
Abstract
Abstract
Background:
Negative-pressure wound therapy (NPWT) has been suggetsed to have a positive impact on the healing of sternal or extremity wounds. However, few data deriving from breast surgery have been published. We evaluated the available literature regarding the effectiveness of NPWT systems in the healing of breast tissues.
Methods:
The PubMed and Scopus databases were searched systematically, and all studies that provided relevant data were considered eligible for inclusion in the review. Twenty studies (154 female patients) met the inclusion criteria (four cohort studies, one case series, and 15 case reports).
Results:
The NPWT system was used alone in 17 patients and in combination with other techniques in the remaining 137. The lesion was secondary to plastic surgery in 107 women, other operations in 40 women (38 of them for breast cancer), and primary breast infection in seven women. Infections (including necrotizing fasciitis), pyoderma gangrenosum, and necrosis were among the most common complications for which NPWT was used. In total, 150 of 154 patients receiving NPWT healed completely. Two patients died before complete closure for reasons unrelated to the wound, and NPWT failed in two patients who healed later with muscle flap coverage.
Conclusion:
The scant published evidence suggests that NPWT systems might be useful in the healing of complicated breast wounds. However, larger studies are needed to investigate the effectiveness of this system further before it is established in breast surgery.
I
The NPWT system consists of three parts: A porous foam dressing custom-prepared according to the dimensions of the wound bed, an adhesive, semi-permeable drape, which is applied on top of the foam dressing to serve as a sealant, and a track pad that is applied on top of the drape and connected via a tube to the therapy unit. The therapy system generates negative pressure that is conducted via the tube to the track pad and thence to the wound, resulting in approximation of the wound edges, aspiration of infectious debris and exudates, reduction of edema, increase in blood flow, promotion of granulation tissue generation, and, preservation of a wound-friendly moist environment [8–10]. Currently, the use of NPWT systems is indicated for a broad spectrum of acute, sub-acute, and chronic wounds, such as diabetic foot ulcers, complex venous leg ulcers, pressure ulcers, dehisced sternal incisions, open abdominal incisions, and traumatic wounds [2]. Interestingly, NPWT has been suggested to achieve faster healing in sternal, extremity, and diabetic foot sites [11–13].
Although the benefit of NPWT in the healing of open wounds is already clear in the literature, the use of this technique specifically in breast surgery is not as common as in other surgical specialties; therefore, there is minimal discussion of this issue in the literature. The large number of breast operations for cancer or aesthetic reasons, the need for impeccable technical and aesthetic outcomes, and the always-existing risk of incision breakdown necessitates the investigation for techniques that optimize wound healing and decrease complications. In this context, we reviewed systematically the available evidence for the effectiveness of NPWT in the healing of breast incisions.
Materials and Methods
Literature search
We searched systematically the PubMed and Scopus databases in October 2012. The search term applied in both databases was (vacuum-assisted closure OR negative pressure wound therapy OR NPWT) AND (breast OR plastic). The bibliographies of all eligible and potentially eligible articles were hand-searched in order to identify additional studies. Only articles written in English, French, German, Spanish, Italian, or Greek were evaluated.
Study selection
Studies reporting on the effectiveness of NPWT in the healing of breast incisions were considered eligible for the review. Studies that did not specify the area on which NPWT was applied were excluded. All types of studies, including case reports and case series, were considered eligible for inclusion.
Data extraction
The extracted data consisted of the main characteristics of the included studies (first author, country, period of the study, study design), total number of patients and number of patients having breast surgery, age, type of breast incision and incision size, management (including NPWT, surgical procedures, or antibiotics), duration of NPWT application, and the outcome of the therapy.
Definitions and outcomes
Breast sites included surgical incisions, both complicated and uncomplicated, and wounds caused by primary breast infections. The outcome of the review was the effectiveness of NPWT in the healing of breast sites.
Results
Five hundred eighty-five articles were identified during the search process (418 PubMed, 162 Scopus, five hand-searching). Twenty articles were included in the review [14–33]. The study selection process is depicted in Figure 1.
