
Abstract
Abstract
Background:
Surgical site infection (SSI) following joint arthroplasty increases length of stay, hospital cost, and leads to patient and healthcare provider dissatisfaction. Due to the presence of non-biologic implants (the prosthetic joint) in these procedures, infection is often devastating and treatment of the infection is more difficult. For this reason, prevention of SSI is of crucial importance in this population. Staphylococcus aureus colonizes the nares of approximately 30–40% of the population, is the most common pathogen causing SSI, and is associated with high morbidity and mortality rate. A pre-operative shower or bath with an antiseptic is an inexpensive and effective method of removal of these transient skin pathogens prior to the procedure and may be used to decrease SSI.
Hypothesis:
We hypothesize that a preoperative antiseptic shower or bath will decrease the rate of SSI.
Methods:
A retrospective review was performed at two affiliated hospitals within the same system, one with a hospital-wide policy enforcing pre-operative antiseptic shower or bath and the other with no policy, with cases included from January 2010 to June 2012. International Classification of Disease-Ninth Revision-Clinical Modification (ICD-9-CM) codes and chart review were used to identify patients undergoing joint arthroplasty and to identify those with SSI.
Results:
Two thousand three-hundred forty-nine arthroplasties were performed at the University of Minnesota Medical Center, a tertiary-care hospital with a pre-operative antiseptic shower or bath policy in place. An additional 1,693 procedures were performed at Fairview Ridges Hospital, a community hospital with no pre-operative policy. There was no difference in the rate of SSI between the two hospitals (1.96% vs. 1.95%; p=1.0). However, the rate of SSI caused by S. aureus was significantly decreased by pre-operative antiseptic shower/bath (17% vs. 61%; p=0.03), as was the rate of methicillin-resistant S. aureus (MRSA) infections (2% vs. 24% p=0.002).
Conclusions:
A pre-operative antiseptic shower and bath policy was associated with a significant decrease in S. aureus and MRSA SSI, but did not decrease the total incidence of SSI. This intervention may decrease the morbidity of S. aureus SSI in this population.
H
Staphylococcus aureus is the most common pathogen isolated from SSIs reported by the U.S. Centers for Disease Control and Prevention (CDC) [7]. In 2008 the CDC's National Healthcare Safety Network (NHSN) reported that S. aureus was isolated from 48.7% of orthopedic SSIs [7]. Staphylococcus aureus transiently colonizes the nares of 30–40% of the population and is a permanent colonizing organism in 10–20% [8,9]. S. aureus is a transient skin pathogen that is not part of the normal resident microflora, however it can pass from the nares to colonize the skin transiently [10,11]. Infection is initiated when a breach in the skin (such as a surgical incision) allows Staphylococcus aureus access to deeper tissues or the blood stream. Staphylococcus aureus is a virulent pathogen, producing enzymes that allow it to destroy tissue, facilitate spread into adjoining tissue, and promote abscess formation [10]. Foreign material, such as sutures and the prosthetic joint, allow S. aureus to adhere, forming biofilms, which decreases the number of bacteria needed to cause infection and makes eradication of the bacteria more difficult [10,12]. Staphylococcus aureus toxins lead to increased morbidity and mortality rates [10], and S. aureus drug resistance increases treatment cost and makes treatment more difficult [13,14]. Surgical site infections due to methicillin-resistant S. aureus (MRSA) are associated with greatly increased mortality, longer length of stay, and greater hospital cost [14].
Prevention of SSI following joint arthroplasty is of crucial importance, because reduction in SSI is associated with decreased hospital cost and improved patient outcomes. A pre-operative shower or bath with an antiseptic is an inexpensive method to wash away transient skin pathogens prior to an operative procedure [15], and this approach is a Category 1 recommendation (i.e., recommended strongly due to the net benefit risk profile) by the CDC for prevention of SSI [16]. We hypothesized that a policy, which enforced a pre-operative antiseptic shower or bath would be associated with a decrease in the rate of SSIs after joint replacement procedures.
