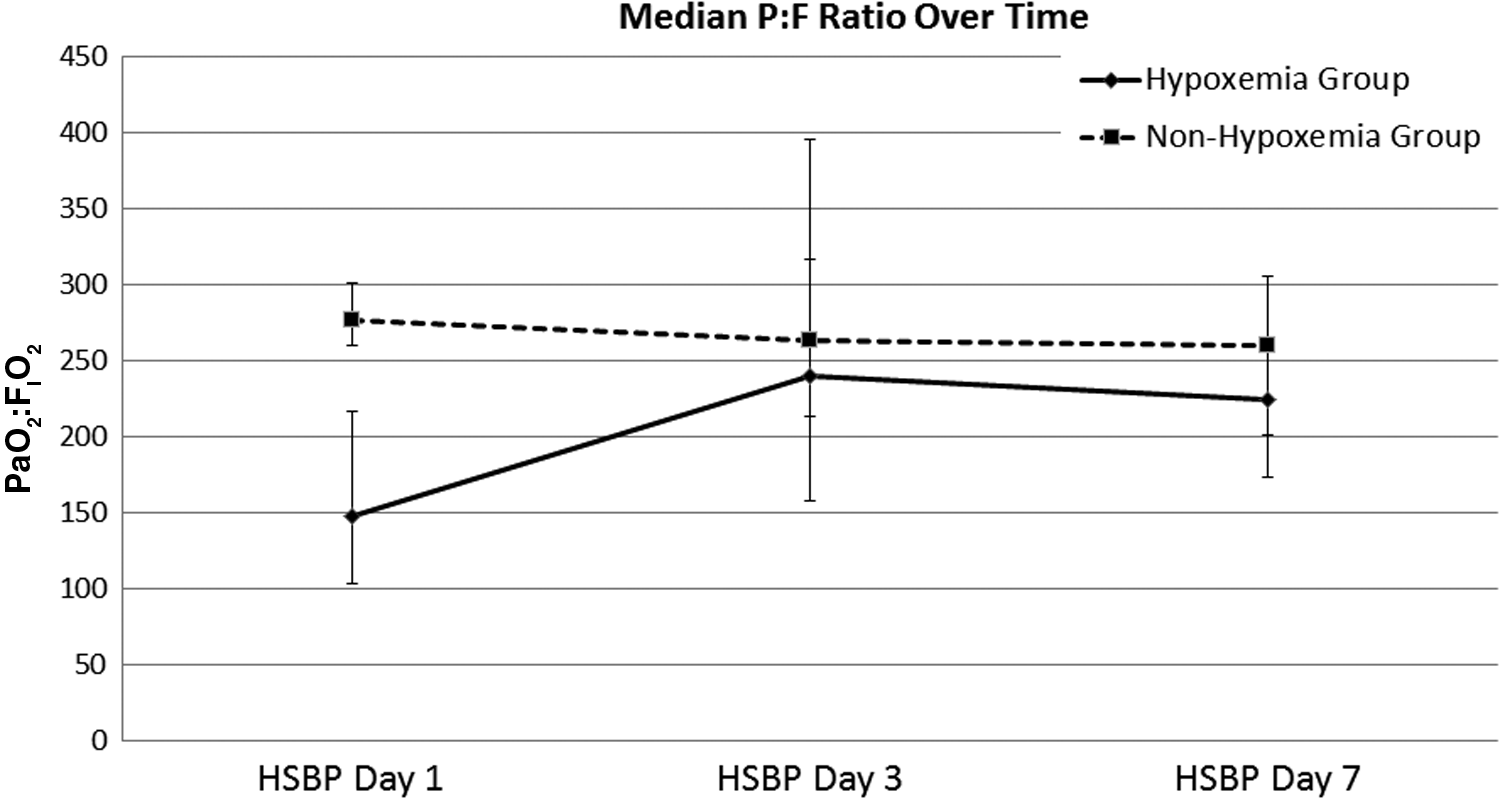
Average P:F over time, by hypoxia group. HSBP=Haemophilus species bacteria pneumonia; P:F=PaO2:FIO2, in mm Hg; Hypoxemia group=Patients with P:F less than 200 at diagnosis of pneumonia. Error bars indicate interquartile range.
