
Abstract

A 53-
A CT scan of the abdomen and pelvis with enteral and intravenous contrast (Fig. 1) demonstrated evidence of acute stump appendicitis with a 4-cm appendiceal remnant with radiopaque suture material at the tip. The stump was fluid-filled and dilated up to 1.5 cm with adjacent inflammatory change. Systemic antibiotics were initiated and she was admitted. Her abdominal pain improved, and she was discharged home on a course of oral antibiotics. Elective laparoscopic stump appendectomy was performed, and surgical pathology confirmed a 3-cm long, 1-cm diameter distal segment of appendix that was confirmed to be the appendiceal stump with no notable abnormality.
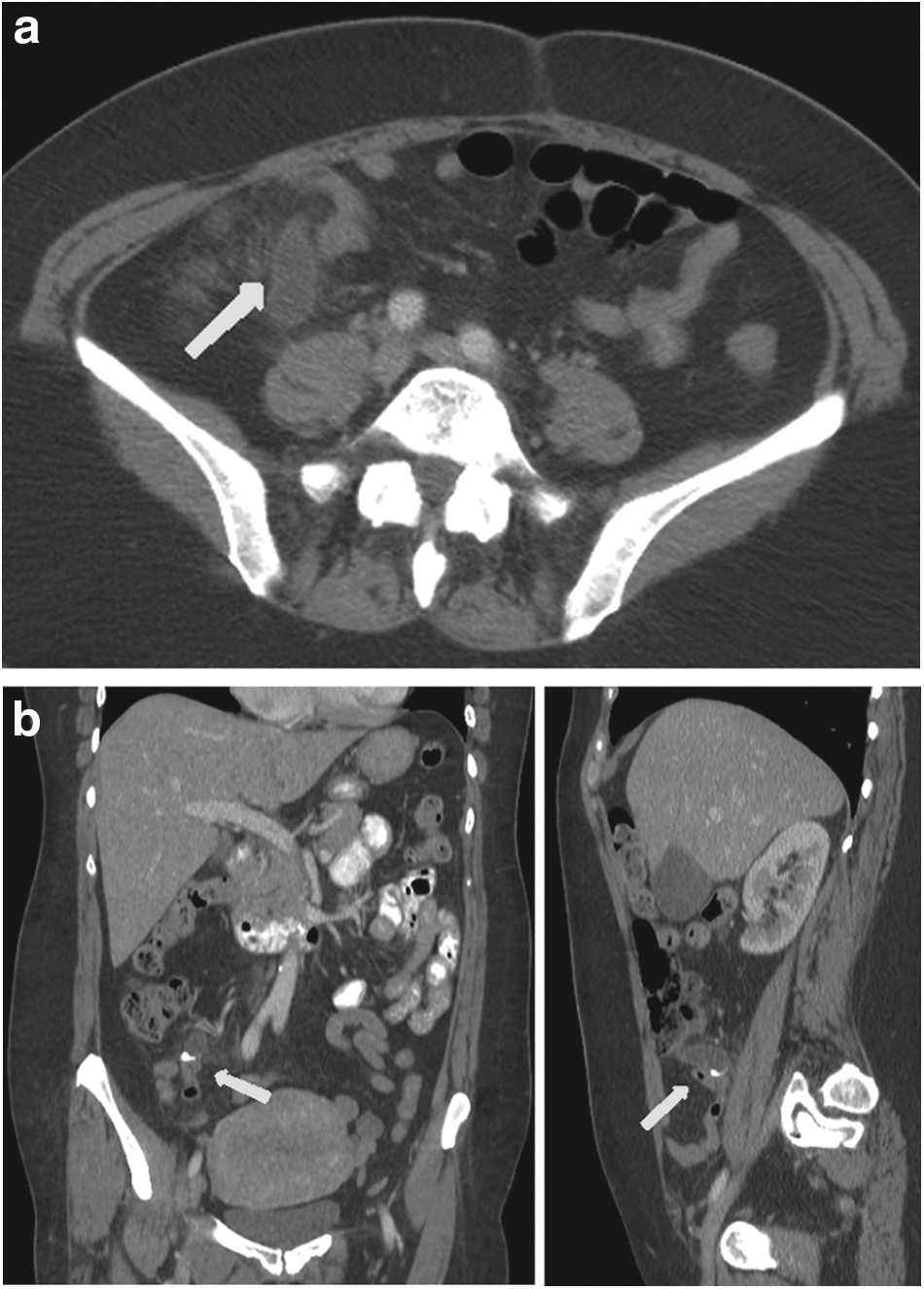
Computed tomography of abdomen, axial
Stump appendicitis is a rare entity and an uncommon late complication of appendectomy, where inflammation occurs in the remaining appendiceal stump [1]. Stump appendicitis requires early detection and diagnosis. Typically, patients present with signs and symptoms similar to acute appendicitis; however, due to prior surgery, the diagnosis is difficult and the rate of appendiceal stump perforation is high [2].
A recent systematic review identified 60 published cases of stump appendicitis, and documented that the interval from the original appendectomy ranged from 4 d to 50 y, and that perforation with gangrene of the stump occurred in 40% of cases [3]. A high level of suspicion of stump appendicitis is required in patients presenting with right lower quadrant abdominal pain and a surgical history of appendectomy, and ultrasound or computed tomography abdominal imaging is diagnostic in most cases. The main cause of stump appendicitis is the persistence of a large appendicular remnant. Treatment consists of a completion appendectomy by either a laparoscopic or open approach.
Correct identification and removal of the appendix at its base without leaving an appendiceal stump at initial appendectomy minimizes the risk of stump appendicitis [4]. To prevent stump appendicitis, some have proposed use of the “critical view” similar to that used in laparoscopic cholecystectomy. The “critical view” ensures proper identification of the entire appendix and its base, the appendix retracted to the left in the 10 o'clock position, visualization of the taenia libera in the 3 o'clock position, and confirmation of the terminal ileum at the 6 o'clock position, with transection of the appendiceal base to allow<0.5 cm appendiceal stump [5].