Patients and Methods
After approval by our institutional review board, a retrospective review was performed of all patients undergoing hip and knee arthroplasties at two affiliated hospitals in the Fairview hospital system between January 2010 and June 2012. The University of Minnesota Medical Center (UMMC), Minneapolis, MN is an 874-bed hospital that performs 23,000 surgical procedures per year. Fairview Ridges Hospital (FRH), Burnsville, MN is a community hospital with 150 hospital beds that performs approximately 10,000 surgical cases per year. The UMMC instituted a comprehensive hospital-wide pre-operative antiseptic shower or bath policy in 1990; FRH has no such policy. The policy states that all patients (both inpatient and outpatient) are to shower or bathe with a chlorhexidine antiseptic product twice prior to the operation: the night before and the morning of the procedure. The agent is applied at full strength and the patient is instructed to clean the skin gently, rinse, dry with a freshly laundered towel, and put on freshly laundered clothing or a clean gown. At both hospitals, patients underwent standard pre-operative skin preparation with chlorhexidine-alcohol solution and the procedures were conducted using standard aseptic technique. Prophylactic antibiotic selection at both hospitals was identical and was included in computerized pre-operative orders. The primary agent is a weight-based dose of cefazolin, redosed every two hours during surgery. For patients with documented penicillin allergy, clindamycin was used as the alternative. Finally, in patients with a history of MRSA, vancomycin was used.
All patients undergoing THA or TKA at both hospitals between January 2010 and June 2012 were included in the study. International Classification of Disease-Ninth Revision-Clinical Modification (ICD-9-CM) codes were used to identify patients undergoing joint arthroplasty. Both hospitals use a protocolized SSI surveillance system to identify patients who develop SSI, with patients followed for one year post-operatively based on the CDC definition [16]. This system uses microbiology reports, physician surveys, SafetySurveillor™ (software for surveillance of infections) (Premier Inc., Charlotte, NC), referral calls from area hospitals, and ICD-9-CM codes reported by the hospital to identify SSI and other post-operative complications. SSIs were categorized as superficial incisional, deep incisional, or joint space infections.
Demographic data for all patients who developed SSI was collected for this retrospective study. This data included patient age, sex, body mass index (BMI), wound class, ASA score, procedure duration, type of anesthesia used for the procedure, the type of joint arthroplasty, and if the procedure was a revision. A surgical risk score was generated using the National Healthcare Safety Network risk score, which is a composite of ASA score, operative time, and wound class. The pathogens cultured from wounds associated with SSI were recorded for each patient. This same demographic data for all patients undergoing THA/TKA (including those that did not develop an infection) from October 2011 through June 2012 was also collected. Fairview Ridges Hospital underwent a change in electronic medical record system in 2011, and therefore, the demographic data for those patients undergoing THA/TKA prior to October 2011 that did not develop a post-operative SSI was unavailable for comparison.
Statistical analysis was performed using SPSS® version 19 (IBM Corp., Armonk, NY). Univariate analysis was performed to compare the rates of infection to demographics. Fischer exact and Chi-square tests were performed on categorical variables, and t-tests for parametric variables or Mann-Whitney U test for non-parametric variables were used for continuous variables. Logistic regression was used to perform multivariate analysis. A p value of 0.05 or less was considered significant.
Results
Over the study period, UMMC performed 2,349 total knee and hip arthroplasties, and FRH performed 1,693. Both hospitals had the same rate of total SSI over the time period of the study (1.96% vs. 1.95% p=1.0). The risk of infection at either hospital was not statistically different during any of the years studied (Fig. 1). The patient populations undergoing THA/TKA at each hospital from October 2011 through June 2012 were similar (Table 1). UMMC, which has the antiseptic pre-op shower/bath policy, did have a wider range of ages, with a lower median age than FRH. At UMMC, more patients underwent the procedure under general anesthesia, and more patients underwent hip arthroplasties. The mean procedure time was longer at UMMC (94 vs. 75 minutes; p<0.001), whereas the ASA score distribution and the median BMI were higher at FRH (29 vs. 31 p<0.001). Compliance with preoperative antiseptic shower or bath was documented in the pre-op checklist and recorded in the database during 2012 only. During this time, 75% percent of patients at UMMC had documentation regarding pre-operative shower, with 94% having used the chlorhexidine soap pre-operatively.