Factors associated with the presence of hypoxemia at the time of HSB pneumonia diagnosis are presented in Table 2. Patients with hypoxemia at the time of diagnosis were less likely to be intubated in the field, had a higher GCS score on arrival, and a lower head AIS. In our patient population, patients with a severe head injury (GCS<9) were significantly less likely to develop hypoxemia from pneumonia (p=0.003). Similarly, patients who required a neurosurgical procedure (craniotomy, craniectomy, or placement of an intra-cranial pressure monitor) were less likely less likely to develop hypoxemia (p=0.007). We found that at least one dose of antibiotics were administered prior to HSBP diagnosis in 79% of hypoxemic patients and 77% of the non-hypoxemia group (p=0.78).
Hypoxemia defined as PaO2:FIO2<200.
Values are presented as Median (IQR), unless noted. p values determined by two-sample Wilcoxon rank-sum (Mann-Whitney U) test for ordinal variables and Fisher exact test for categorical variables.
AIS=Abbreviated Injury Scales.
Clinical outcomes such as development of a subsequent pneumonia, hospital and intensive care unit length of stay, tracheostomy, and mortality were also analyzed (Table 3). There were no significant differences in any of these clinical outcome measures between patients who had hypoxemia compared with patients who did not have hypoxemia.
Hypoxemia defined as PaO2:FIO2<200.
Values are presented as Median (IQR), unless noted. p-values determined by two-sample Wilcoxon rank-sum (Mann-Whitney U) test for ordinal variables and Fisher exact test for categorical variables.
Discussion
Most healthy adults have upper airway colonization with H. influenzae, which can serve as a potential reservoir of infection that can spread to the lower respiratory tract [10]. However, this occurs relatively infrequently in hospitalized patients, because HSB are responsible for less than 10% of all hospital-acquired pneumonia [11] and typically affects children or chronically ill patients. Among mechanically ventilated patients who develop nosocomial pneumonia, the presence of coma on admission and absence of antibiotic administration have been identified as risk factors for HSBP [12]. It is unexpected that HSB would be an important pathogen in trauma patients because they are generally healthy prior to admission. However, many basic science and clinical investigations have supported the theory that a traumatic insult leads to alteration of the host immune system [13]. Additionally, it appears that some strains of H. influenzae have a preference for damaged respiratory mucosa [10]. These processes likely allow HSB to become a pathogen in previously healthy individuals.
A few studies have noted the presence of HSB pneumonia in adult and pediatric trauma patients and suggest that it may be an important risk factor for respiratory dysfunction [8,9,14]. In one study of intubated trauma patients, the presence of H. influenzae was the sole independent risk factor for the development of acute lung injury, with a hazard ratio of 8.8 (95% confidence interval 2.7–28.6) [14]. Also, tracheal colonization with this pathogen has been associated with the eventual development of pneumonia in head trauma patients [15]. Our data demonstrate that HSB is a clinically important pathogen in early pneumonia in ventilated trauma patients and is associated with high rates of hypoxemia. In our patient population, pneumonia due to HSB tends to occur early, which suggests that the pathogen is native to the patient and becomes pathogenic after the injury. The hypoxemia improved with supportive care and antibiotic therapy, and did not have a significant effect on patient outcomes such as subsequent pneumonia, ventilator days, or mortality. Because these outcomes were rare, the lack of effect on subsequent outcomes could have been due to small sample size and a type II error. Nevertheless, our findings that hypoxemia associated with HSBP does not affect outcome is consistent with our clinical experiences treating this pathogen. Haemophilus species bacteria pneumonia is sensitive to a variety of antibiotics and easy to treat. In this population of trauma patients, the major drivers of mortality and other severe complications are likely to be factors other than their transient hypoxemia.