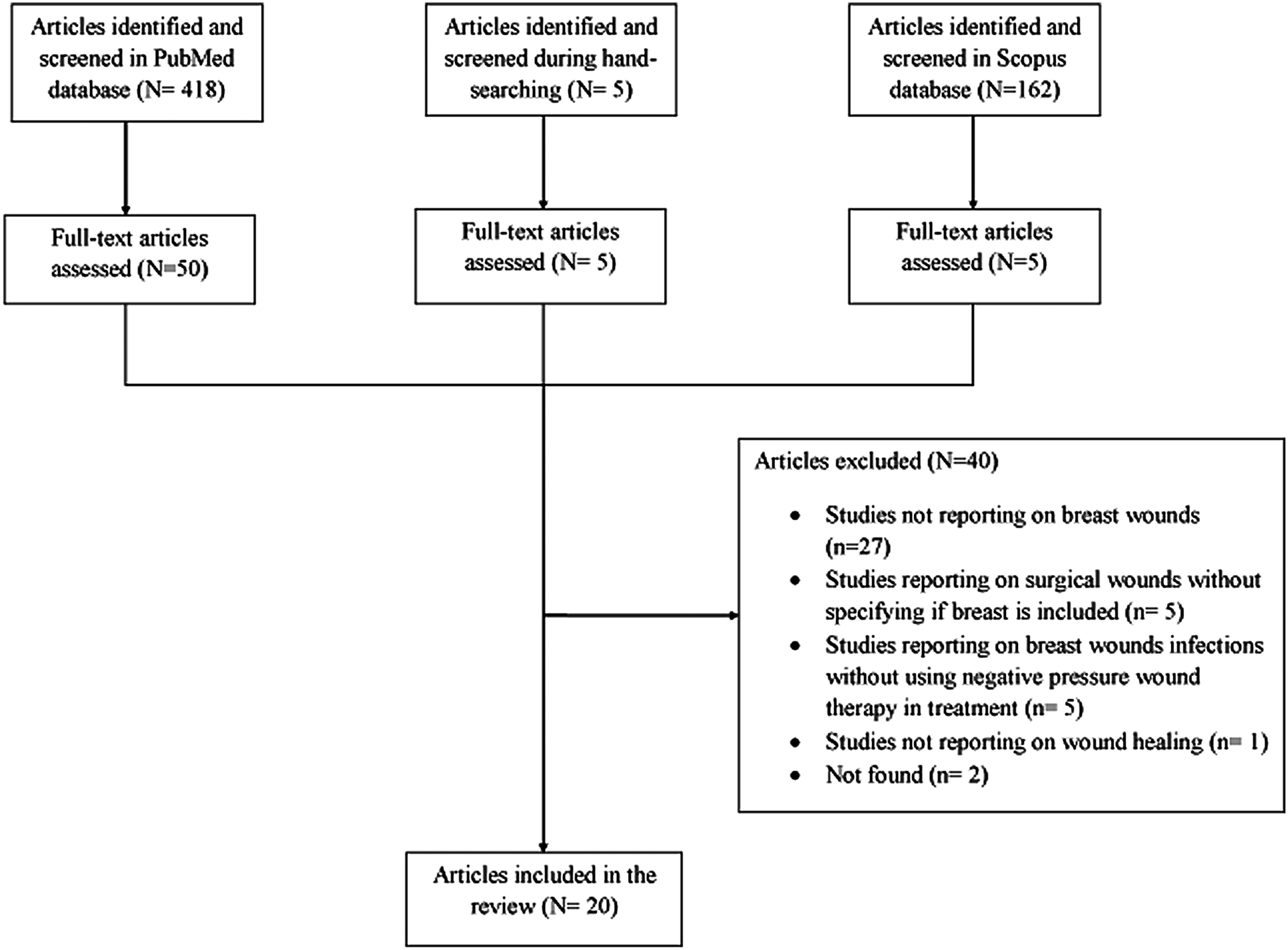
Search process and selection of articles for review.
The eligible articles comprised four cohort studies (two prospective and two retrospective) [19,31–33], one case series (including five patients) [28], and 15 case reports [14–18,20–27,29,30]. The characteristics of these studies are presented in Table 1. A total of 154 female patients are included. Of the total population, 107 had a breast incision site related to a plastic surgery procedure (96 augmentation mammoplasties, four transverse rectus abdominis myocutaneous [TRAM] flap reconstructions, four reduction mammoplasties, one bilateral inferior pedicle mammoplasty, one reconstruction with skin, and one implant rupture followed by breast rupture), whereas 40 patients had breast incisions for other surgical indications: 38 patients had breast cancer, one patient had fibrocystic mastopathy, and one had a breast biopsy. Furthermore, seven patients had been admitted for a primary breast infection, including five chronic wounds caused by non-puerperal mastitis, one primary complicated abscess, and one primary recurrent breast abscess of unknown etiology. The detailed treatments and procedures used in the patients of each study are presented in Table 1.
The antibiotics administered to each patient were the following: amoxicillin-clavulanic acid, ciprofloxacin, flucloxacillin, trimethoprim, and sulfamethoxazole; flucloxacillin, cefuroxime, and ciprofloxacin; clindamycin, cefuroxime, flucloxacillin, and ciprofloxacin; amoxicillin, ciprofloxacin, and flucloxacillin; or ciprofloxacin, flucloxacillin, clindamycin, and cefuroxime.