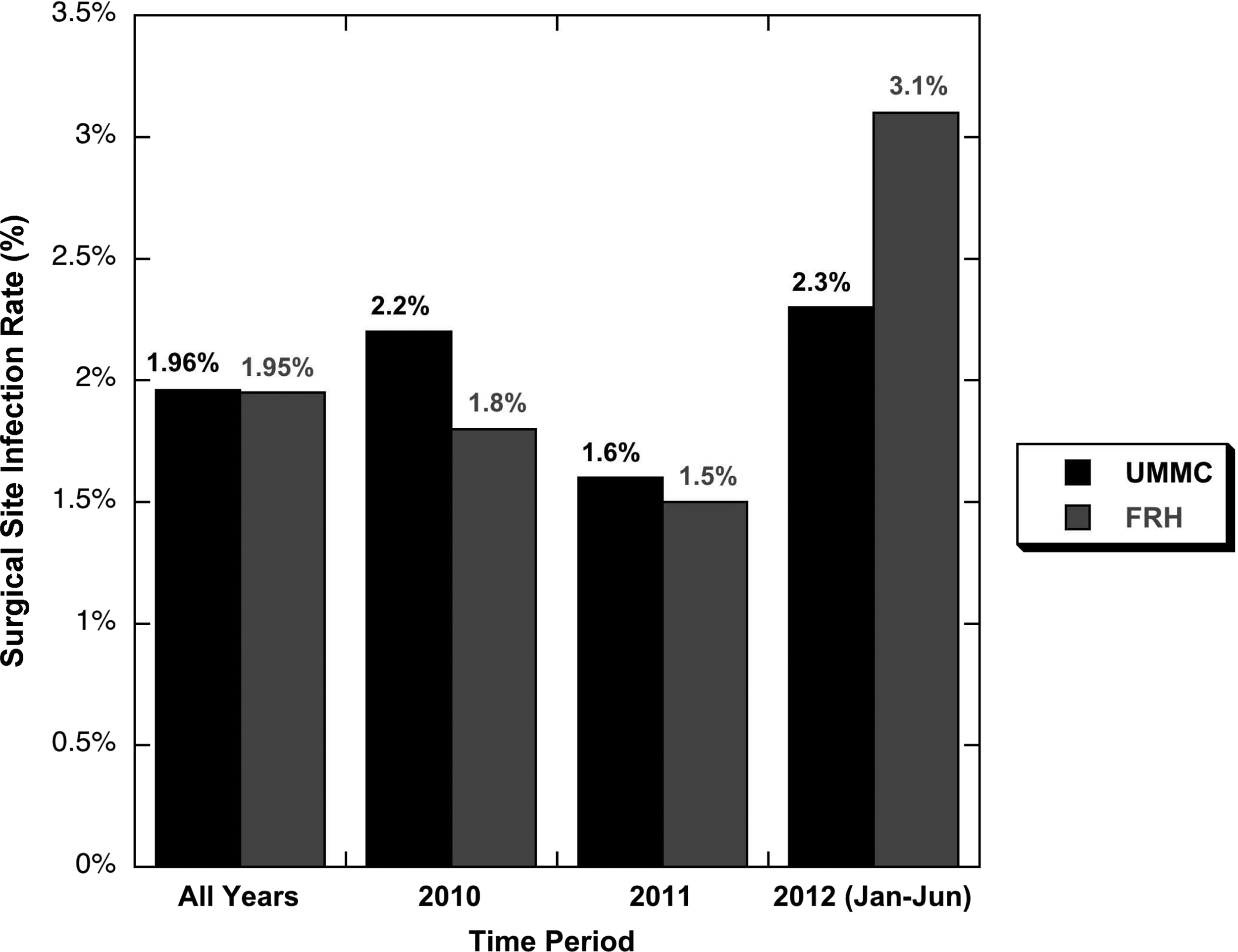
Rate of surgical site infections in patients undergoing TKA/THA in each hospital: total and per year. There is no significant difference in SSI between hospitals in any of the years evaluated (p>0.5 for each year compared).