In our dataset, traumatic brain injuries were classified in multiple ways: Higher rate of field intubations, lower admission GCS score, higher head AIS, and more neurosurgical procedures. In the existing trauma literature, traumatic brain injuries and prehospital intubation are both independent risk factors for pneumonia, respiratory failure, and acute respiratory distress syndrome (ARDS) [16–18]. In our data, patients with traumatic brain injuries developed lower rates of hypoxemia. This was an unanticipated finding, as we expected patients with severe head injury to have more episodes of aspiration and more respiratory dysfunction. We explored several hypotheses to explain our findings. We theorized that in our series, traumatic brain injuries were associated with increased use of antibiotics that did not eradicate the infection but blunted the severity of the pneumonia and hypoxemia. In our intensive care unit, patients with an intracranial pressure monitor routinely receive narrow-spectrum antibiotic prophylaxis with nafcillin or cefuroxime. Antibiotic prophylaxis is known to alter a patient's flora to select for resistant pathogens and has been associated with the development of more severe nosocomial pneumonia [19,20]. We performed an analysis subsequently to examine the effect of antibiotic administration on the development of hypoxemia. Other than administration for intracranial pressure monitor prophylaxis, most antibiotics were administered peri-operatively for abdominal, orthopedic, or neurosurgical procedures. We found that at least one dose of antibiotics was administered in 79% of hypoxemia patients and 77% of the non-hypoxemia group (p=0.78). In our patient population, antibiotic administration was not associated with development of hypoxemia.
Several other theories could explain our findings. Our intensive care unit policy states that all patients should have the head of the bed at 30 degrees or higher as part of a standardized ventilator bundle [21]. It is conceivable that compliance with this policy is better in patients with head injuries as a part of intracranial pressure management than in patients without head injuries; this could not be corroborated with a retrospective study. Additionally, there may have been a more judicious approach to fluid administration for patients with a traumatic brain injury, allowing for less pulmonary edema and better respiratory function. It is also conceivable that brain injury leads to a protective systemic cascade to avert the development of hypoxemia. Unfortunately, the literature on this is sparse. Whereas most studies show that traumatic brain injuries increase the risk of developing pneumonia, no other study has examined the impact of brain injury on the degree of hypoxemia once pneumonia has developed.
One possible weakness of our study is that approximately 32% of the pneumonias identified were polymicrobial. Fifteen patients (22%) had two organisms isolated in culture, six patients (9%) had three organisms, and one patient had four organisms isolated in culture (1%). Other pathogens included methicillin-sensitive Staphylococcus aureus in eight patients, methicillin-resistant Staphylococcus aureus in three patients, Streptococcus pneumoniae in three patients, and viridans group streptococci in three patients. In total, 14 types of organisms other than Haemophilus were isolated in 22 patients. Twelve patients with polymicrobial pneumonias (55%) were hypoxemic at presentation, compared with 27 (57%) of monomicrobial pneumonias (p>0.05), suggesting that the hypoxemia was not related to the number of organisms isolated from culture.
In general, trauma patients have a high risk of respiratory dysfunction from a variety of etiologies, including high injury severity, advanced age, and massive transfusions [22]. We performed univariate analysis on a variety of factors and there was no significant association between hypoxemia and any of the above factors. Severe chest trauma such as pulmonary contusion [23] or multiple rib fractures [24] could also cause confounding in the data because these would be independent risk factors for hypoxia. There was no significant difference between chest AIS in the hypoxemia group and the non-hypoxemia group, and thus it is unlikely that chest trauma could have been a confounder in our data. Some variables were rare in the population (such as field intubations and mortality) and differences between groups were analyzed with the Fisher exact test; these rare events are also subject to type II error. Unfortunately, our sample was too small to perform a robust multivariable analysis on all risk factors.
In conclusion, intubated trauma patients who develop HSBP are diagnosed early in the hospital stay and develop a high rate of hypoxemia that is transient. Traumatic brain injury requiring neurosurgical intervention and a GCS less than 8 points were associated with a lower rate of hypoxemia in patients with HSBP. Hypoxemia secondary to HSBP was not associated with prolonged intensive care unit or hospital stay, subsequent development of pneumonia, increased ventilator days, or increased mortality.
Footnotes
Author Disclosure Statement
No competing financial interests exist.