One patient discontinued because of insurance problems and was switched to treatment with wet-to-dry dressings.
The preliminary treatment with oxacillin was switched to piperacillin-tazobactam and vancomycin after the emergence of oxacillin-resistant strains.
Pristnamycin, cefotaxime, metronidazole, and linezolid also were administered.
The antibiotics that were administered during therapy included oral flucloxacillin and metronidazole, IV gentamicin, and linezolid.
Abbreviations: abx=antibiotics; IV=intravenous; MDR=multi-drug-resistant; NAC=nipple–areola complex; NPWT=negative pressure wound therapy; NR=not reported; PHMB=polyhexamethylene biguanide; TNP=topical negative pressure; TRAM=transverse rectus abdominis muscle; VAC=vacuum-assisted closure.
The NPWT was used to aid treatment of various complications. Three sites developed more than one complication [24,27,30]. Specifically, complications included 104 infected sites (two with necrotizing fasciitis), five site recurrences, five chronic wounds, three pyoderma gangrenosum, two site dehiscences, two seromas, one breast and implant rupture, one venous congestion of the nipple–areola complex, one heavily exuding site, 13 with necrosis (11 by radiation), and 18 complicated open breast sites.
The NPWT was used as an adjunct in all but 17 patients. In 21 cases, the NPWT system was used during or right after the surgical procedure. In the remaining cases, the NPWT was applied only when the wound was complicated. The site size differed considerably among the studies that provided relevant data, as did the duration of application of NPWT, which ranged from 72 h to a few months. Data on the precise period that was required for the healing with the use of NPWT were not provided within the studies. The non-surgical techniques used for the prevention and treatment of infections included antibiotic administration, orally or intravenously, or deposition of dressings that were impregnated with silver or polyhexamethylene biguanide.
A total of 150 out of 154 wounds healed ultimately using an NPWT system with or without other procedures. In two patients, NPWT failed because of vascular compromise, and muscle flap closure was required for definitive coverage [31]. In addition, the sites in two other patients were nearly healed after the application of NPWT, but the patients died before complete site closure for reasons unrelated to the wound [16]. Complications related to NPWT were not reported in any of the papers.
Discussion
According to the published evidence, NPWT, both alone and in combination with surgical procedures or antibiotics, might be useful in the healing of complicated breast incisions and injuries. No complications attributed to NPWT were reported in the studies we reviewed.
For the majority of the patients, NPWT was used as an adjunct and in combination with a variety of surgical techniques, including wound debridement, skin grafts, muscle/omental flaps, curettage, acellular dermal matrix, or meshes. Until now, no major failures regarding its use have been reported. On the contrary, NPWT has proved to be helpful in the healing of vulnerable breast injuries; i.e., after irradiation [19,21], as well as in sites with rare, difficult-to-treat infections [17,22,28,29].
Apart from healing, other indirect benefits arise from the use of negative pressure in the wound area. Faster healing can result in a vital acceleration of other procedures such as irradiation and chemotherapy, which commonly are required postoperatively in patients who undergo breast surgery because of cancer. In addition, NPWT can serve as a space holder and prevent the collapse of the breast envelope before reconstruction [27]. From the aesthetic point of view, it has been reported that the minimally invasive nature of the therapy aids shape preservation as well as prevention of skin retraction [17]. Furthermore, the possibility of using the NPWT system on an outpatient basis or even as home treatment [21] might have a positive impact on the psychosocial aspects of the disease, increasing the confidence and the self-esteem of the patients. The daily cost of the treatment with negative pressure is higher than the cost of conventional treatment [31], but since the healing is faster and the length of hospitalization decreases, the overall treatment cost may be reduced.
Our study should be interpreted in view of certain limitations. First and foremost, the published evidence regarding the use of NPWT in breast wounds is limited. Additionally, comparative studies between women receiving NPWT for breast wounds and those receiving non-NPWT treatments were not available, and therefore, the clear impact of the NPWT on the clinical outcomes could not be detected. Furthermore, few data were available regarding the precise reduction of the injury size after the use of the NPWT system. Yet, the authors of the included studies did not distinguish whether NPWT was applied clearly as an adjunct in healing or to avoid postoperative complications in high-risk patients (i.e., women receiving radiotherapy, or corticosteroids). Finally, the cases that were retrieved appear to be significantly heterogeneous regarding the reason for the application of the NPWT, adding to the weakness of the findings of the study, even though they do cover a wide spectrum of breast operations.
In conclusion, the limited available evidence suggests that NPWT might be effective in aiding the healing of complicated breast sites. However, larger studies investigating the effectiveness, safety, and appropriate use of negative pressure in breast surgery are needed.
Footnotes
Author Disclosure Statement
No funding was received for this work. None of the authors has any conflict of interest in relation to this study.