SSI=Surgical Site Infection; BMI=Body Mass Index (kg/m2); NHSN=National Healthcare Safety Network; ASA=American Society of Anesthesiologists.
Analysis of risk factors associated with SSIs
Demographic data for patients that developed SSIs is presented in Table 2. There was no difference in median age, sex, operation performed, wound class, ASA scores, or surgical risk scores between patients that developed SSI at UMMC and FRH. There was no difference (p=0.620) in the rate of superficial incisional (22% vs. 29%), deep incisional (22% vs. 25%) and joint space SSIs (56% vs. 46%) between the hospitals. There were more patients who developed a SSI after undergoing a revision of a previous procedure at UMMC and more patients with SSI had received general anesthesia. The procedure time of patients with SSI was longer at UMMC than FRH (127 vs. 98 min; p=0.050).
NHSN=National Healthcare Safety Network; ASA=American Society of Anesthesiologists.
To identify risk factors associated with developing a post-operative SSI in our study population, we combined patients from both hospitals that underwent THA/TKA in October 2011–June 2012 and compared those that developed a SSI to those that did not develop a SSI (Table 3). Development of SSI was associated with use of general anesthesia, ASA≥3, wound class of dirty or contaminated, and surgical risk index≥2 (p<0.05). Patients with a BMI of greater than 30 had a higher rate of SSI (3.2% of obese patients developed SSI vs. 1.5% of non-obese patients; p=0.05).
BMI=Body Mass Index (kg/m2); NHSN=National Health and Safety Network; ASA=American Society of Anesthesiologists.
Analysis of risk factors for S. aureus SSI
Significantly less S. aureus was isolated from patients with SSI at UMMC with a pre-procedure shower/bath policy (17% vs. 61% p=0.03) (Fig. 2). UMMC did have higher numbers of SSI isolates of coagulase negative Staphylococcus (a resident microflora of the skin), however, there was no increase in drug resistance, virulent organisms or other transient pathogens. Table 4 compares patient variables for those that developed S. aureus SSI compared with those with other pathogens isolated. In univariate analysis, the only significant difference between patients who developed S. aureus SSI and those that did not was the hospital location, with increased S. aureus SSI associated with the hospital without an antiseptic shower policy. No other patient variables were significantly different between patients with S. aureus SSI and SSIs from other pathogens. We performed logistic regression using the variables of hospital, patient sex, revisional procedure, wound class, procedure time, and ASA score, and again found that the only variable significantly associated with risk of development of S. aureus SSI after joint replacement was the hospital at which it was performed (Table 5).

The distribution of the most common pathogens isolated from surgical site infections (SSI) at Fairview Ridges Hospital (FRH) and University of Minnesota Medical Center (UMMC). There were significantly fewer SSI due to S. aureus and Methicillin-resistant S.aureus at UMMC with a pre-operative antiseptic shower policy. There was no increase in other virulent organisms. (CoagNS: coagulase negative Staphylococcus. Other isolates not pictured, were alpha-hemolytic Streptococci, beta-hemolytic Streptococci, P. acnes, Citrobacter species, K. pneumoniae, E. cloacae, Group D Enterococcus, G. adiacens, Serratia species, and Corynebacteria.
UMMC=University of Minnesota Medical Center; FRH=Fairview Ridges Hospital; BMI=Body Mass Index (kg/m2); NHSN=National Healthcare Safety Network; ASA=American Society of Anesthesiologists.
TKA=total knee arthroplasty; THA=total hip arthroplasty; ASA=American Society of Anesthesiologists.
The only variable that was independently associated with S. aureus surgical site infection was the hospital that performed the procedure. The OR for having the procedure at fairview Ridges hospital, with no pre-operative antiseptic showers was 15.8.
The rates of both deep incisional and joint space infections due to S. aureus were significantly decreased at UMMC with the pre-procedure antiseptic shower or bath policy compared with FRH. (Deep incisional: 10% vs. 100%; p=0.0004 and Joint space: 22% vs. 60%; p=0.014 respectively). The rate of superficial infection with S. aureus was also decreased at UMMC, however this difference did not reach significance (11% vs. 30% p=0.582). Figure 3 illustrated the breakdown of superficial, deep and joint space infections due to Methicillin-sensitive S. aureus (MSSA), MRSA and other pathogens. The mean length of stay for initial infection management was longer for patients with S. aureus SSI (7.1 vs. 4.7 days, p=0.017) and 14% of patients with S. aureus SSI developed bacteremia versus 2% with other pathogens (p=0.031) (Table 5).
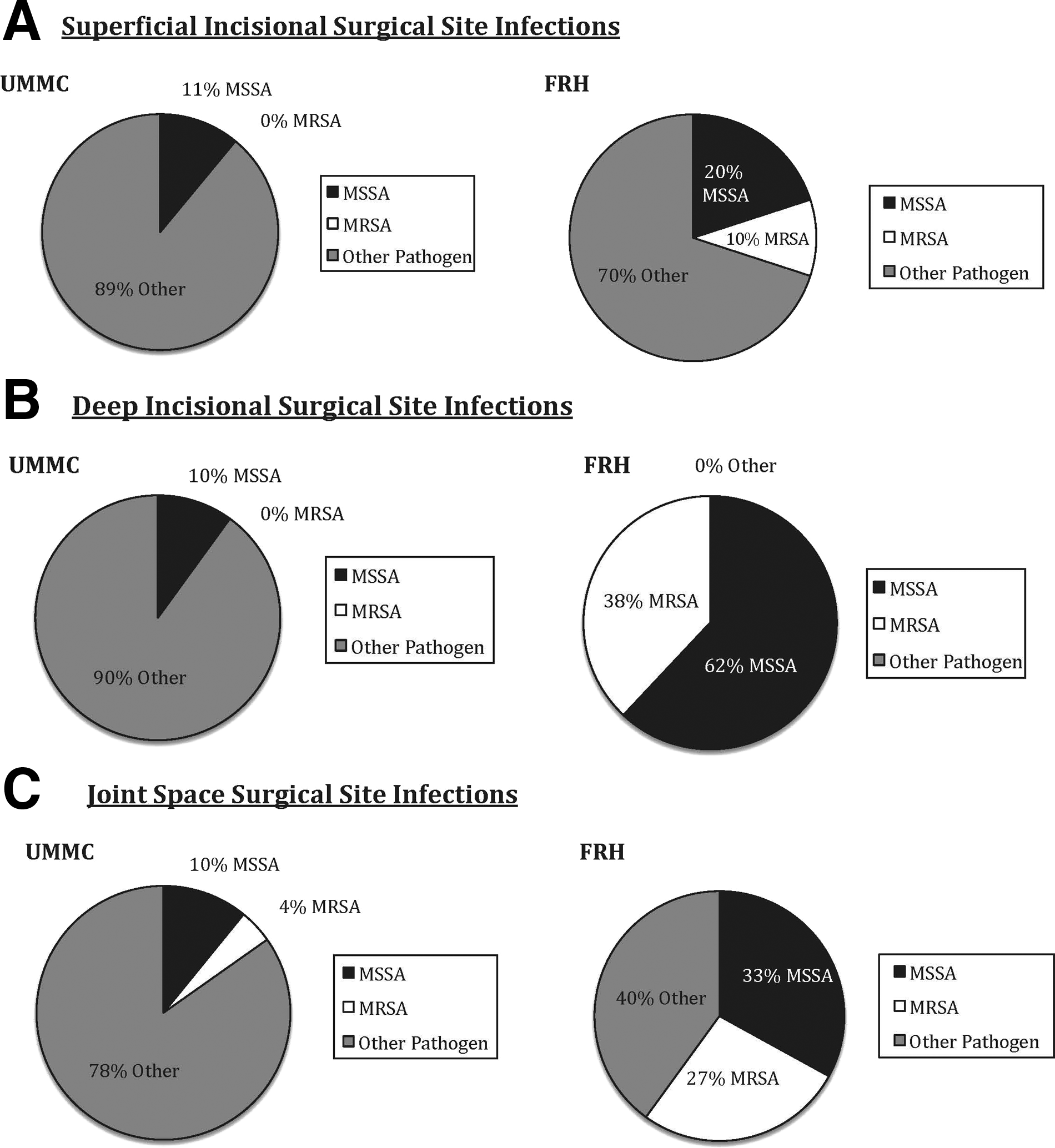
Comparison of pathogens cultured from surgical site infections (SSI) at University of Minnesota Medical Center (UMMC) with a pre-operative antiseptic shower policy and Fairview Ridges Hospital (FRH) with no preoperative antiseptic showers. Methicillin sensitive S. aureus (MSSA) and Methicillin-resistant (MRSA) S. aureus in deep incisional and joint space SSI were significantly less at UMMC with the pre-operative antiseptic showers.
The rate of MRSA SSI was significantly lower at UMMC than FRH (2.2% vs. 24% p=0.002). The rate of joint space infections with MRSA was significantly decreased at UMMC with the pre-operative antiseptic shower policy. (4% vs. 27%; p=0.047) (Figure 3). The rates of superficial incisional and deep incisional infections with MRSA were not significantly different between the two sites (0% vs. 10% p=0.211 and 4% vs. 27% p=0.069). Two of the nine patients with MRSA SSI developed bacteremia (22%) and both of these patients developed life-threatening sepsis. One of these two patients subsequently died from severe sepsis; this was the only death in our series (Table 5).
Given that the population in both hospitals has a number of patients that underwent revisions and that the population included patients that underwent revision for infection with a dirty or contaminated wound, we performed secondary analysis removing this patient population. Analysis of this subgroup did not differ from results of the entire cohort. Demographic data did not change (Supplemental data file). The rates of all SSI were similar, 1.6% at UMMC and 2.5% at FRH (p=0.297) and rates of S. aureus SSI remained significantly higher in the group at FRH than at UMMC (54% versus 19%, p=0.007). In multivariate analysis, the only independent risk factor for development of S. aureus SSI was having the procedure at FRH with no pre-operative antiseptic shower policy (adjusted odds ratio 10.6; 95% Confidence Interval 2.0–54.8; p=0.005).
Discussion
Surgical site infections are devastating post-operative complications of orthopedic procedures [3,5,6]. Recent evidence-based guidelines for prevention of SSI include appropriate pre-operative antibiotic prophylaxis, glycemic control, aseptic technique, and appropriate pre-operative skin preparation [16]. Over the past decade, significant regulatory attention has been given both to adherence to these guidelines and more recently, to reimbursement for complications [17]. Numerous recent studies show a decrease in SSI with preoperative showers or baths with chlorhexidine [18–21] with continued recommendations from the CDC for pre-operative use of antiseptic washes [16]. However, the efficacy of preoperative antiseptic baths/showers has been questioned, with several recent reviews suggesting there is no clear evidence of benefit for chlorhexidine preoperative bathing versus other wash products in decreasing the rate of SSI [22].
Our retrospective review did not demonstrate a difference in the SSI rate between the two hospitals. Independent risk factors for SSI identified in this study were obesity (BMI>30), general anesthesia, ASA score>3, wound class of III or IV, and surgical risk score>2. This is similar to the risk factors identified in other studies [23–25]. However, our retrospective review does identify a significant decrease in S. aureus and MRSA SSI after total joint arthroplasty with pre-operative antiseptic shower or bath. The only variable that was associated with this significantly decreased rate of S. aureus SSI in both univariate and multivariate analysis was having a pre-operative antiseptic shower or bath policy. Having that policy in place decreased the rate of S. aureus SSI from 61% to 17%, and decreased the rate of MRSA infections from 24% to 2%. Multiple other studies have also demonstrated this decrease in S. aureus infections (both SSIs and blood stream infections) after chlorhexidine showers or baths [13,26–28].
MSSA and MRSA were both associated with longer hospital stays and the only death in the series was following the development of severe sepsis from a MRSA SSI.
Decreasing the rate of S. aureus SSI is significant, as this pathogen has been shown to cause greater morbidity and mortality in patients, as well as increasing hospital costs when compared with other infections [6,13,26]. We demonstrated an increased length of stay and greater incidence of systemic complications of infection with S. aureus. The rates of both deep and joint space infections due to S. aureus were significantly decreased at the hospital with the pre-operative chlorhexidine policy. These deeper infections, in particular the joint space infections, cause the greatest morbidity, and frequently require at least one, if not multiple re-operations [3]. In a study done by Kurtz et al., the mean cost for treating a peri-prosthetic hip infection was $30,300 in 2009 and $24,200 for knee infections [3]. The annual cost of treatment for infected knee and hip peri-prosthetic infections and subsequent revisions was $566 million in 2009 and is projected to increase to more than one billion dollars in 2020 [3]. A chlorhexidine pre-procedure shower or bath has been demonstrated to be cost effective in the reduction of SSI in orthopedic procedures [29,30]. Kapadia et al. report the cost benefit of using chlorhexidine per 1,000 total knee arthroplasty patients was a net savings of approximately $2.1 million at their institution.
Demographics such as sex, revision rate, wound class, and surgical risk score are not significantly different between the two hospitals studied, however there were several differences noted. The University of Minnesota Medical Center is a medical school associated hospital, with greater range in age of patients and longer operative time. The larger age range and lower BMI is expected at UMMC, due to the number of pediatric and young adult cases performed there. These cases are largely performed on children and younger adults who have undergone solid organ or bone marrow transplants or have some other previous malignancy. These patients would be expected to be at greater risk than the general population for SSI. Further research would be needed to define the impact that this difference in demographics could have on the expected rate of infection at each hospital and was not the objective of this study.
We did have several limitations to our review. Due to a change in electronic medical record systems, we were unable to access demographic data from FRH in patients prior to October 2011 that did not develop SSI. This decrease in the number of available patients included in demographic analysis may have given an undue bias. However, as the rate of SSI did not significantly differ between 2010, 2011, or 2012, we are confident that this time period sample is fair representation of the general patient populations. Our patient population includes patients undergoing revisions of previous arthroplasties, as well as a small number of patients with wound classes III or IV. Both of these patient groups would be expected to have higher rates of infection, and so we also analyzed the populations excluding these “high risk” groups. Our overall results were not changed. We feel that including these higher risk patients provides our study with a broader application to diverse patient population seen at many tertiary care hospitals. Also, numerous brands of chlorhexidine wash are used at UMMC, which may also affect our data. In addition, most patients are outpatients and apply the wash themselves. Although they are instructed in correct application, it unknown how many apply it incorrectly or do not comply with the protocol. We also have limited data on compliance of patients, as this was documented in the patient chart starting in 2012 with no data prior to this. The compliance documentation is per patient report, and is subject to significant bias.
In conclusion, prevention of surgical site infection after joint replacement is of critical importance in improving patient outcomes. A pre-operative antiseptic shower or bath policy is a simple, cost-effective method to decrease S. aureus and MRSA SSI. However, there is a paucity of randomized controlled trials examining the effectiveness of this method. There are multiple patient risk factors for SSI that are out of our control, such as patient age, BMI, medical co-morbidities, and others. Therefore, the risk factors that we can control, such as appropriate antibiotic dosing, intra-operative technique and postoperative care are of even more importance. We would suggest that adding a pre-operative antiseptic shower or bath policy is an important and easily implemented additional intervention that can decrease the rate of S. aureus and MRSA SSI.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.